Concepts of growth and development II
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
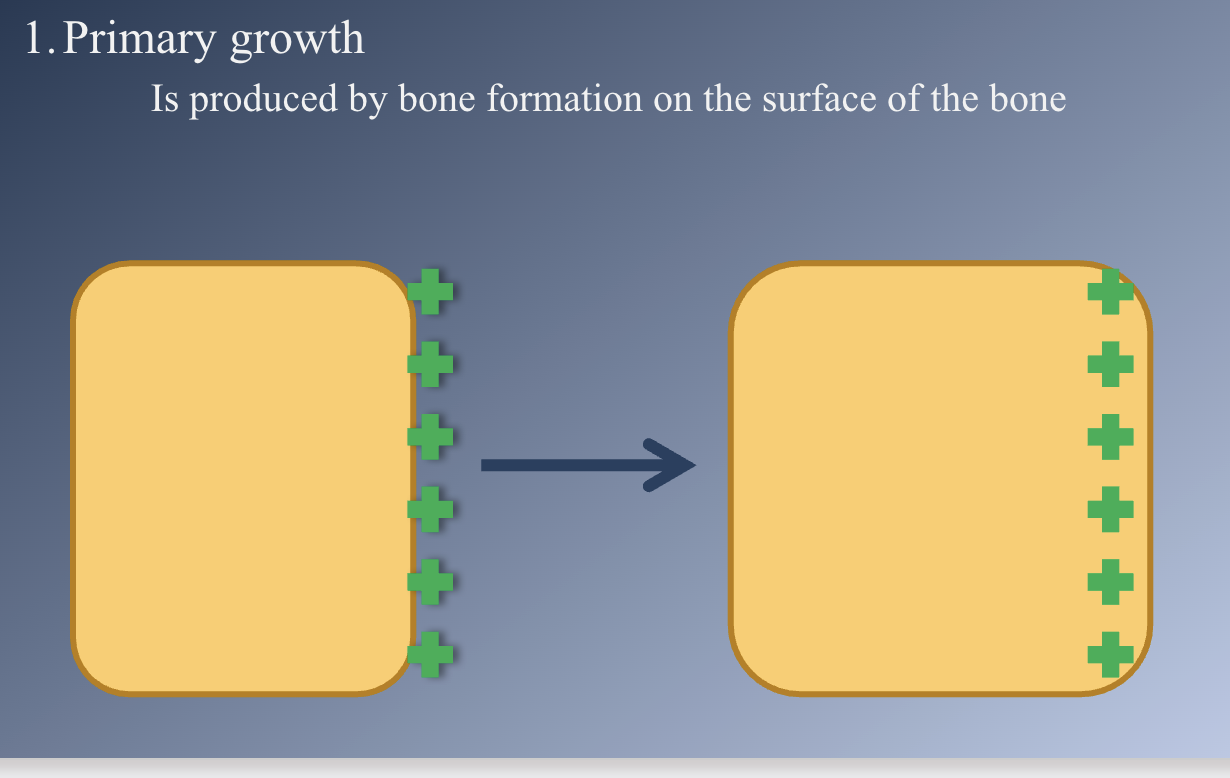
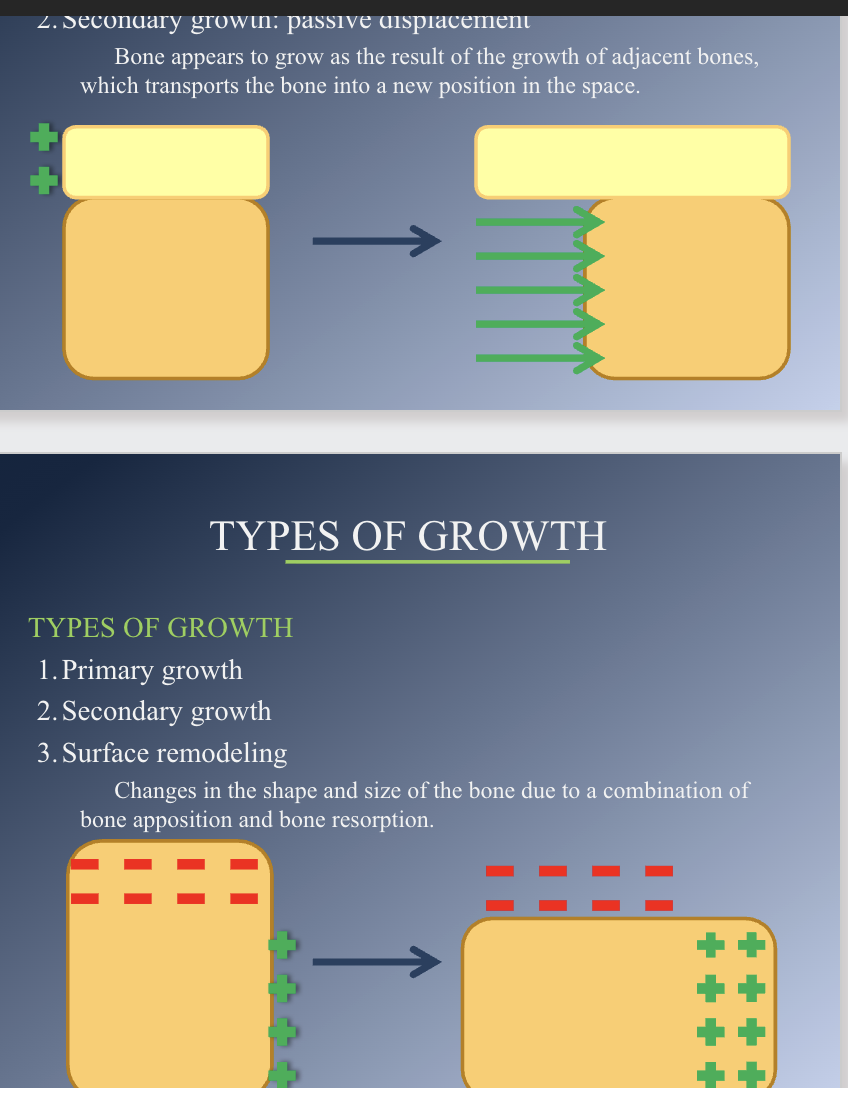
Types of growth
Primary- produced by bone formation on surface of bone
Secondary: Passive displacement. Bone appears to grow as result of the growth of adjacent bones, which transports the bone into a new position in the space.
Surface remodeling- Change in shape and size of bone due to combination of bone apposition and resorption.
Cranial vault
1. Made up of flat bones formed directly by intramembranous bone formation.
2. Remodeling and growth occur primarily at the periosteum contact areas between adjacent skull bones → CRANIAL SUTURES
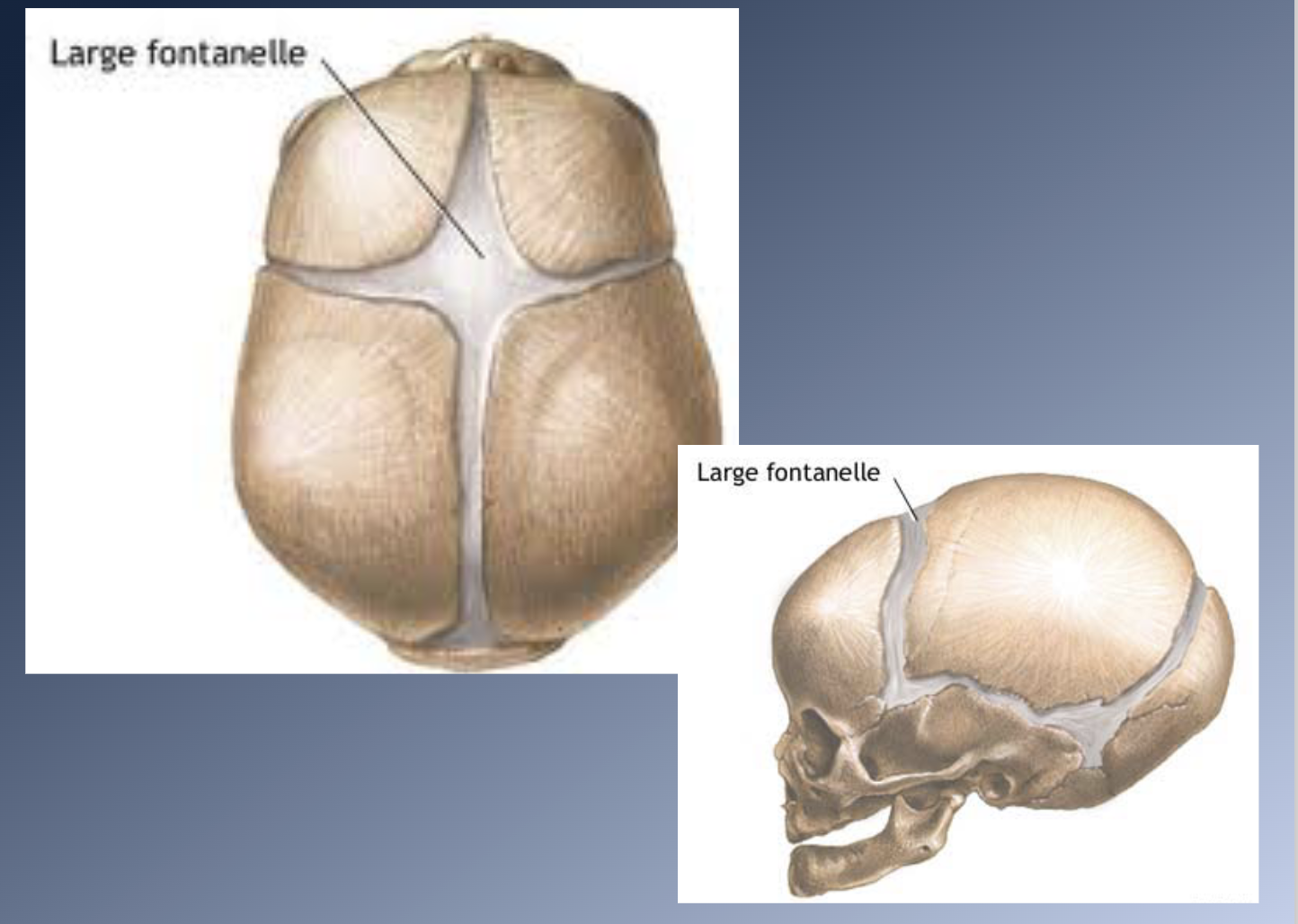
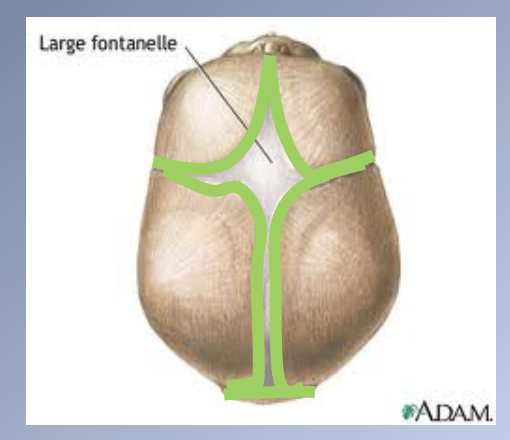
3. BIRTH:
1. Bones widely separated by loose connective tissues = FONTANELLES
2. These allow considerable deformation of the skull at birth
4. POST-NATAL GROWTH
1. Apposition of bone along the edges of the fontanelles eliminates these open spaces fairly quickly
2. Bones remain separated by a thin, periosteum-lined suture for many years
3. In adult life, these bones are fused
5. MECHANISM OF GROWTH
1. Main: apposition of new bone at these sutures
2. Remodeling allows for changes in contour during growth
- Bone removed from the inner surface of the cranial vault
- New bone is added on the exterior surface
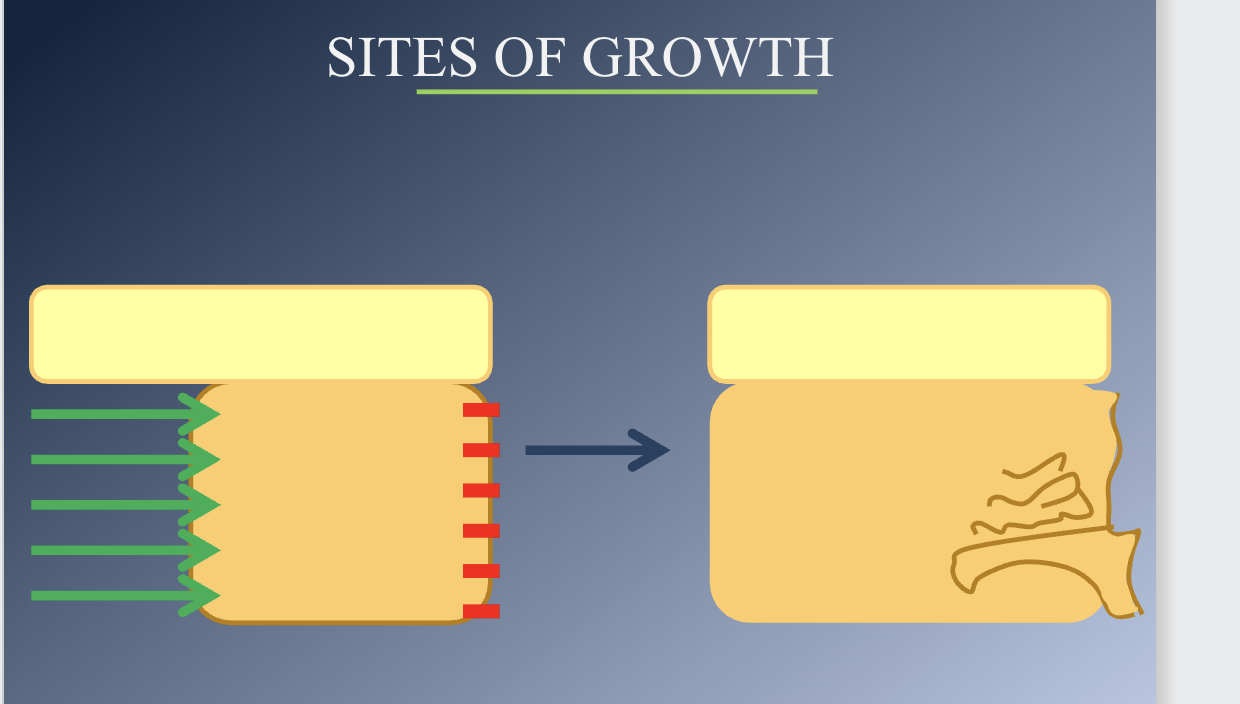
Sites of growth
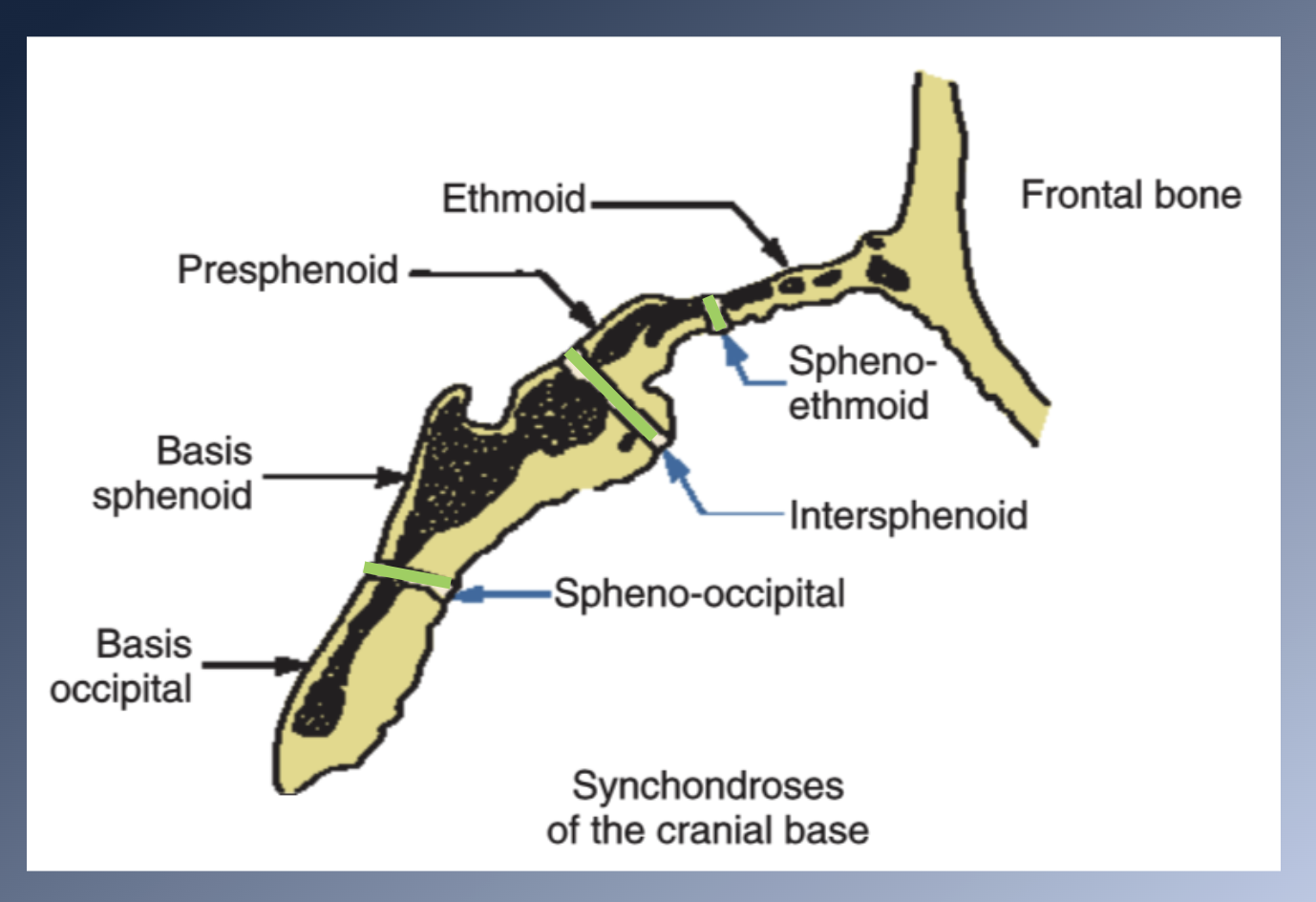
CRANIAL BASE
1. Formed initially in cartilage à endochondral ossification à
bone
2. MIDLINE STRUCTURES
3. CENTRES OF OSSIFICATION early in embryonic life in the chondro-cranium (basioccipital, sphenoid, ethmoid bones)
4. SYNCHONDROSES remain between the centres as ossification proceeds
5. Inmovable joints
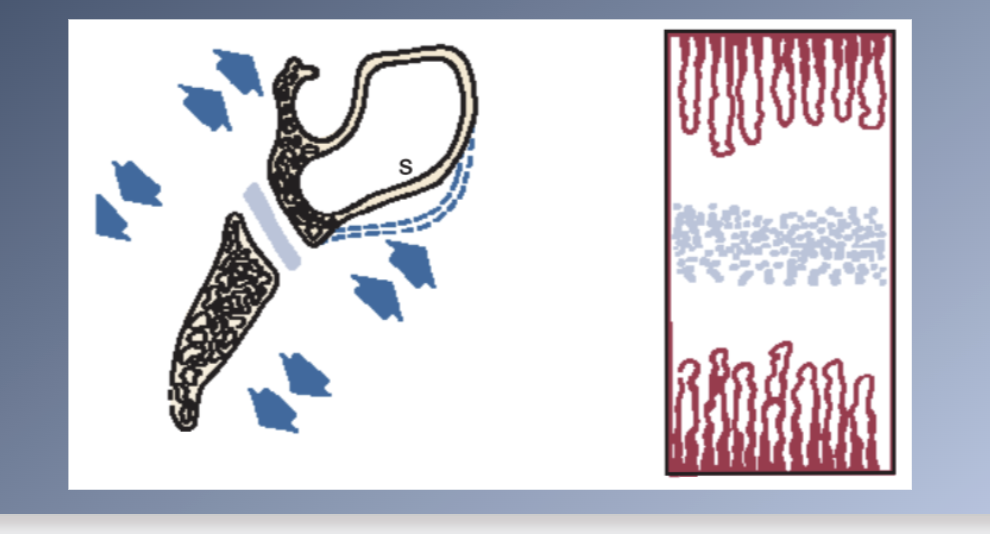
5. SYNCHONDROSES: two-sided epiphyseal plate
1. Area of cellular hyperplasia in the center
2. Bands of maturing cartilage cells extending in both directions
3. Mature cartilage is eventually replaced by bone
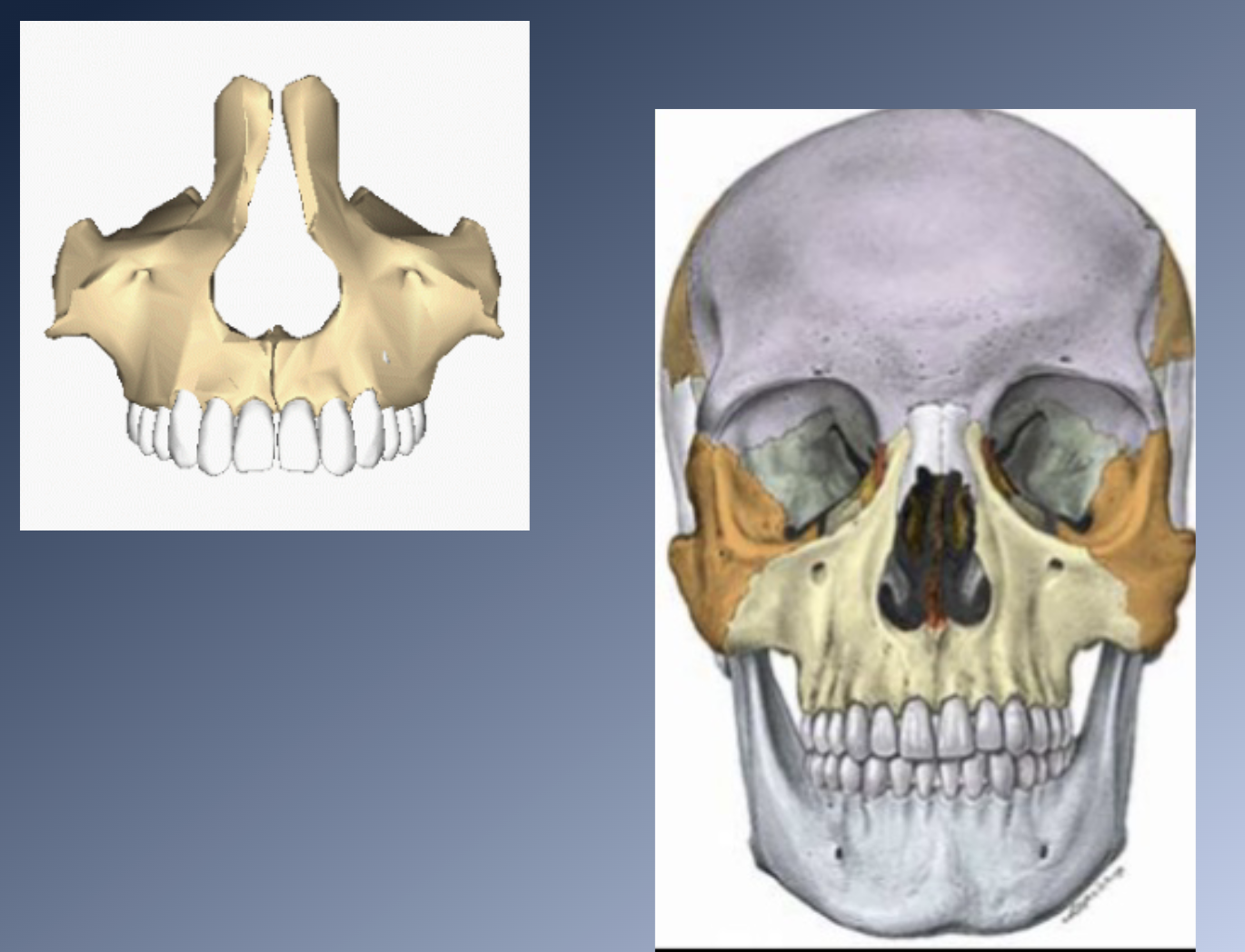
Sites of growth: Maxilla
1. EMBRYO:
• Forms initially from a center of mesenchymal condensation in the maxillary process, on the lateral surface of the nasal capsule.
. EMBRYO:
• Growth cartilage contributes to lengthening of the head and anterior displacement of the maxilla, but does not contribute directly to formation of the maxillary bone.
• Malar cartilage disappears and is TOTALLY replaced by bone well before birth.
• Bone formed entirely by APPOSITION of new bone to free surfaces.
Sites of growth: Maxilla 2
2. Postnatal development:
1. Apposition of bones at the sutures that connect the maxilla to the cranium and cranial base.
2. Surface remodeling: dramatic surface changes.
3. Moved forward by growth of the cranial base
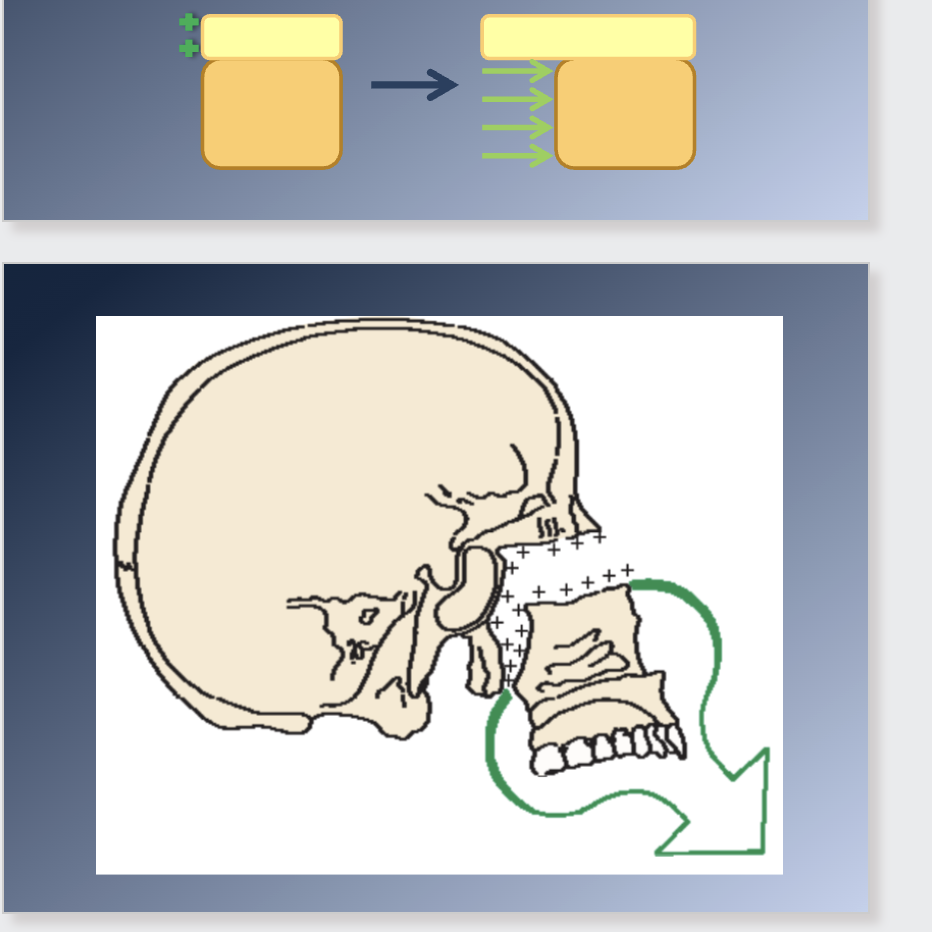
Maxilla should “grow out” from under the cranium
1. Pushed from behind by growth of the cranial base (imp. <6yr)
2. Growth at the sutures
Sutures attaching the maxilla posteriorly and superiorly are ideally situated to allow downward and forward repositioning.
1. As displacement occurs, the open space is filled in by proliferation
of bone at this locations
2. The sutures remain the same width, although they increase in length
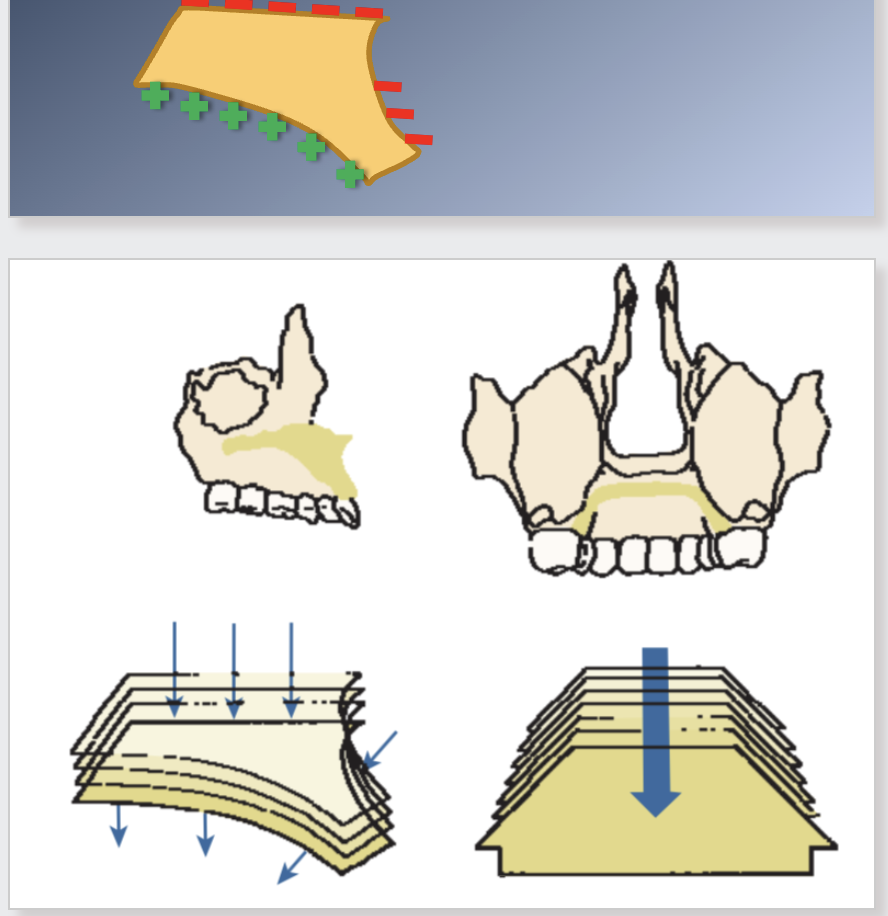
Sites of growth: Maxilla 3
5. As the maxilla grows downward and forward, its front surfaces are REMODELED.
1. Front surfaces are remodeled and bone is removed from most
of the anterior surface.
2. Anterior surface is moving forward.
5. Remodeling may oppose or produce an additive effect on growth.
1. Additive effect at the palatal bone: bone is removed on the nasal side and added on the oral side
2. Anterior part of the alveolar process is a resorptive area, cancelling part of the forward growth.
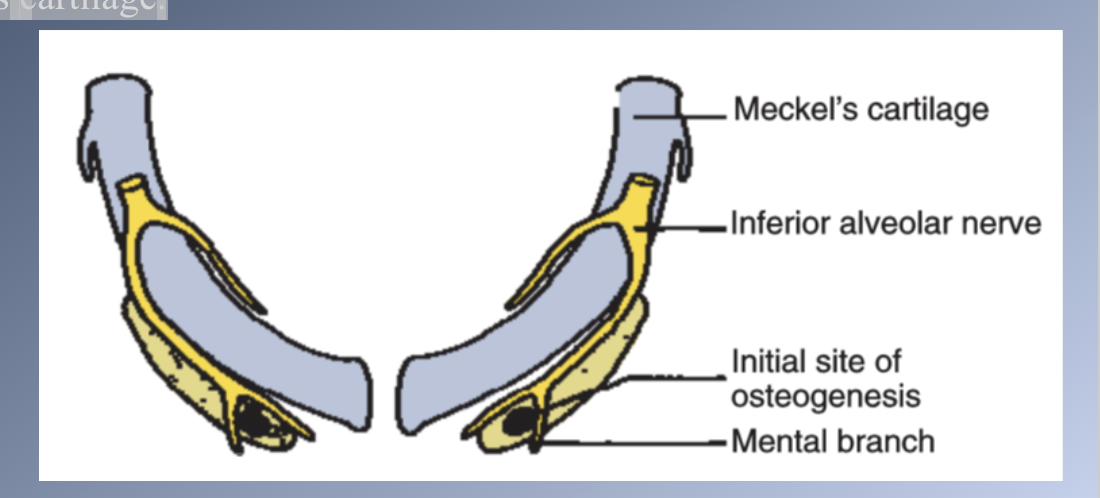
Manibular formation
1. EMBRYO:
• Mandible develops in the same area as the cartilage of the first pharyngeal arch, Meckel’s cartilage.
• Development begins as a condensation of mesenchyme lateral to Meckel’s cartilage.
EMBRYO:
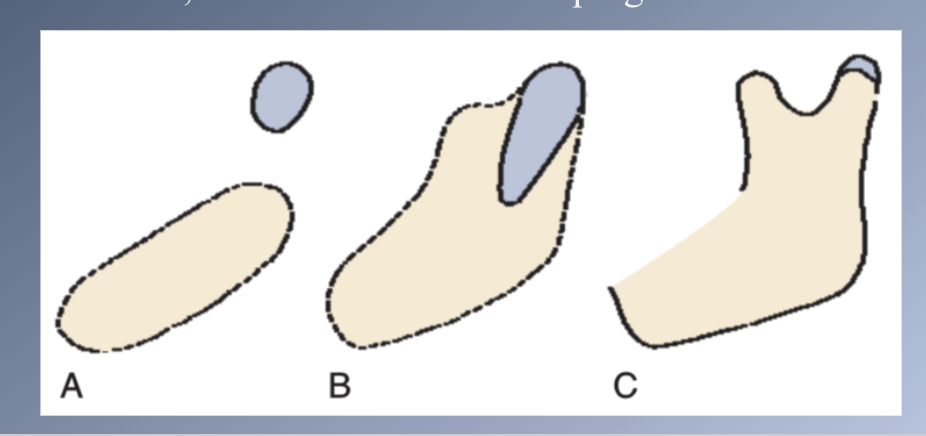
• Meckel’s cartilage disintegrates and largely disappears as the bony mandible develops
• Condylar cartilage develops initially as an independent secondary cartilage, separated by a considerable gap from the body (A)
• Early in fetal life, it fuses with the developing mandibular ramus (B)
Manibular formation 2
POST-NATAL GROWTH:
• Endochondral AND periosteal activity are important in growth of the mandible.
• Displacement of the TMJ by cranial base growth plays a negligible role.
3. CONDYLAR CARTILAGE OF THE TMJ:
• Cartilage covers the surface of the condyle at the TMJ.
• Hyperplasia, hypertrophy and ENDOCHONDRAL replacement.
OTHER AREAS OF THE MANDIBLE:
• Formed and grow by DIRECT SURFACE APPOSITION and REMODELING.
• How does the mandible grow???
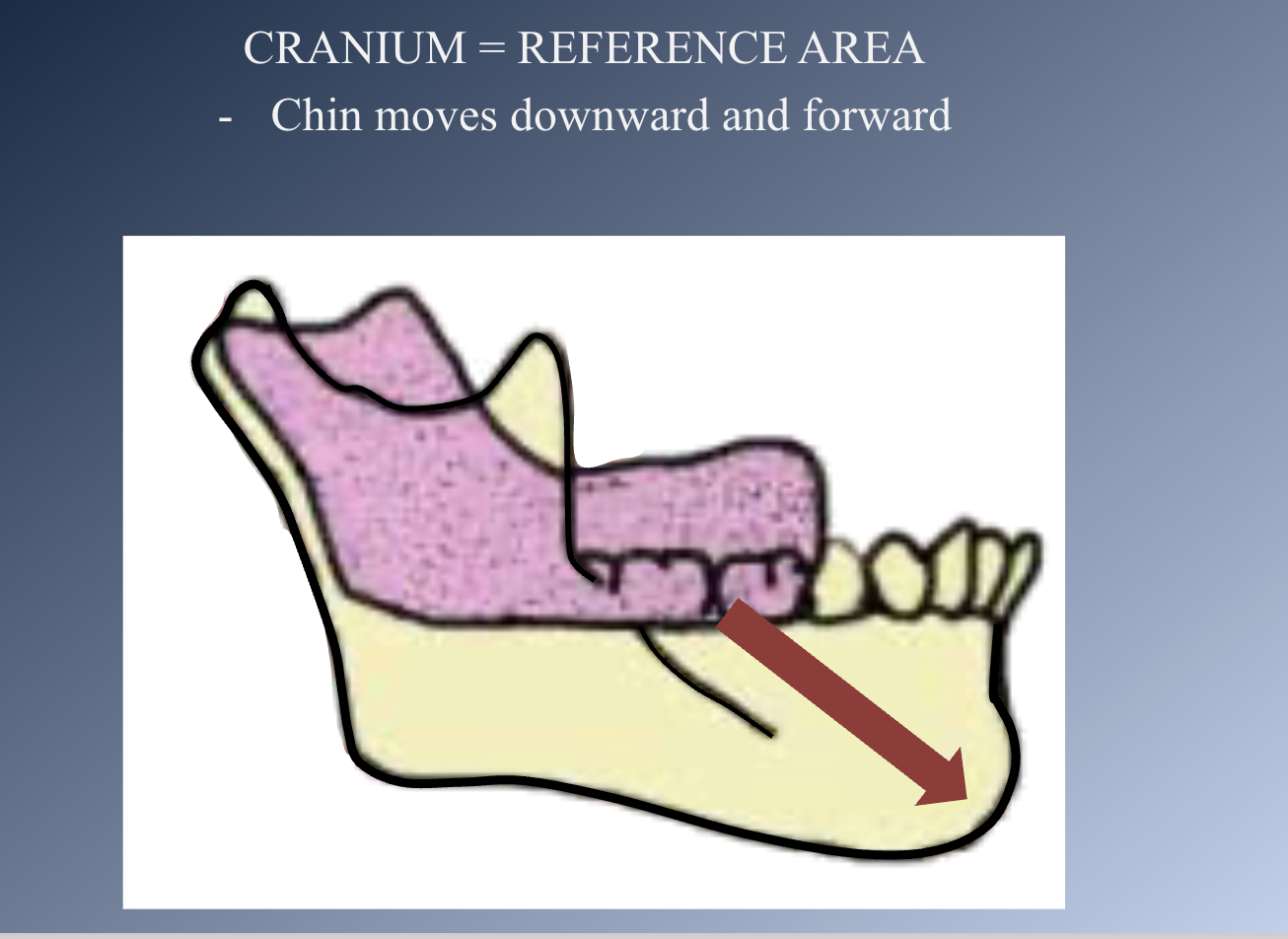
Direction of mandibular growth
Mandible formation: Growth sites
• CHIN: inactive, translated downward and forward
– Growth not possible by cartilage replacement or interstitial bone growth.
– Remodeling
• BODY of the mandible:
– Grows by PERIOSTEAL APPOSITION of bone on its
POSTERIOR surface.
• RAMUS:
– ENDOCHONDRAL replacement at the condyle
– SURFACE REMODELING
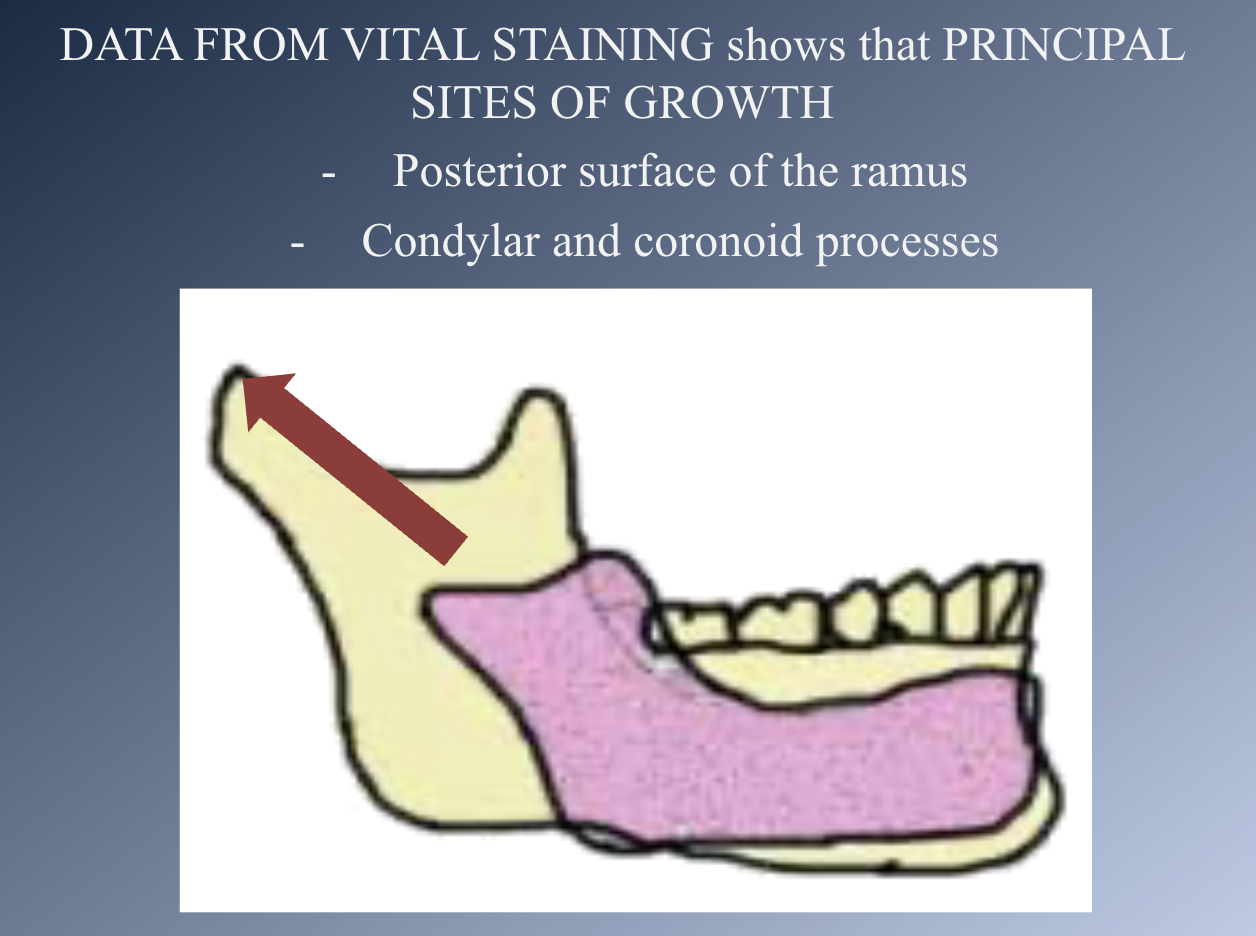
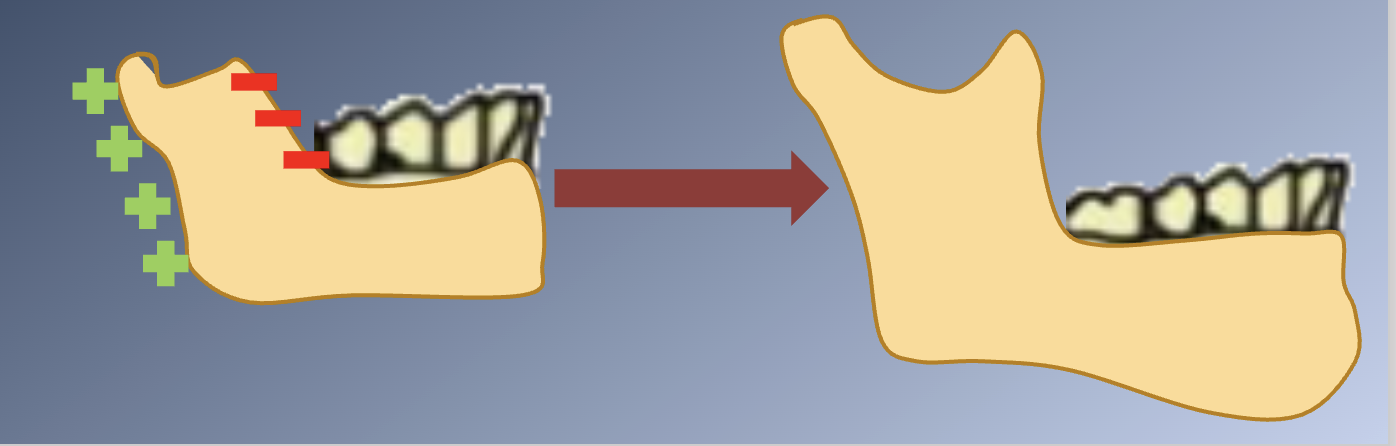
GROWTH SITES:
• The mandible grows longer by apposition of new bone on the posterior surface of the ramus.
• Large quantities of bone are removed from the anterior surface of the ramus.
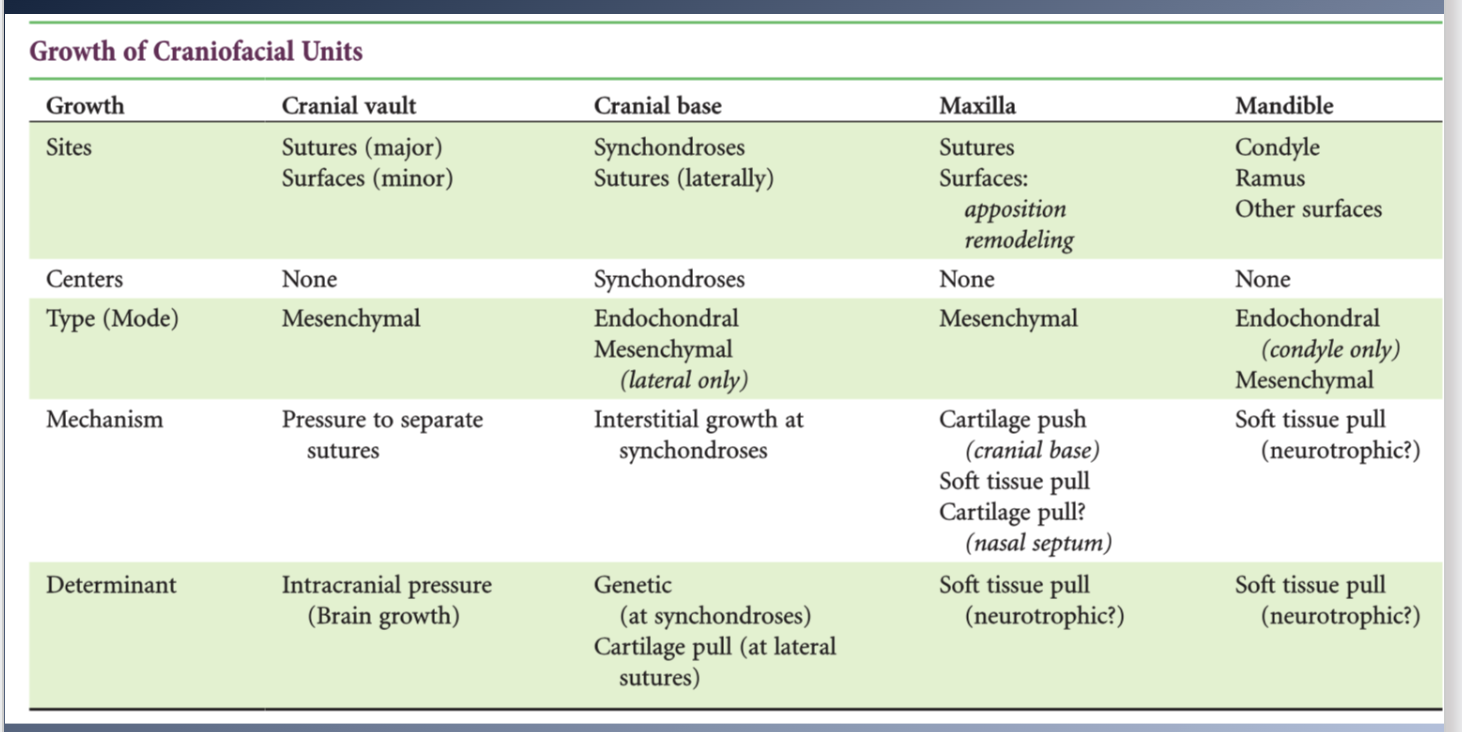
Summary
CRANIUM: grows as a response to growth of the brain
CRANIAL BASE:
- Independent growth potential, might be influenced by the growth of the brain.
- Endochondral growth and bony replacement at the synchondroses
- Synchondroses have independent growth potential, but might be influenced by the growth of the brain
Summary 2
Maxilla:
- Combination of growth at the sutures and direct remodeling on the surface.
- Translated downward and forward as the face grows
- Nasal septum cartilage and soft tissues contribute to the forward
repositioning of the maxilla
MANDIBLE:
- Endochondral proliferation at the condyle, apposition and resorption of bone at surfaces.
- Translated in space by the growth of the muscles and other soft tissues.
- Addition of new bone at the condyle is in response to the soft tissue changes.
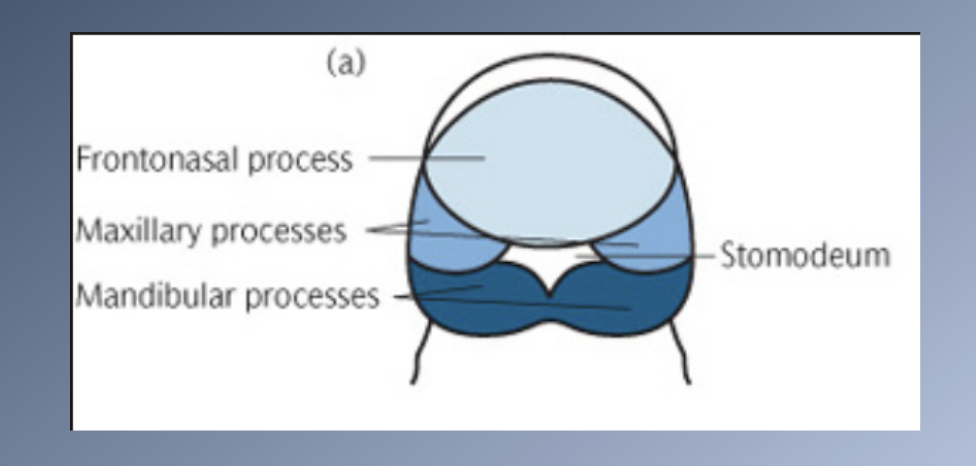
Embryological development
- Nearly all tissues of the face and neck originate from the
ECTODERM.
- Including the muscular and skeletal elements that elsewhere in the body are derived from the mesoderm.
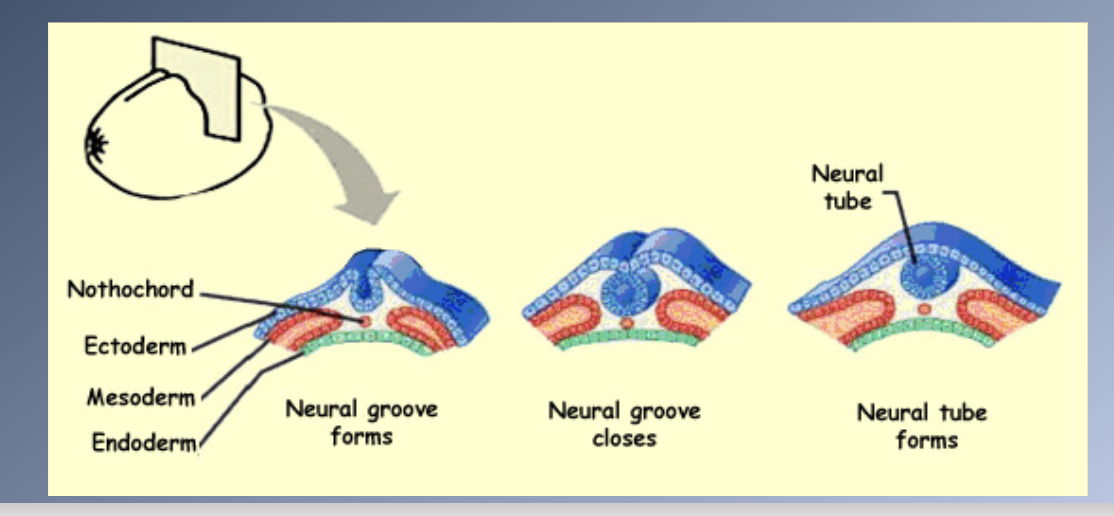
- Most of the tissues develop from the neural crest cells that migrate downward beside the neural tube and laterally under the surface ectoderm.
- Facial growth is dominated by regional growth centres as the organ systems are formed and final differentiation of tissues Xoccurs.
Embryological development 2
PRINCIPAL STAGES IN CRANIOFACIAL DEVELOPMENT
1. Germ layer formation and initial organization of craniofacial structures (Day 17)
2. Neural tube formation and initial formation of the oropharynx (Days 18-23)
Embryological development 3
PRINCIPAL STAGES IN CRANIOFACIAL DEVELOPMENT
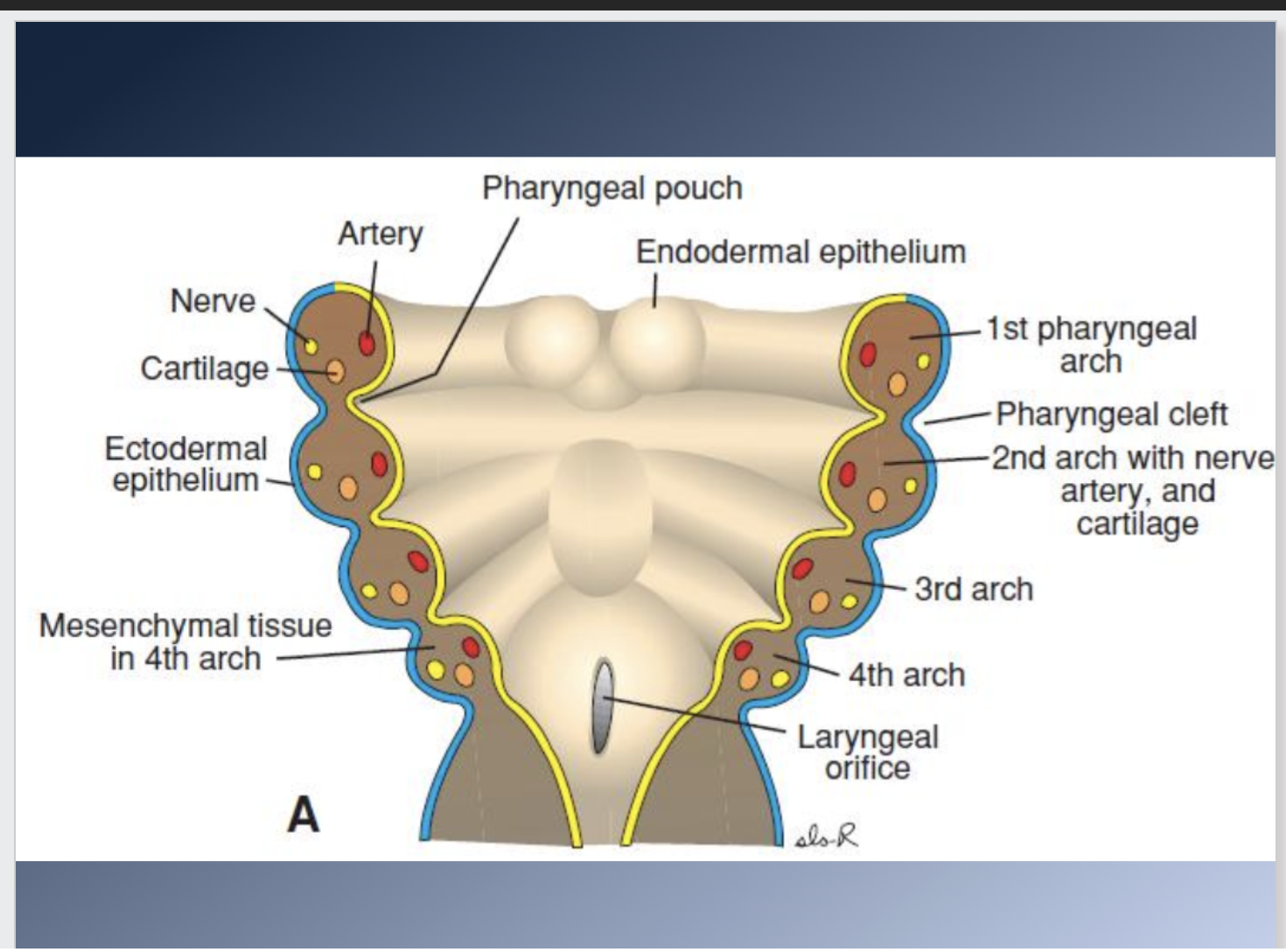
3. Origins, migrations and interactions of cell populations, especially neural crest cells (Days 19-28)

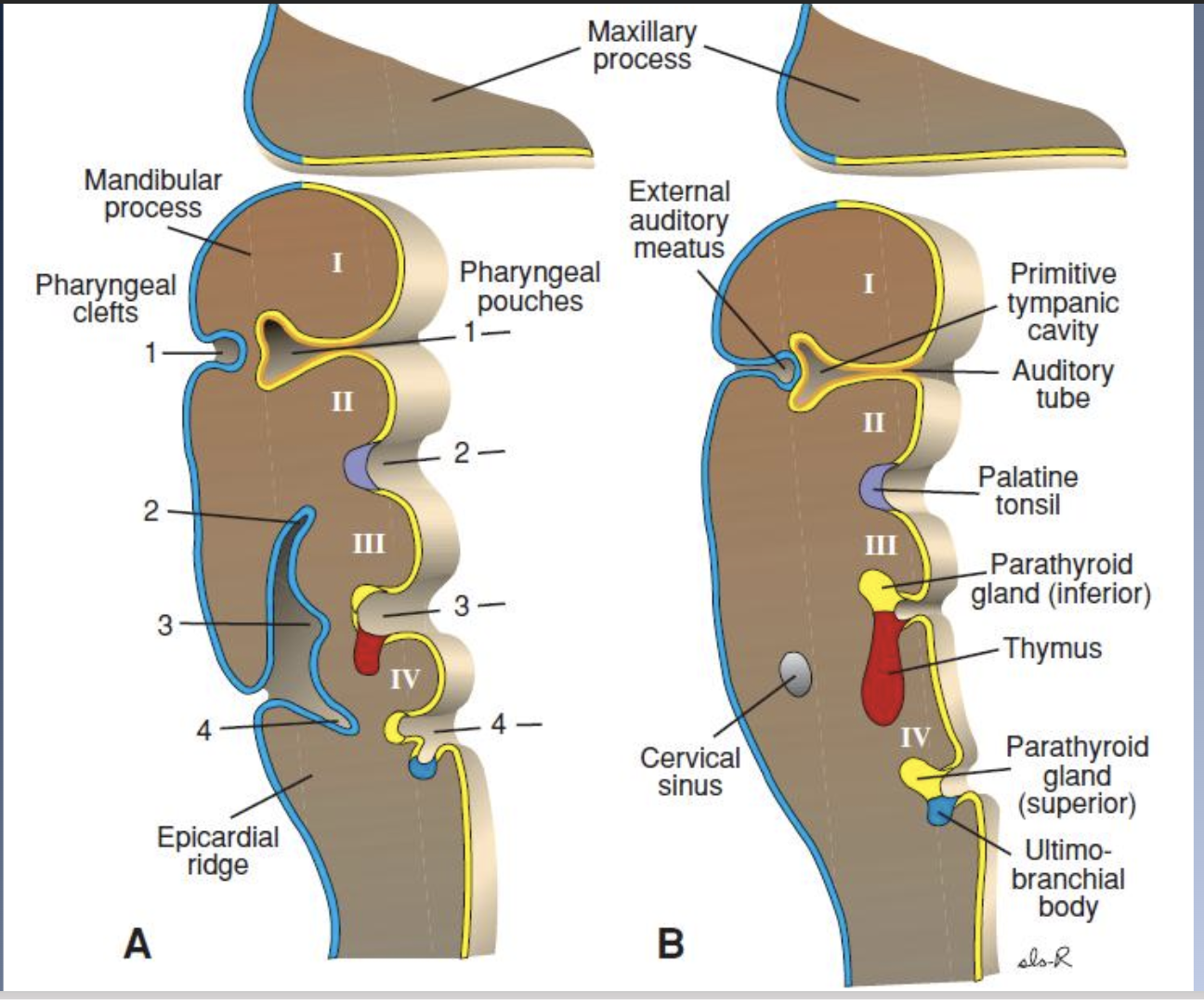
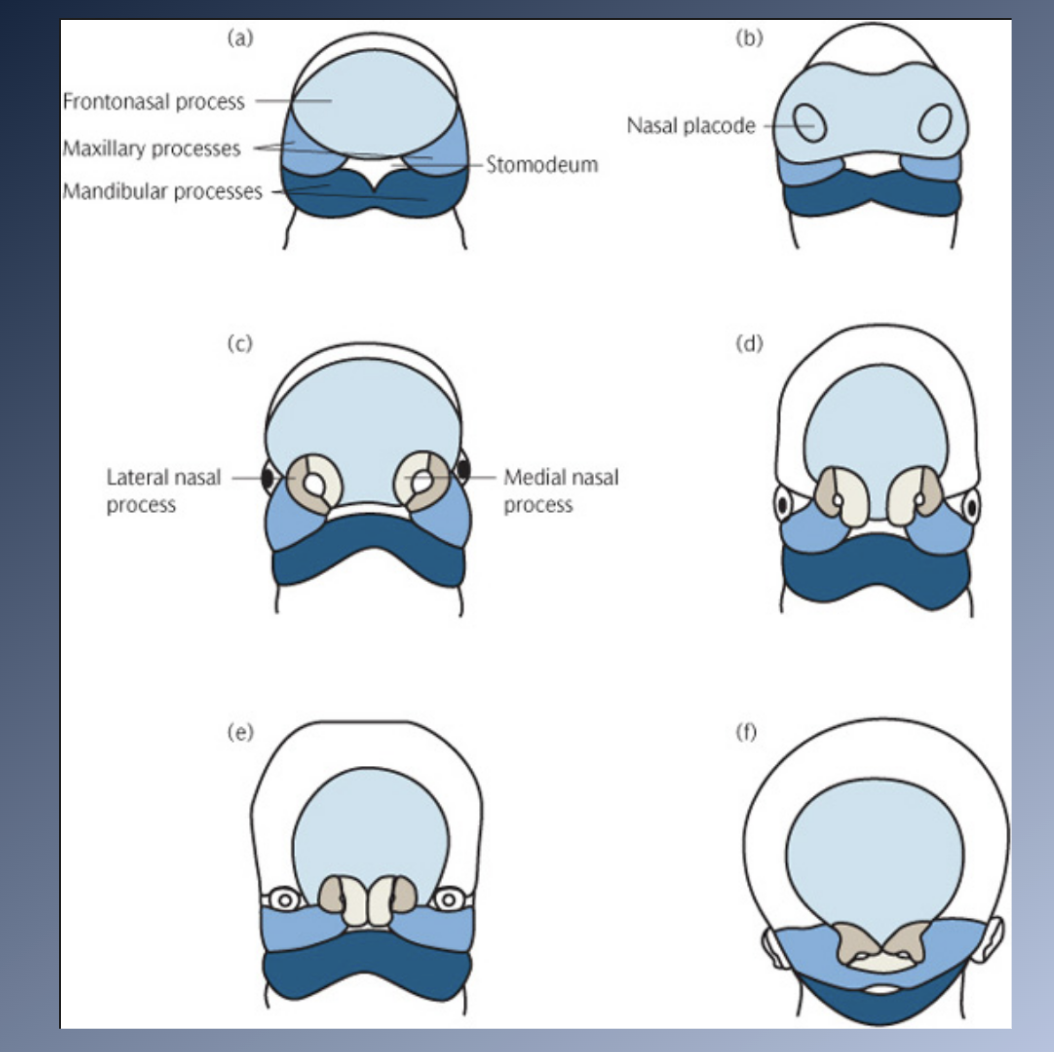
Embrologic development 4
PRINCIPAL STAGES IN CRANIOFACIAL DEVELOPMENT
4. Formation of organ systems, especially the pharyngeal arches and the primary (days 28-38) and secondary (Days 42-55) palates
5. Final differentiation of tissues: skeletal, muscular and nervous elements (Day 50-birth)
LATE FETAL DEVELOPMENT & BIRTH
- Third trimester of intrauterine life, fetus 1000g à3000g
- Continued rapid growth
- At birth, the head is nearly half the total body mass and is the largest impediment to passage through the birth canal
- Large uncalcified fontanelles allow change of shape during birth
- Relative lack of growth of the lower jaw
Pre-school years physical development
General pattern is a continuation of the pattern of the late fetal
period
1. Rapid growth
2. Relatively steady increase in height and weight
Circumstances that can affect normal growth
1. Premature birth
2. Chronic illness
3. Nutritional status
Circumstances that can affect normal growth
1. Premature birth
Low birth weight < 2500g
Premature infants: small first and second years of life
2. Chronic illness
Leave less energy available to support growth
Acute illness à temporary cessation of growth à no long-term effect
The more chronic the illness à more cumulative effect
3. Nutritional status
Nutritional supply in excess of the amount necessary for survival. Once nutritional adequacy is achieved, additional nutritional intake is not a stimulus to more rapid growth
Indicators of e=developmental age
1. Chronological age
2. Physical growth
3. Skeletal development
4. Dental development
Skeletal development
Assessment of skeletal age based on the MATURATIONAL STATUS of markers within the skeletal system:
1. Ossification of the bones of the hand and the wrist
2. Development of cervical vertebrae
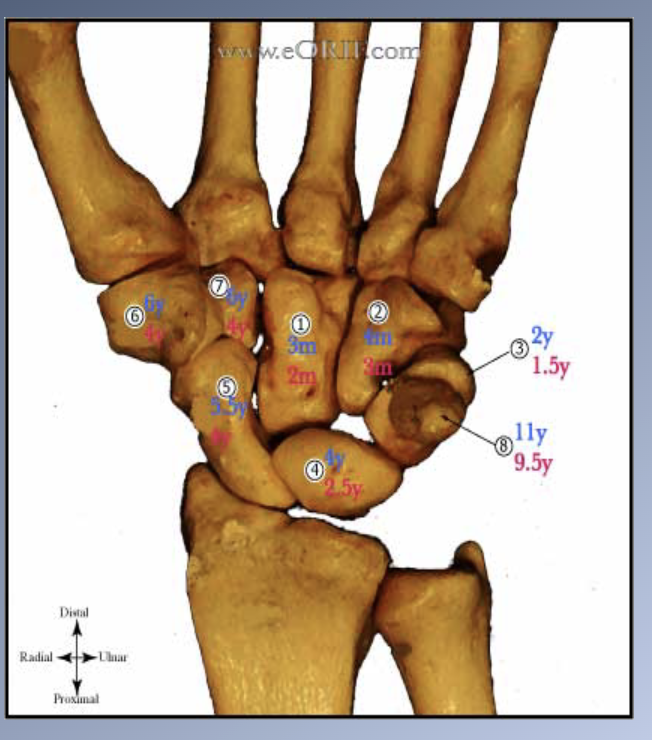
Skeletal development hand
Ossification of the bones of
the hand and the wrist
1. + 30 small bones which have predictable sequence of ossification.
2. All bones have a predictable sequence of ossification à accurate picture of the skeletal developmental status.
3. No single bone is diagnostic by itself.
4. Comparison with atlas of the development of the hand and wrist.
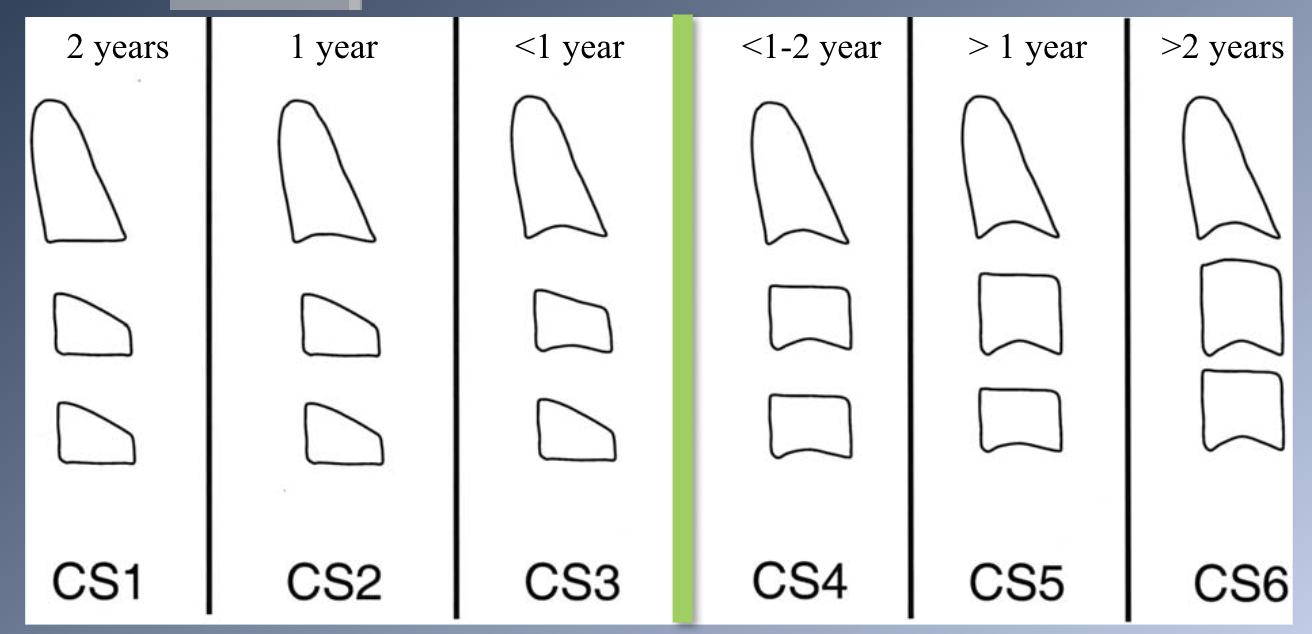
Development of cervical vertebrae
1. Evaluation of changes in the shape and size of cervical vertebrae.
Adolescence
Adolescence = period of life when sexual maturity is attained.
1. Secondary sexual characteristics appear.
2. Maturation of the sex organs.
3. Fertility is attained.
4. Adolescent growth spurt.
5. Adolescent growth spurt.
6. Profound physiologic changes that significantly affect the face and dentition.
- Mixed dentition à permanent dentition
- Acceleration in the overall rate of facial grow
- Differential growth of the jaws
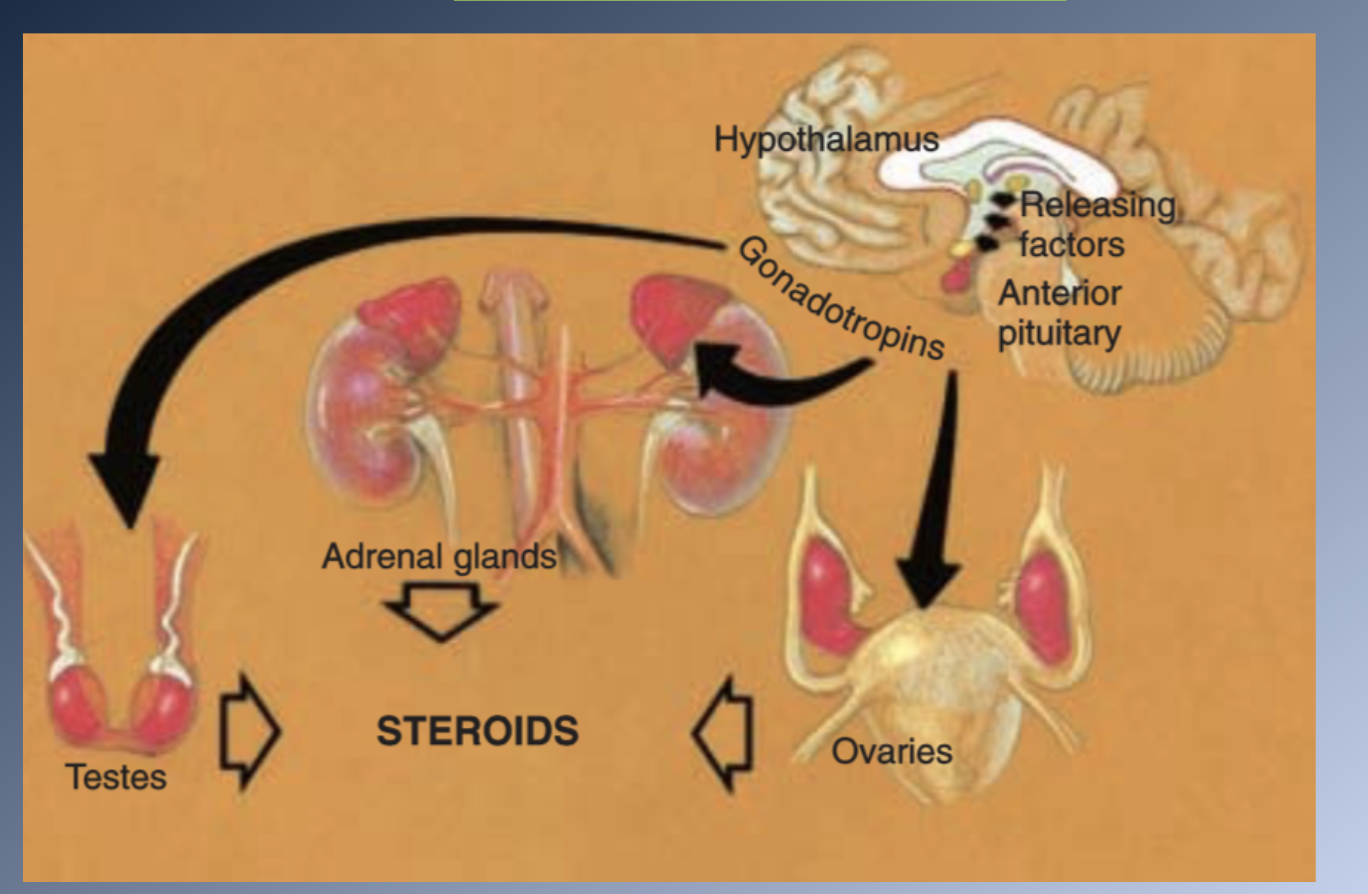
Initiation of adolescence
BRAIN influenced by internal clock and external stimuli→
HYPOTHALAMUS secretes RELEASING FACTORS→
Carried to the PITUITARY GLAND by the pituitary portal system→
ANTERIOR PITUITARY produces PITUITARY GONADOTROPINS→
Stimulate endocrine cells in the ADRENAL GLANDS and SEX ORGANS to produce SEX HORMONES
Adolescnce difference in sex
- In every individual, a mixture of male and female sex hormones is produced.
- Balance of the competing male and female hormones.
- MALE
- Different cell types in the testes produce both testosterone and the female sex hormones.
- FEMALE
- Secretion of estrogen by the ovaries, and later progesterone.
- Testosterone is produced in the adrenal cortex
TIMING OF PUBERTY
Individual variation- occurs usually 2 years before in girls vs. boys
TIMING OF PUBERTY- girls
Beginning of the physical growth spurt (PGS)
1) Appearance of breast buds
2) Early stages of the development of pubic hair
II. Peak velocity (1 year after stage 1)
1) Noticeable breast development
2) Pubic hair is darker and more widespread
3) Axillary hair
III. Onset of menstruation (1-1.5 year after stage 2)
1) Growth spurt is almost complete
2) Broadening of the hips
3) Adult fat distribution
4) Development of breasts is complete
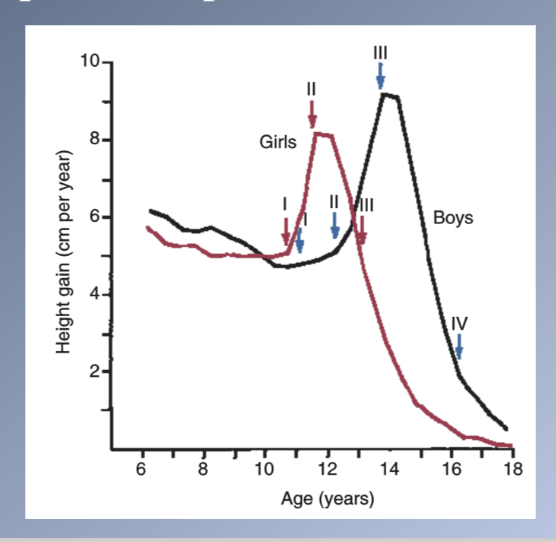
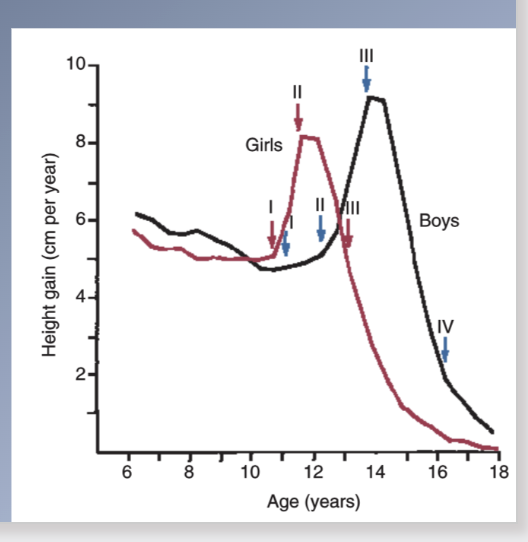
Boys puberty
I. Fat spurt
1) Gains weight, feminine fat distribution
2) Scrotum begins to increase in size
II. Spurt in height starts (1yr after stage I)
1) Redistribution and decrease in fat
2) Pubic hair starts to appear
3) Growth of the penis begins
III. Peak velocity (8-12m after stage II)
1) Axillary and facial hair upper lip
2) Spurt in muscle growth
3) Continued decrease subcutaneous fat
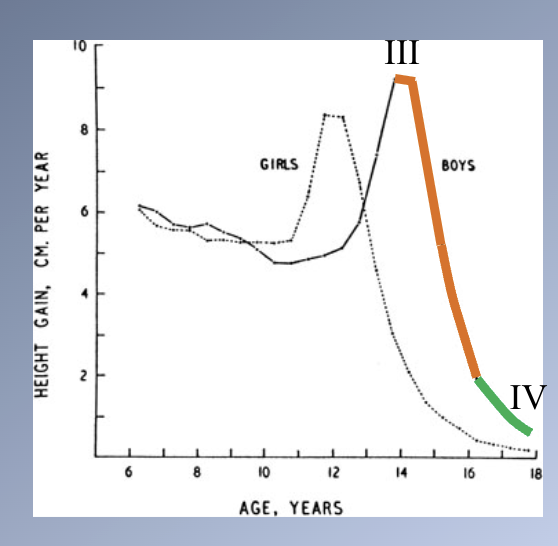
IV. Peak velocity (15-24m after stage III)
1) Spurt of growth ends
2) Facial hair on upper lip & chin
3) Color of pubic and axillary hair
4) Further increase in muscular strength
5) Adult distribution
Timing of puberty
- Importance in ultimate body size
- Earlier onset → smaller adult size
- Later onset → larger adult size
- Impact of sex hormones on ENDOCHONDRAL bone growth
- Stimulate cartilage to grow faster = PGS
- Increase rate of skeletal maturation
- Early cessation of growth after sexual maturity > girls
- Boys are taller than girls
- Girls mature earlier à finish growth much sooner
- Boys have slow but steady growth before PGS
- Epiphyseal plates close more slowly in males
Timing of puberty 2
Timing is affected by genetic and environmental influences.
- Amount of body fat in girls
- Seasonal and cultural factors (faster in spring & summer)
- City children mature faster than rural ones
Growth of the jaws correlates with the physiologic events of puberty in a similar way as growth in height
1) Adolescent growth spurt in the length of the mandible
2) Modest increase in growth at the sutures of the maxilla
3) Cephalocaudal gradient of growth more evident→ Mn growth > Mx growth = DIFFERENTIAL JAW GROWTH
4) Juvenile spurt (girls> boys) 1-2yr before adolescent PGS → equal or even greater the jaw growth in sexual maturation