Week 9 - Brainstem II and Visual Fields
1/65
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
_________: double vision
Diplopia
What are potential causes of diplopia? (hint: 5x)
1. Disorders of the extraocular eye muscles
2. Nerve injury/compression
3. Trauma
4. Disorders of NMJ
5. Inflammation
How does disorders of the extraocular eye muscles cause diplopia?
Dysconjugate gaze (gaze doesn't line up b/w the eyes)
Which pathologies can cause diplopia?
- Thyroid disease (affects the muscles)
- Myasthenia gravis (affects the NMJ)
- MS (affects the CN II via inflammation)

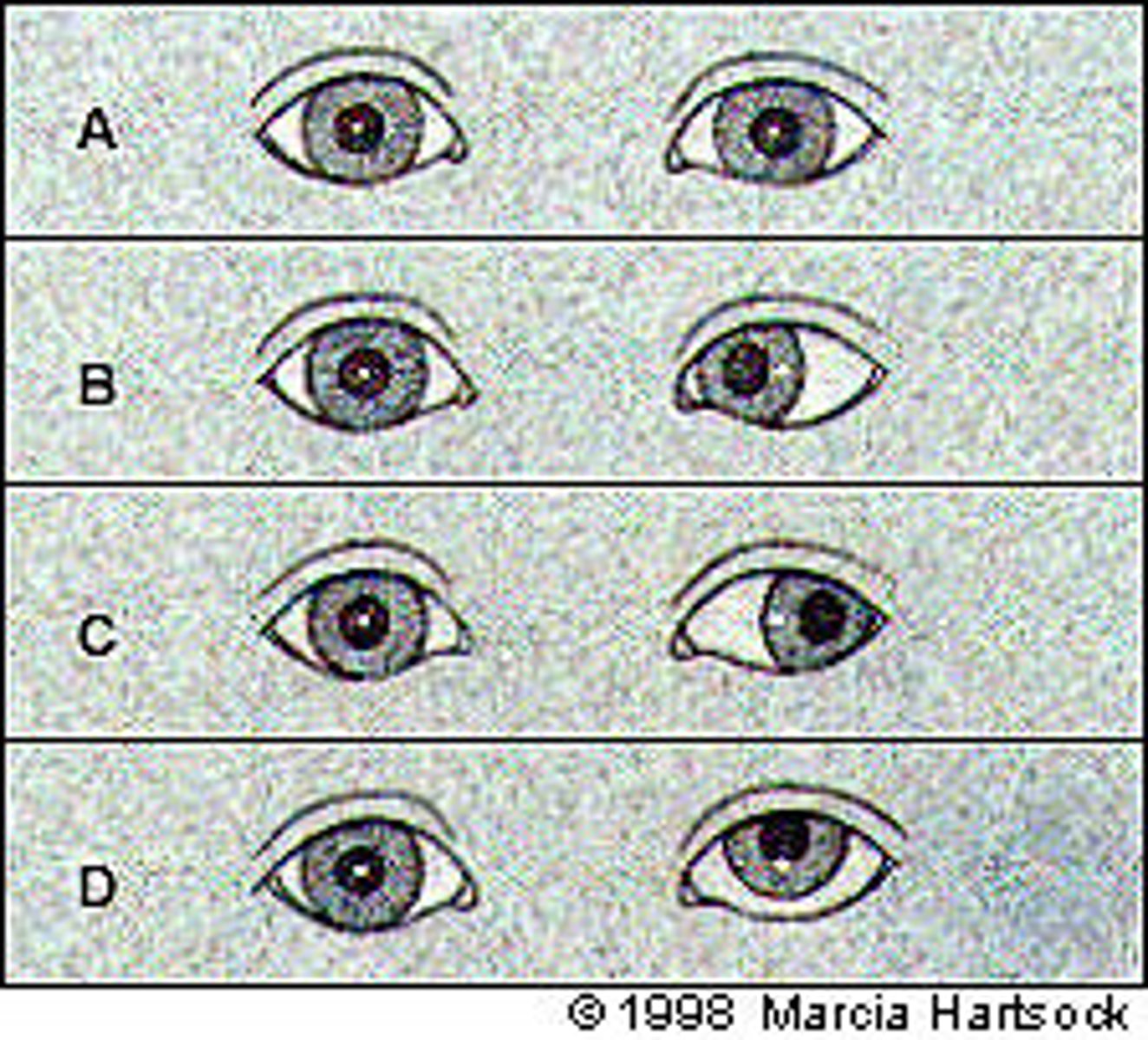
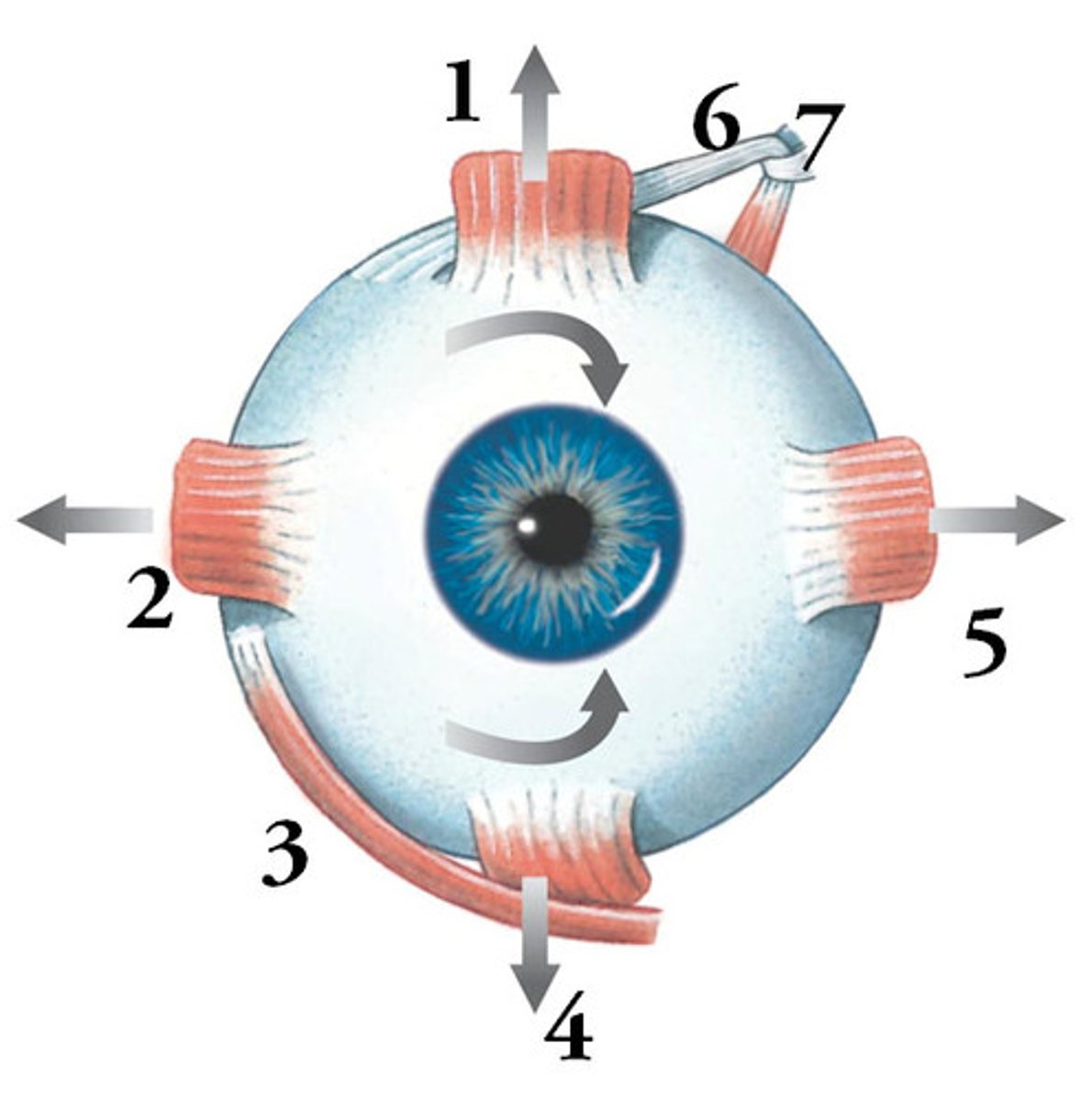
Oculomotor palsy: muscle(s) affected
MR, IR, SR, IO, levator palpebrae
Oculomotor palsy: resting eye position
Down and out (only LR + SO are active)
Oculomotor palsy: eyelid position
Ptosis (drooping)
Oculomotor palsy: pupil signs
Dilated, unresponsive to light
Trochlear palsy: muscle(s) affected
Superior oblique (depression & intorsion)
Trochlear palsy: resting eye position
Up (hypertropia) and out (extorsion--not visible)
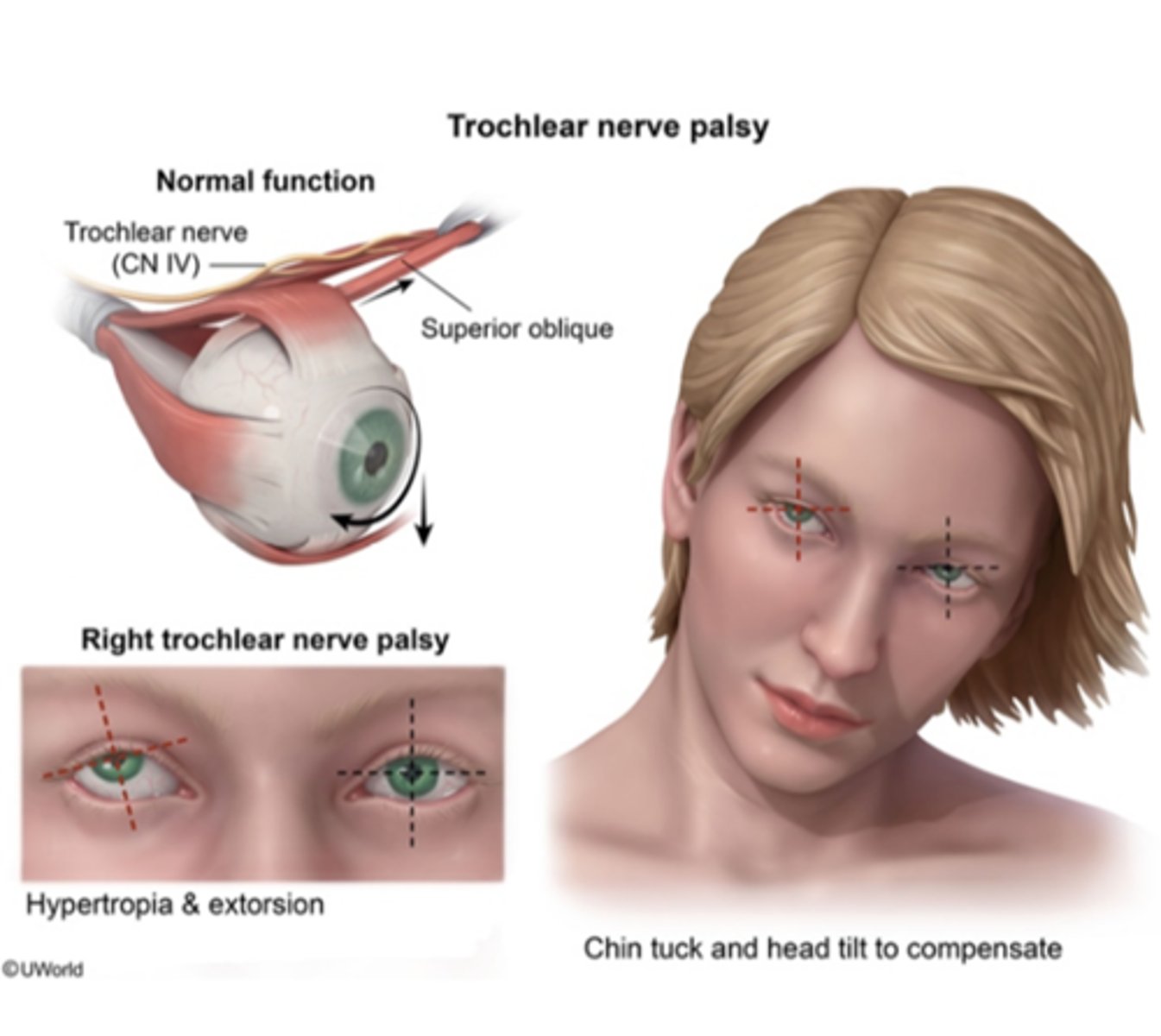
Trochlear palsy: compensation/ head position
Head tilt AWAY from the affected side w/ chin tuck
Trochlear palsy: diplopia direction
Vertical
Abducens palsy: muscle(s) affected
Lateral rectus
Abducens palsy: resting eye position
Adduction
Abducens palsy: diplopia direction
Horizontal
Pupil constriction is under _______ (SNS/ PNS) control
PNS
Pupil dilation is under ________ (SNS/ PNS) control
SNS
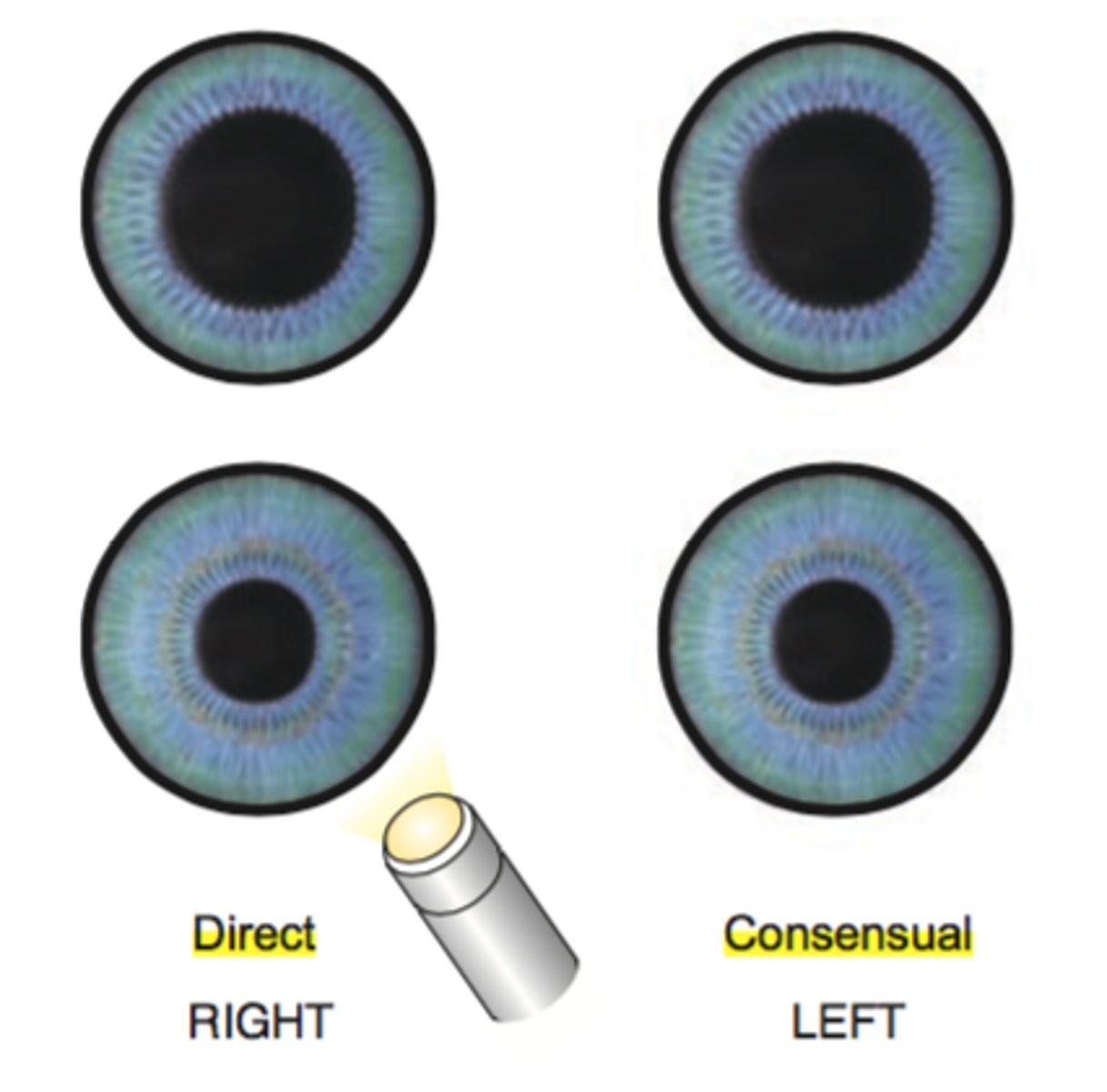
Direct response (NORMAL): light shown in RIGHT eye --> ________ (left/ right) pupil constriction
Right
Consensual response (NORMAL): light shown in RIGHT eye --> ________ (left/ right) pupil constriction
Left
Direct response (ABnormal): light shown in RIGHT eye --> right _________ (constriction/dilation)
No response--may appear dilated
Consensual response (ABnormal): light shown in RIGHT eye --> left ________ (constriction/dilation)
Constriction
Horner syndrome: due to disruption to _______ (SNS/ PNS) pathway to eye and face
SNS
Horner syndrome: potential causes/ lesions
- Lateral hypothalamus or brainstem lesion
- Spinal cord lesion (above T1-T2)
- T1/T2 spinal root damage
- Carotid plexus damage
- Cavernous sinus damage
- Orbit lesion
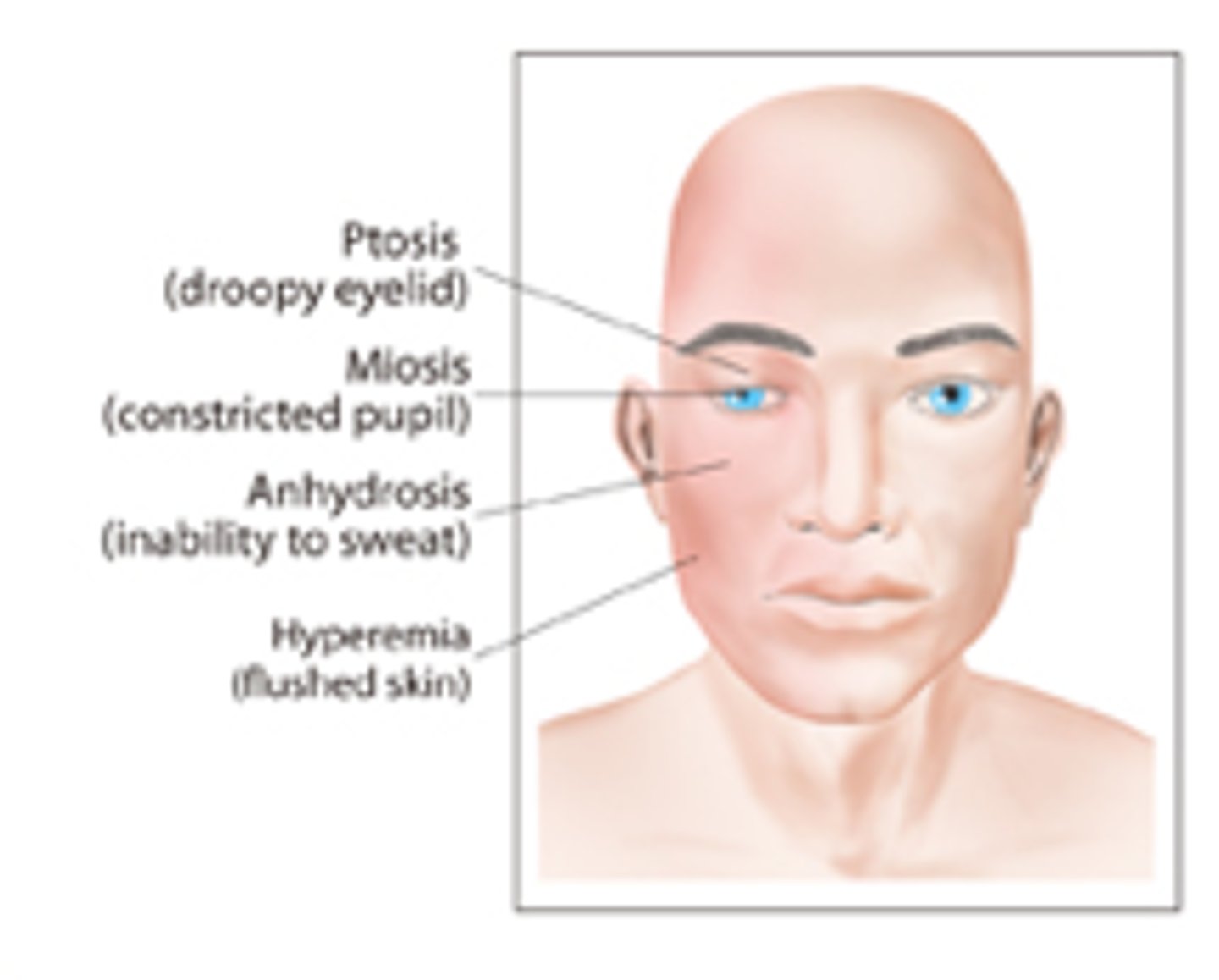
Horner syndrome: clinical signs
1. Ptosis (upper eyelid droop)
2. Miosis (constricted pupil)
3. Anihidrosis (decreaed sweating)
True or false: circuits from the cerebellum and brainstem to the cortex influence cranial nerves III, IV, and VI
TRUE (this is known as supranuclear control and it prevents us from being chameleons)

________: rapid eye movements to bring an object of interest into visual field
Saccades
________: stable movement of eyes to keep a focus on a moving target
Smooth pursuit
__________: visual fixation on an object that is moving closer or farther away
Vergence
_________: ability to maintain visual fixation while the head is moving
Vestibulo-ocular reflex (VOR)
Which regions of the cortex are involved w/ regulating eye movements?
1. Visual cortex
2. Parieto-occipito-temporal area
3. Frontal eye fields
__________: interprets visual input received from CN II
Visual cortex (Bordmann area 17)
_________: produces ipsilateral pursuit and contralateral eye movements
Parieto-occipito-temporal area
_________: produces contralateral saccades
Frontal eye fields (Brodmann area 8)
W/ right-way eyes, the eyes gaze ________ (toward/away) from the side of weakness/paralysis
AWAY
(ex: L cortical lesion or stroke --> R hemiparesis --> L gaze TOWARD side of lesion)
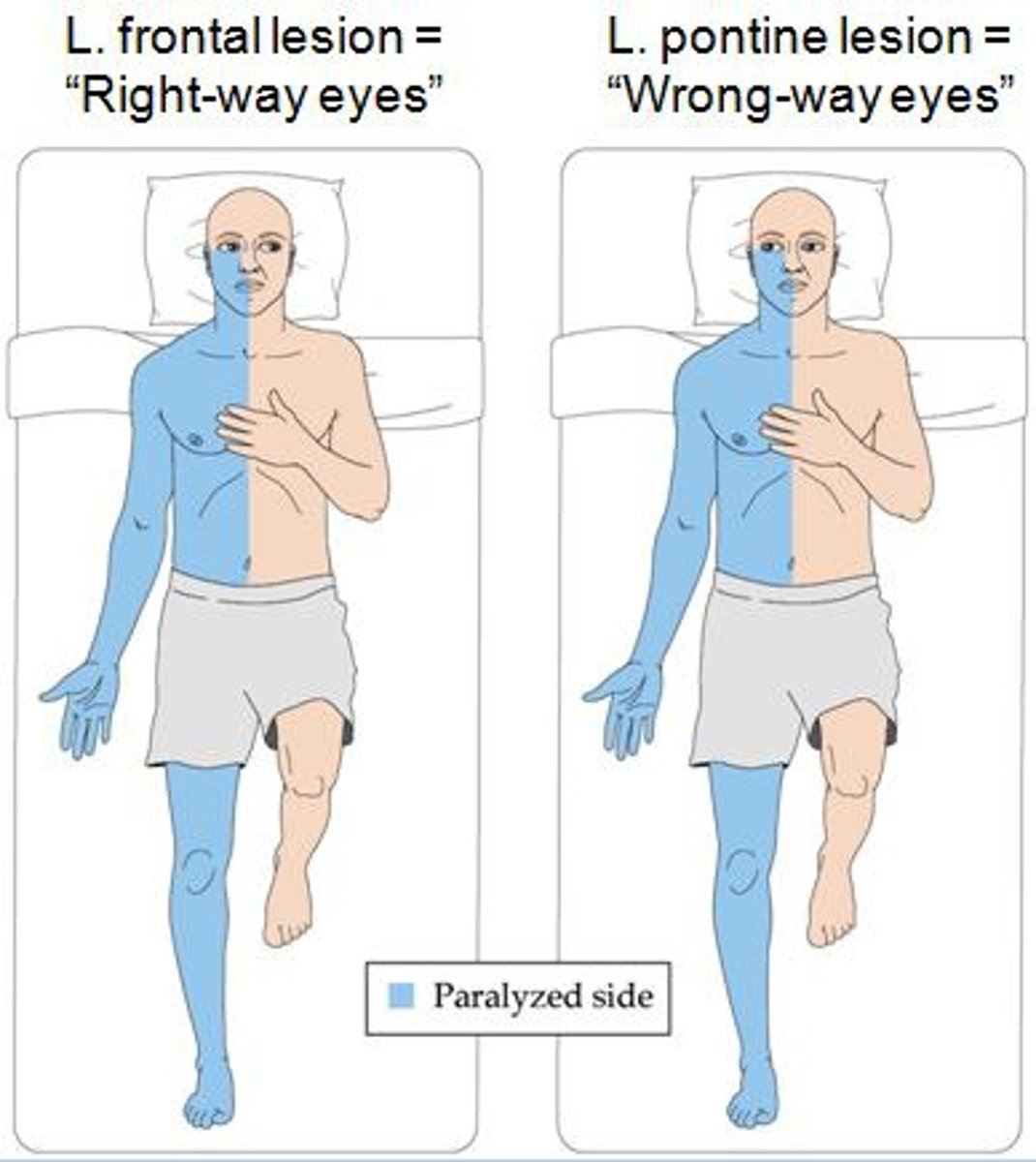
W/ wrong-way eyes, the eyes gaze __________ (toward/away) from the side of weakness/paralysis
TOWARD
(ex: involvement of abducens nucleus or PPRF --> ipsilateral gaze weakness --> eyes drift AWAY from the side of lesion)
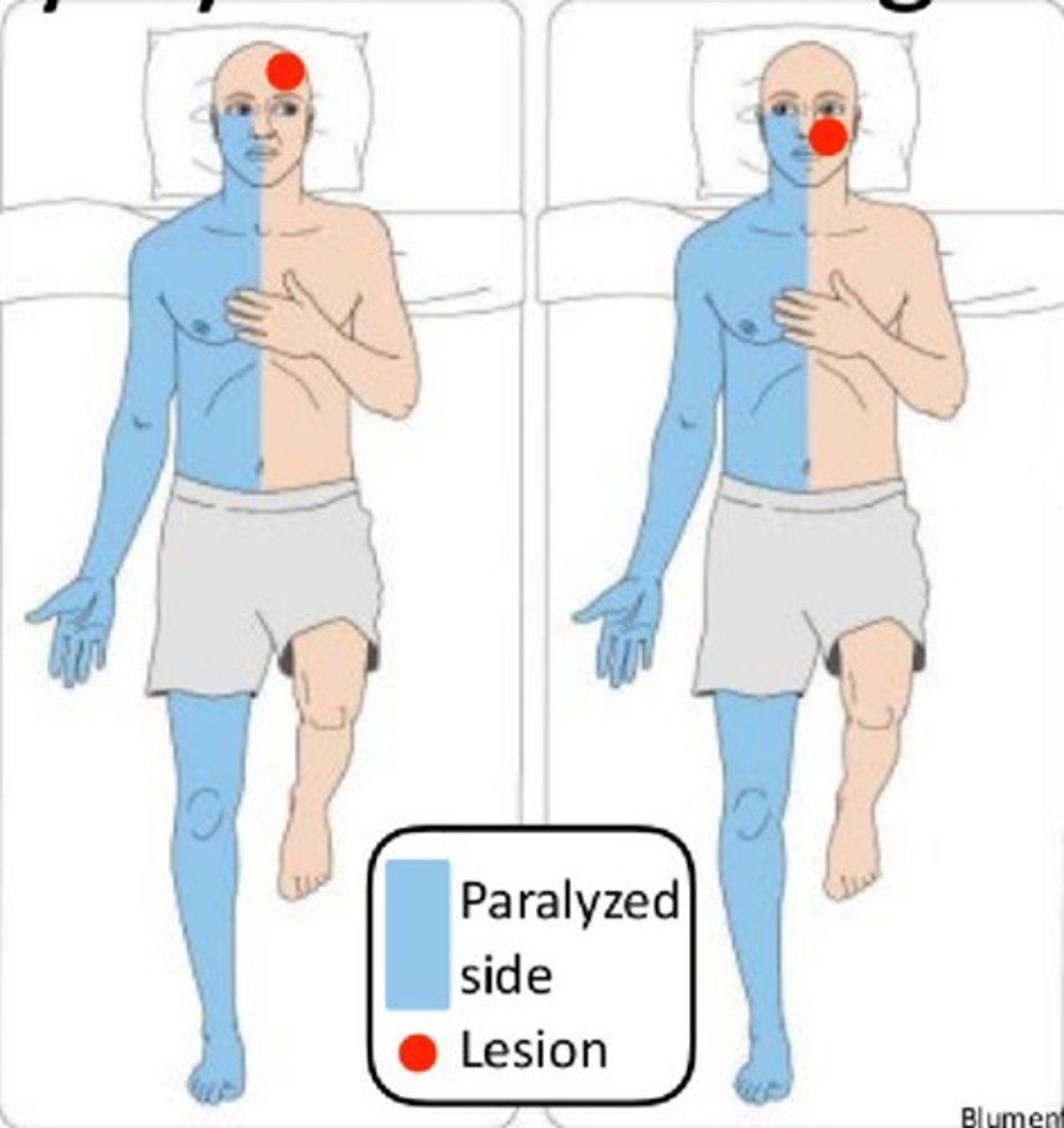
Where is the location of damage w/ right-way eyes?
Cerebral hemispheres
Where is the location of damage w/ wrong-way eyes?
Cortex seizure activity, thalamic hemorrhage, lesions of pons -- more serious
How is an image perceived by the retina?
Inverted and reversed
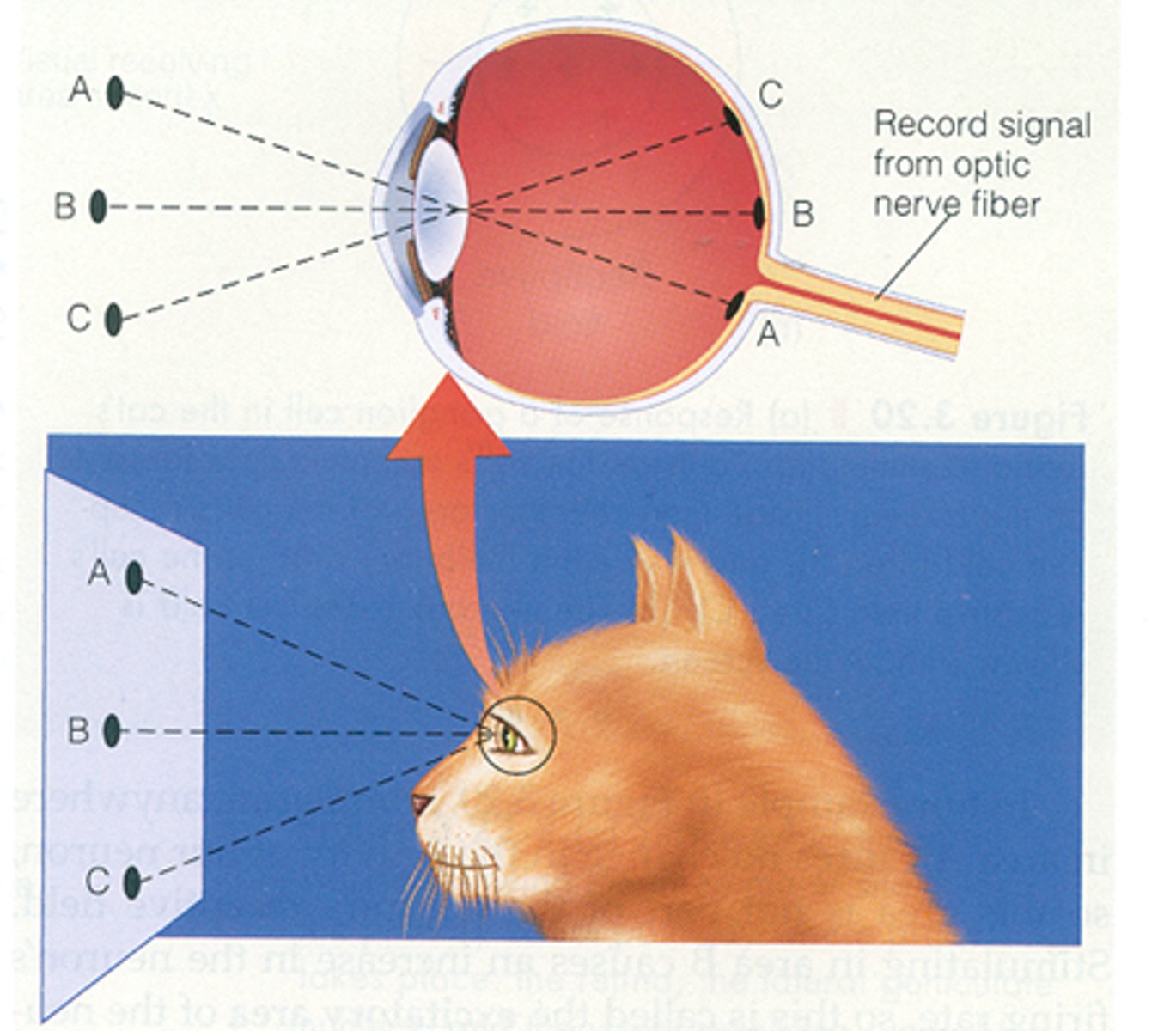
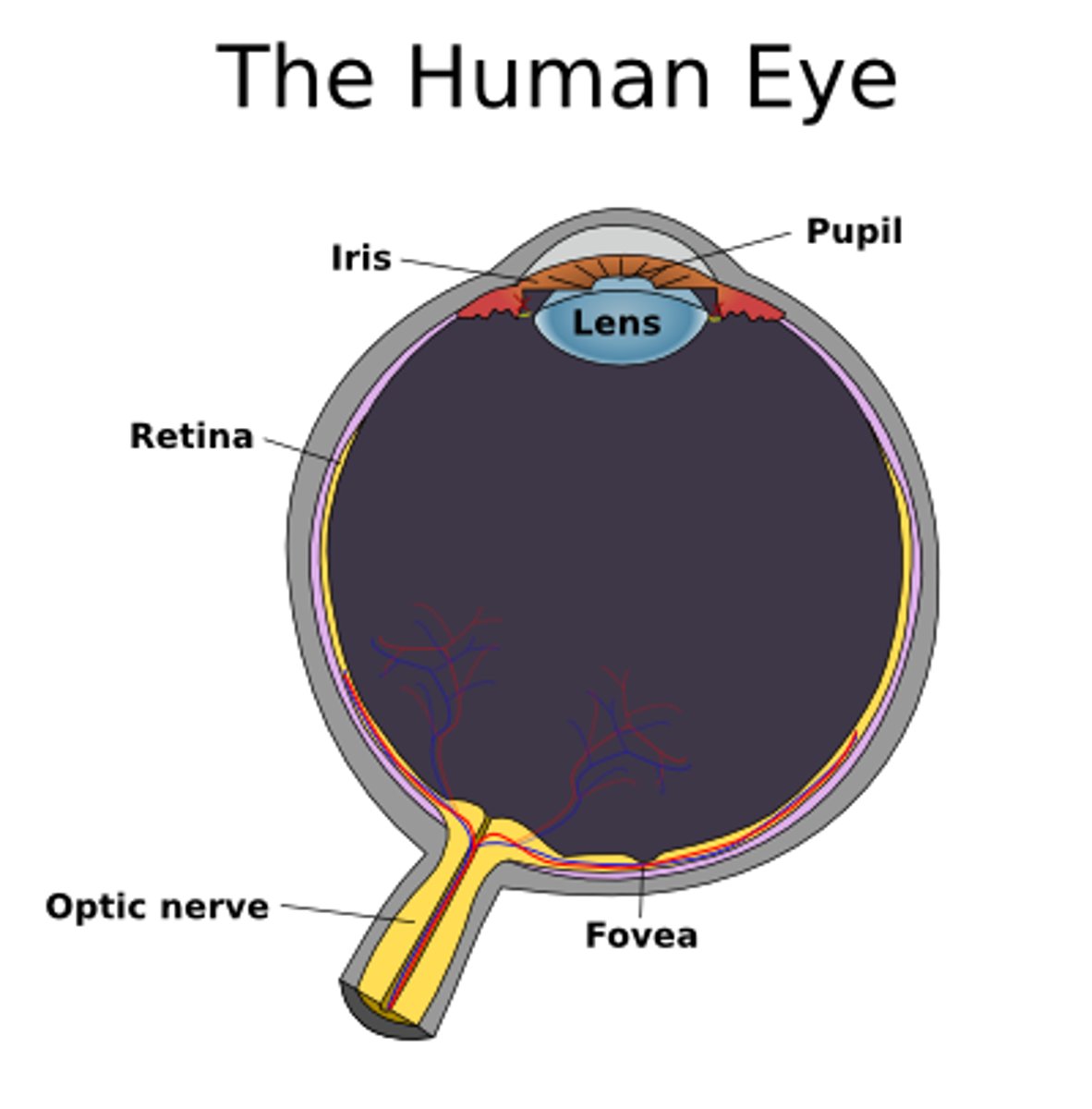
What is the name for the portion of the retina that has the greatest visual acuity?
Fovea
Which cells in the retina make up the optic nerves and "fire" action potentials?
Ganglion cells
If you are looking at an object that is on the RIGHT, where does it project in the eye?
R temporal visual field --> R nasal retinal field
L nasal visual field --> L temporal retinal field
Info from the nasal retinal fields travel down the optic nerve to reach which structure?
Optic chiasm
Which RETINAL field crosses: nasal or temporal
Nasal (info from the temporal RETINAL field carries onto optic tract on ipsilateral side)
Info from the nasal and temporal retinal fields eventually travel through the track together to synapse (primarily) in which structure?
LGN (of thalamus)
From the LGN, info from the R SUPERIOR VISUAL field will travel through which optic radiation?
L inferior optic
What is another name for the inferior optic radiations?
Meyer's loop
What is the pathway of the inferior optic radiations?
LGN --> around temporal lobe --> lower bank of the calcarine fissure (lingula)
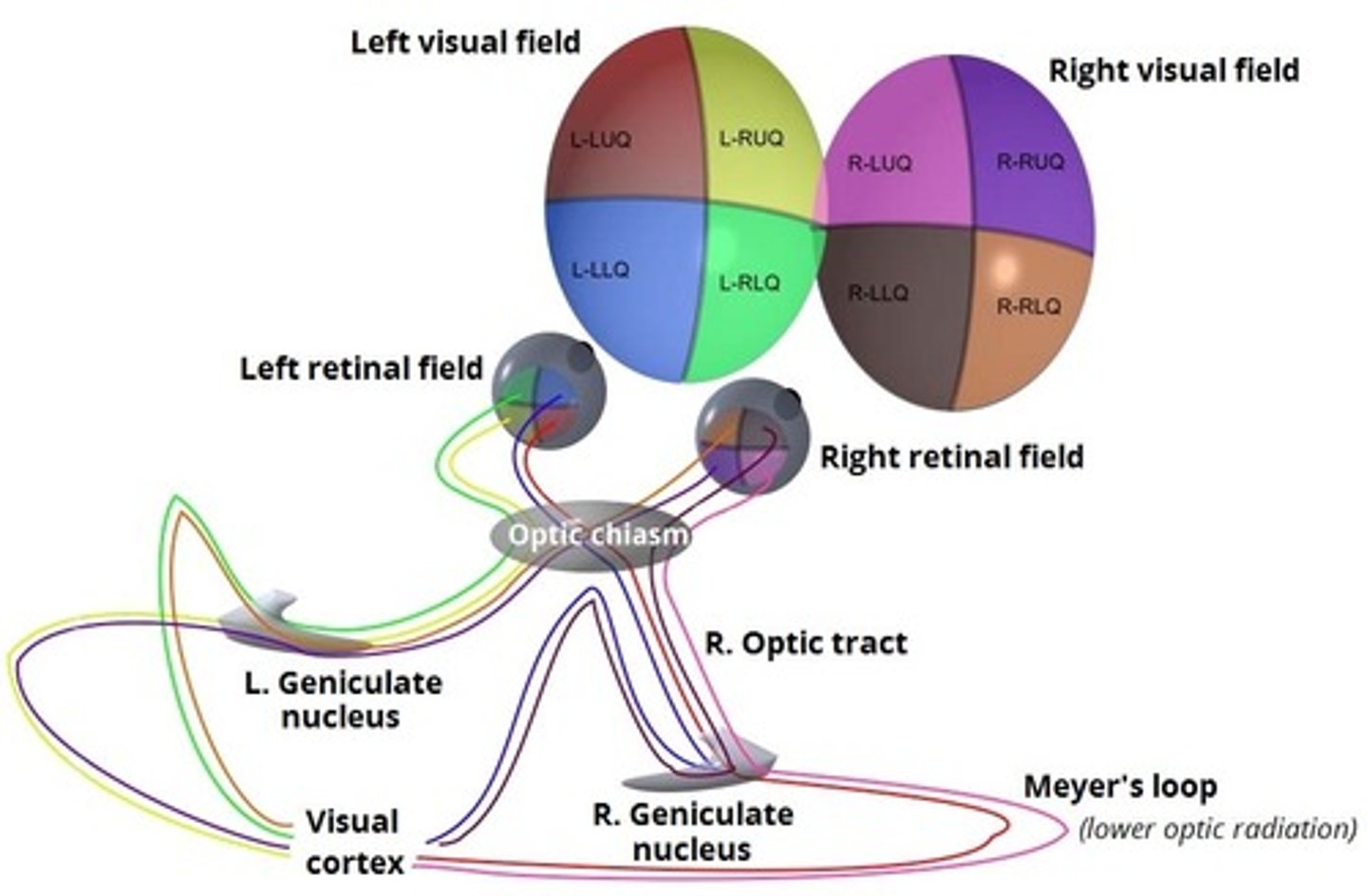
From the LGN, info from the L INFERIOR VISUAL field will travel through which optic radiation?
R superior optic
What is the pathway of the superior optic radiations?
LGN --> parietal lobe --> upper bank of calcarine fissure (cuneus)
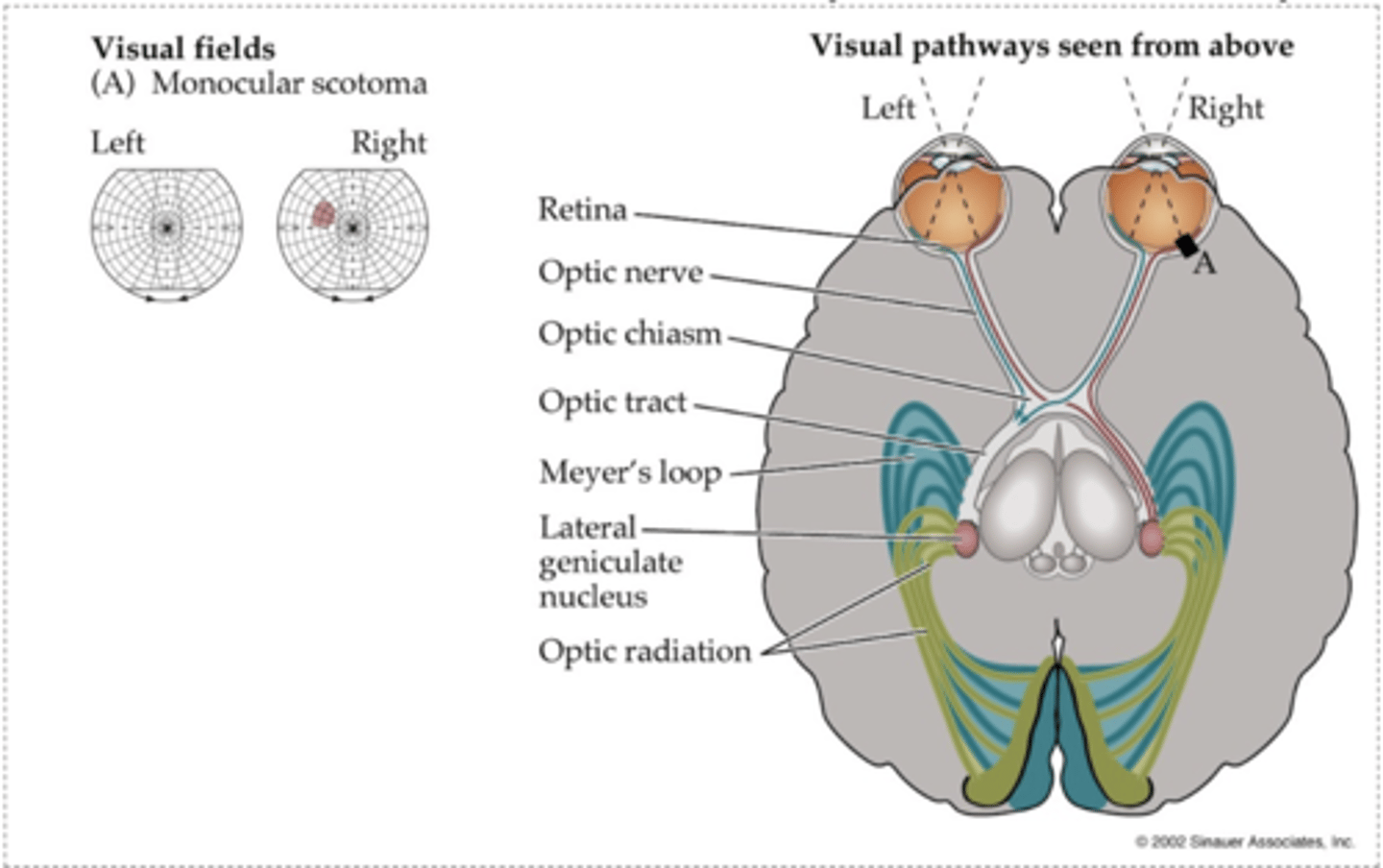
Visual field deficit: retina of R eye
R monocular scotoma (circumscribed region of vision loss)
What are some possible causes of a lesion @ the retina?
Retinal infarcts, infections, degeneration
Visual field deficit: optic nerve of R eye
R monocular vision loss
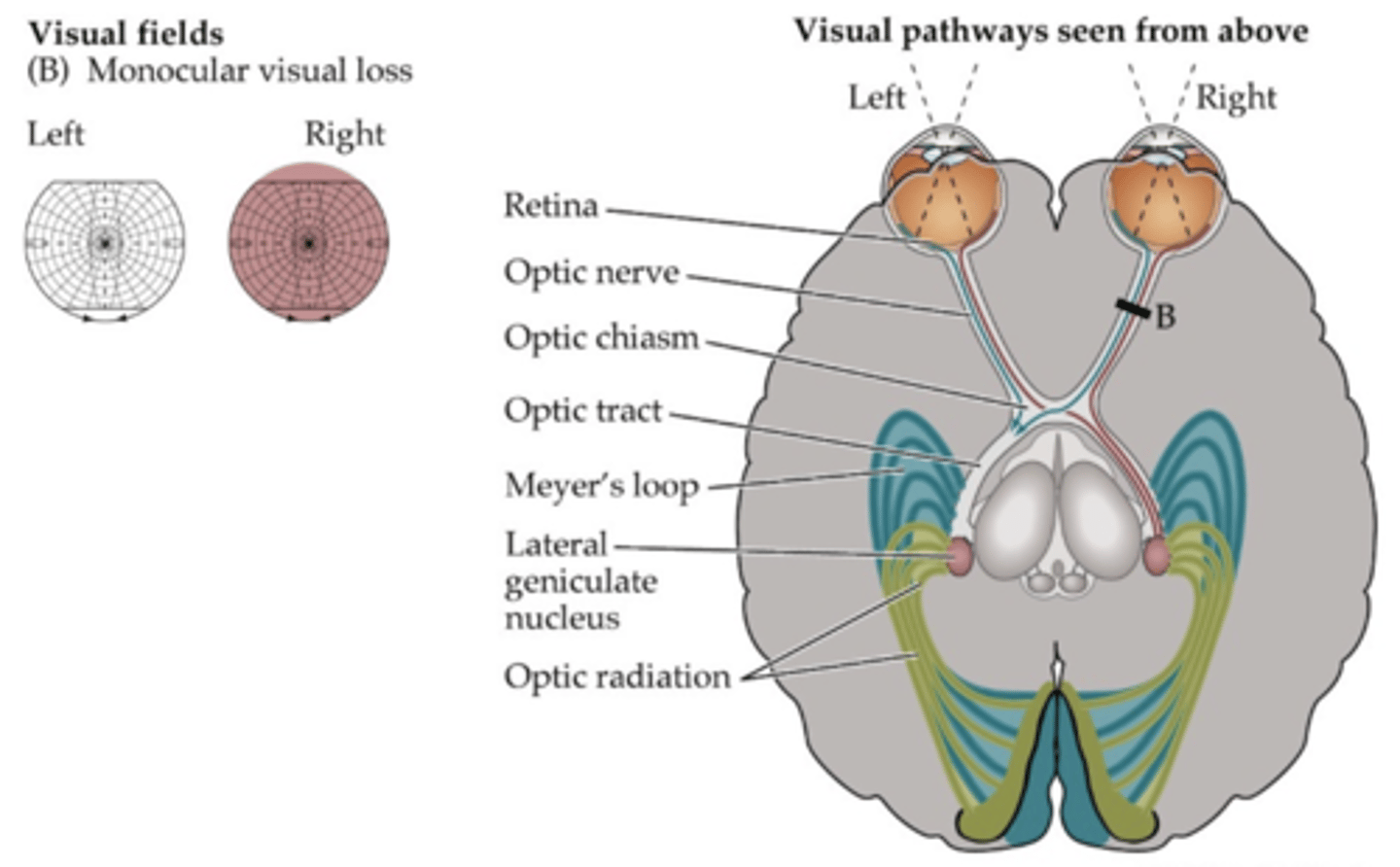
_________: blindness in one eye
Anopia
What are some possible causes of a lesion @ optic nerve?
Optic neuritis/ MS, glaucoma, tumors of CN II
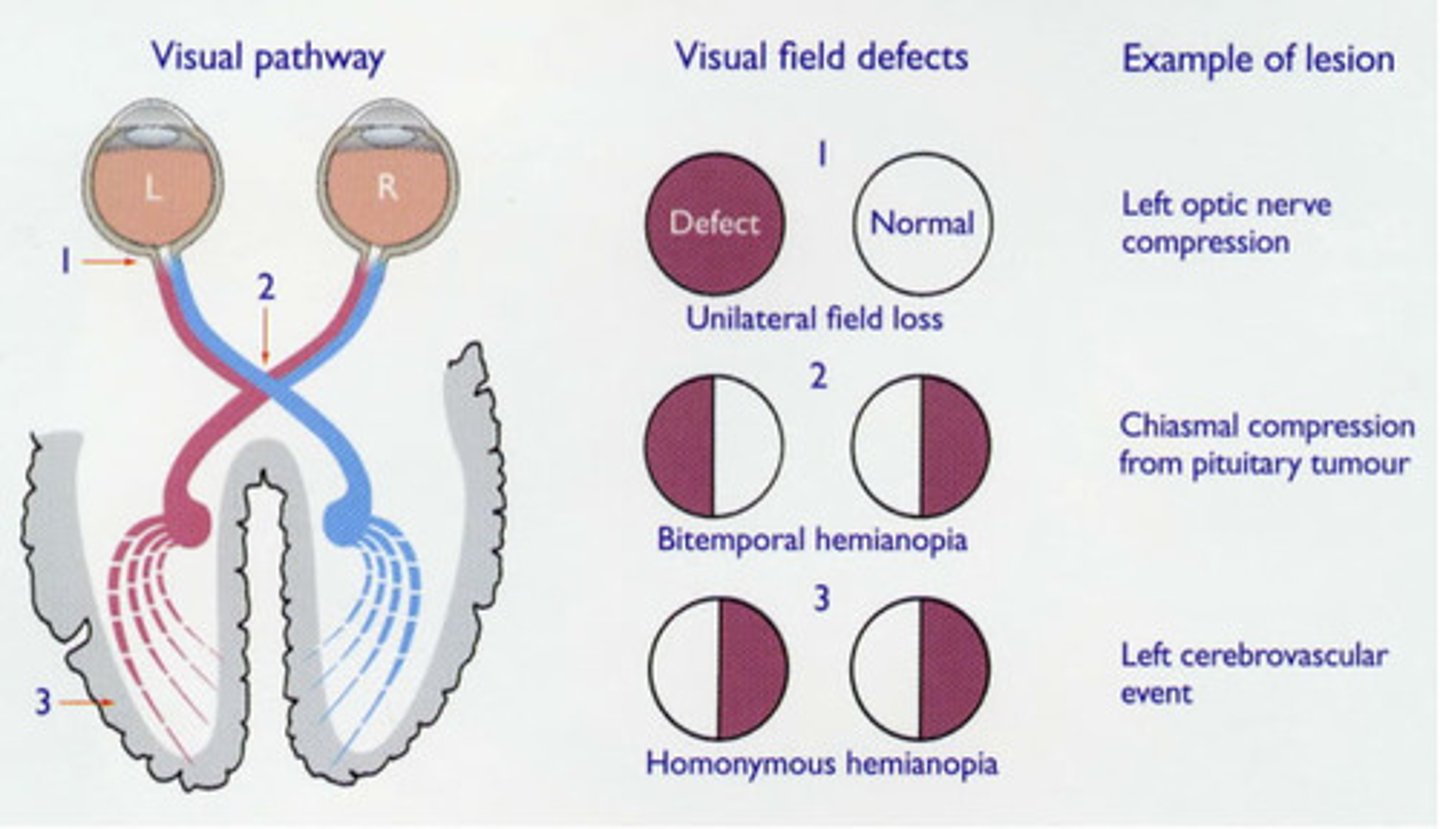
Visual field deficit: optic chiasm
Bitemporal heminopia (tunnel vision)
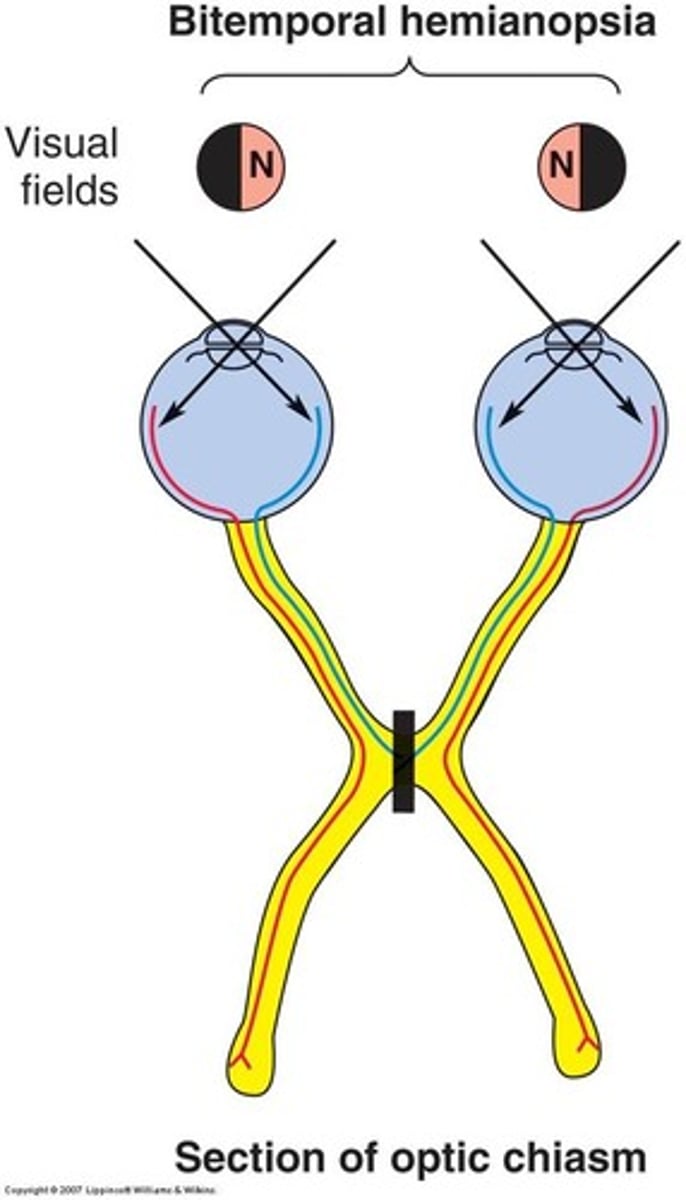
What are some possible causes of a lesion @ the optic chiasm?
Pituitary tumor
Visual field deficit: R optic tract
Contralateral (L) homonymous hemianopia (loss of opposing visual fields on both eyes)
NOTE: this picture depicts a lesion @ L optic tract
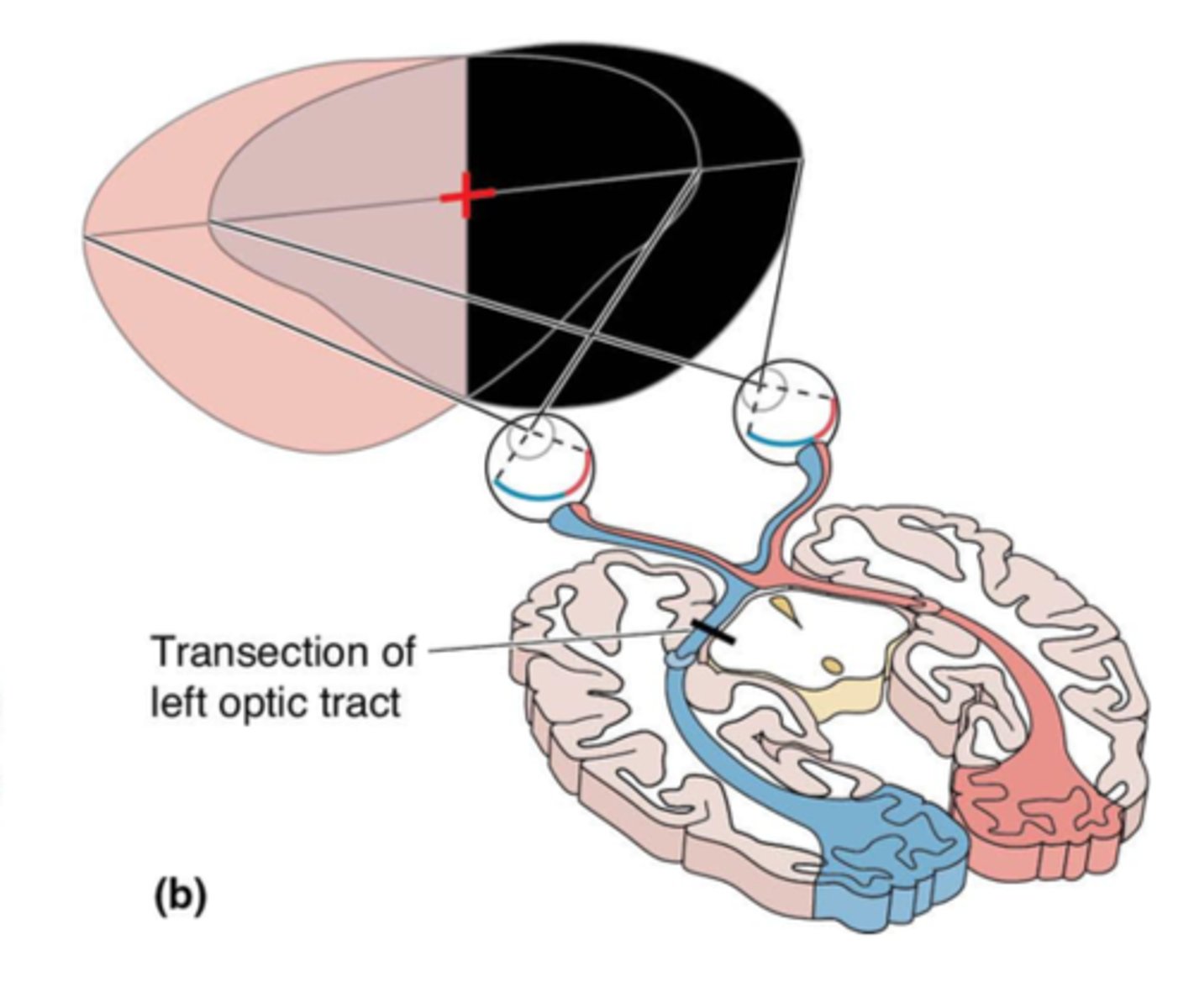
What are some possible causes of a lesion @ optic tract?
Tumors, demyelination, infarcts
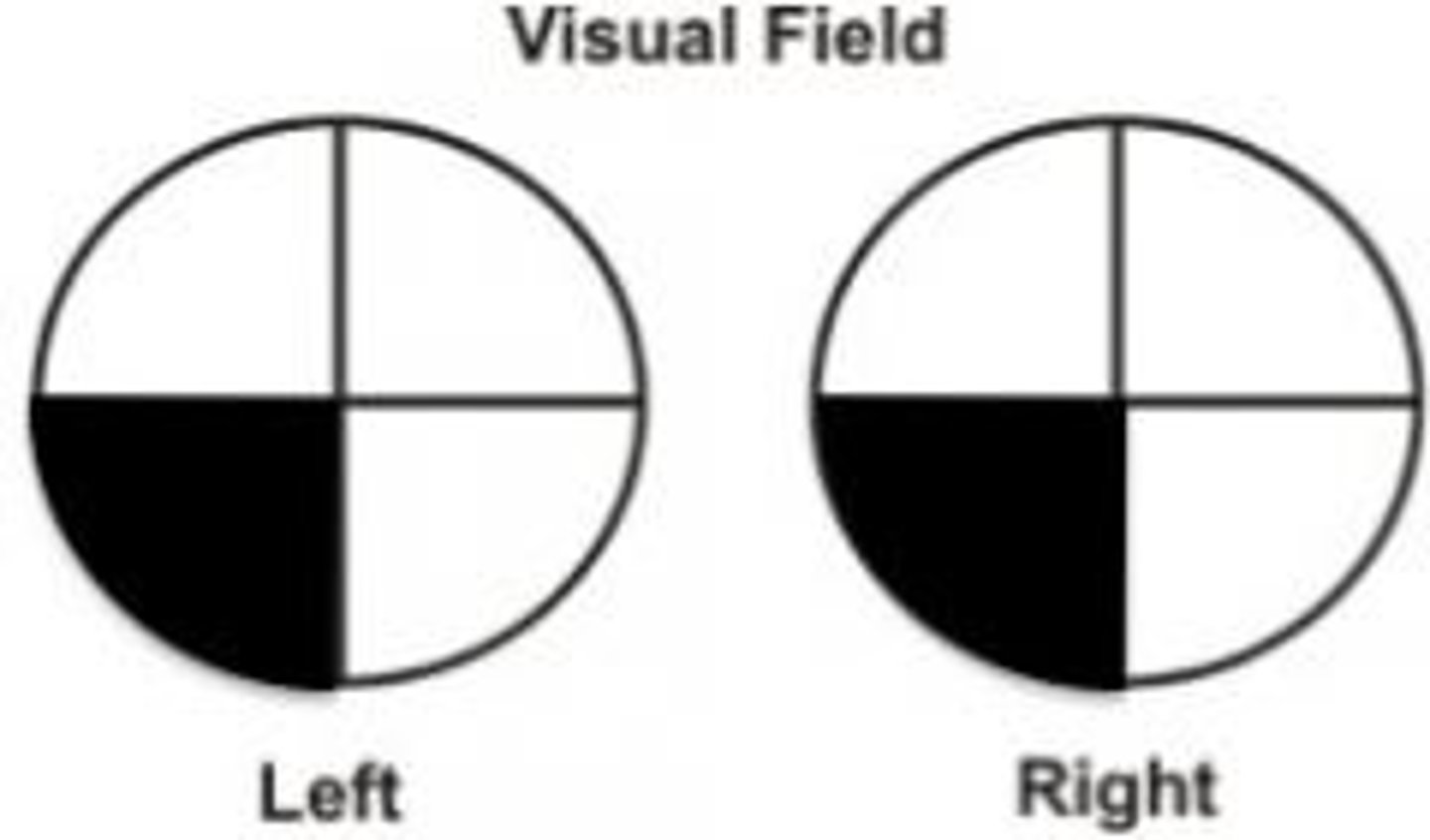
Visual field deficit: inferior optic radiations on R or inferior bank of calcarine fissure on R
Contralateral (L) superior quadrantanopia
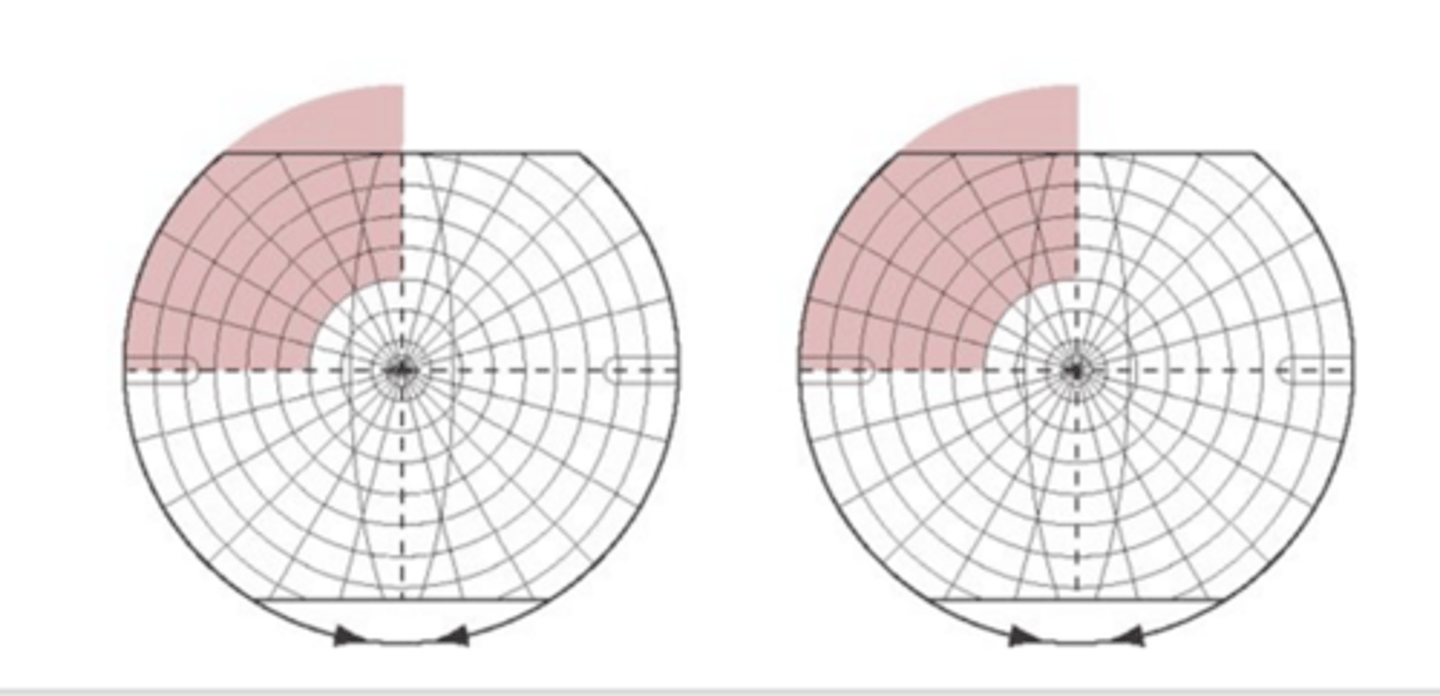
What are some possible causes of a lesion @ inferior optic radiations or lingula
MCA inferior division infarct, temporal lobe lesion/damage
Visual field deficit: superior optic radiations on R or superior bank of calcarine fissure on R
Contralateral (L) inferior quadrantanopia
What are some possible causes of a lesion @ superior optic radiations or superior bank of calcarine fissure
MCA superior division infarct, parital lobe lesion/ damage
Visual field deficit: both optic radiations on R OR entire primary visual cortex on R
Contralateral (LEFT) homonymous hemianopia
NOTE: the image depicts damage to the LEFT side
What are some possible causes of a lesion @ both optic radiations on R or entire primary visual cortex on R
MCA stem or PCA infarct, occipital lobe lesion/damage
If fibers reroute from the LGN, where do they go instead? (hint: these are our extrageniculate pathways)
Pretectal area and/or superior colliculus (both are in the midbrain)
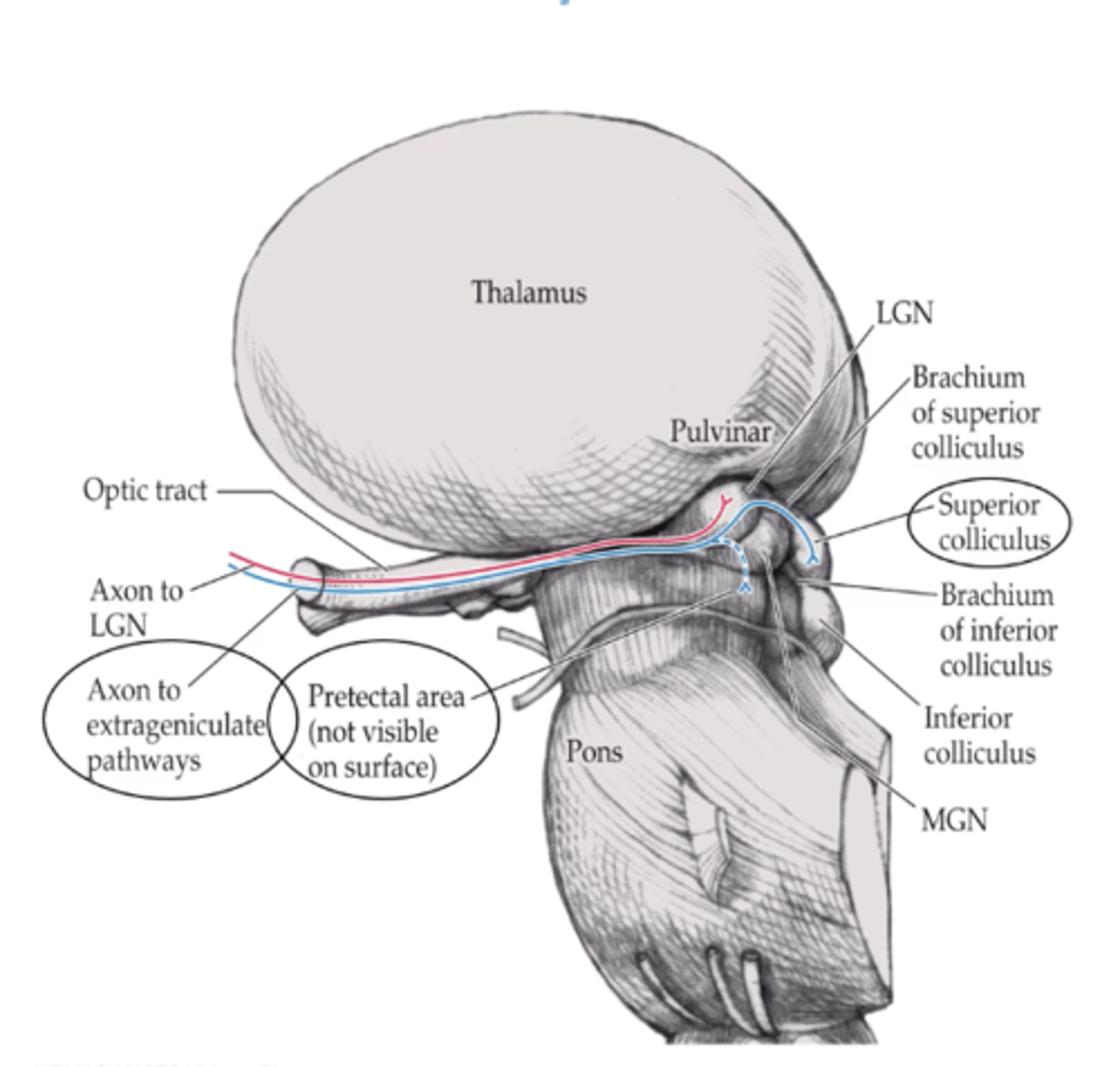
What are the 2 functions of the extrageniculate pathways?
Project to frontal eye fields to direct pupillary eye reflex & direct visual attention and eye movements