Neurological Disorders Objectives
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
Sundowning (select all that apply)
a. specific type of agitation
b. patient becomes more confused & agitated in late afternoon or evening - may be due to disruption of circadian rhythms
c. create a quiet, calm environment, maximize exposure to daylight, evaluate meds, limit naps & caffeine, consult HCP on drug therapy
Ischemic stroke
Occurs when there is inadequate blood flow to a part of the brain due to partial or complete occlusion of an artery
Thrombotic stroke
A blood clot forms at the site of injury to a vessel wall, narrowing the lumen; often associated with HTN, diabetes, & preceded by TIAs
Embolic Stroke
Occurs when an embolus lodges in & occludes a cerebral artery; results in infarction & edema of area supplied by involved vessel
Symptoms/Manifestations of an Embolic Stroke (select all that apply)
a. sudden onset with severe clinical manifestations
b. warning signs are less common
c. patient usually remains conscious
d. prognosis is r/t amount of brain tissue deprived of blood supply
Non-modifiable Risk Factors for Stroke (select all that apply)
a. Age: stroke risk increases with age, doubling each decade after 55 years old
b. Gender: more common in men, but more women die from stroke, oral contraceptives can cause clots
c. Ethnicity or race: African Americans have twice the incidence of stroke & a higher death rate from stroke compared to any other ethnic group
d. Family history or hereditary: at higher risk if a family member has had one
Dementia Etiology (select all that apply)
a. Caused by treatable & untreatable conditions.
b. The most common causes are neurodegenerative conditions that cannot be reversed - DLB &FTLD
c. Vascular disorders (multi-infarct dementia) is the second most common cause - ischemic or hemorrhagic brain lesions, ↓ blood supply to brain, may be cause by CVA or multiple
Early Stage or Mild Dementia (select all that apply)
a. Onset is slow & hidden from family
b. Short-term memory impairment, especially with new learning
c. Forgetfulness & poor judgment.
d. Loss of initiative & interests
e. Geographic disorientation, difficulty driving
f. Small personality changes
g. Loses ability to plan & organize
Late Stage or Severe Dementia (select all that apply)
a. Little memory, unable to process information
b. Unable to perform self-care: immobile, incontinence
c. Difficulty or unable to eat or swallow
d. Cannot understand words & often unable to talk
e. Will need total care
Dementia Complications
Dysphagia, aspiration pneumonia, UTIs, & injury from falls/wandering
AD Complications
Dysphagia (risk for aspiration & pneumonia), risk for infection, risk for impaired skin integrity, elimination problems
Stroke Planning & Outcomes (select all that apply)
a. Maintain stable or improved LOC
b. Attain maximum physical functioning
c. Maximize self-care abilities & skills
d. Maintain stable body functions
e. Maximize communication abilities
f. Maintain adequate nutrition
g. Avoid complications of stroke
h. Maintain effective personal & family coping
i. Teach families early warning signs & strategies for home care
Stroke Risk Reduction
Promote healthy diet, weight control, regular exercise, no smoking, limit alcohol, routine health assessment, manage risk factors, ASA commonly used prophylactically in high-risk patients
What is the extent of a stroke dependent on? (select all that apply)
a. rapidity of onset
b. size of area damaged
c. presence of collateral circulation
d. where in the body it is happening & how much blood it supplied to the brain
Modifiable Risk Factors for Stroke (select all that apply)
a. HTN: #1 modifiable risk factor
b. diabetes: 5x higher risk than general population
c. smoking: doubles the risk
d. obesity, sleep apnea, metabolic syndrome, lack of physical diet, drug & alcohol abuse
Transient Ischemic Attack (TIA)
Brief short-lived episode of neurologic dysfunction without acute infarction of the brain. TIAs may be due to micro emboli that temporarily blocks blood flow to the brain. WARNING SIGN of pending thrombotic stroke (is a medical emergency). Treat with Aspirin.
Signs & Symptoms of Stroke
Dependent on the location of the lesion. Common signs include altered LOC, weakness, numbness, paralysis, speech/visual disturbances, severe headache, unequal pupils, HTN, facial drooping, & difficulty swallowing
Manifestations of Right-Brain Stroke (select all that apply)
a. Paralyzed left side hemiplegia
b. Left-sided neglect
c. Spatial-perceptual deficits
d. Tends to deny or minimize problems
e. Rapid performance, short attention span
f. Impulsive - safety problems
g. Impaired judgement
h. Impaired time concepts
Manifestations of Left-Brain Stroke (select all that apply)
a. Paralyzed on right-side hemiplegia
b. Impaired speech/language aphasias
c. Impaired right/left discrimination
d. Slow performance, cautious
e. Aware of deficits; depression, anxiety
f. Impaired comprehension r/t language, math
Motor Function Impairment (select all that apply)
a. Mobility
b. Respiratory function
c. Swallowing & speech
d. Gag reflex
e. Self-care abilities
Characteristic Motor Deficits (select all that apply)
a. Akinesia: Loss of skilled voluntary movement
b. Impairment of integration of movements
c. Alterations in muscle tone
d. Alterations in reflexes: changes from hyporeflexia to hyperreflexia
d. contralateral effects
Types of Aphasia (select all that apply)
a. Receptive: loss of comprehension
b. Expressive: inability to produce language
c. Global: total inability to communicate
Dysphasia (select all that apply)
a. Impaired ability to communicate
b. Non-fluent: minimal speech activity with slow speech
c. Fluent: speech is present, but it makes no sense
Dysarthria
A problem with the muscular control of speech, impairment may involve pronunciation, articulation, & phonation
Stroke: Affect (select all that apply)
a. Difficulty controlling emotions
d. Emotional responses may be exaggerated or unpredictable
c. Depression & feelings associated with changes in body image & loss of function can make this worse
Stroke: Intellect (select all that apply)
a. Both memory & judgment may be impaired as a result of stroke
b. Although impairments can occur with strokes affecting either side of brain, some deficits are r/t hemisphere in which stroke occured
Stroke: Elimination (select all that apply)
a. Initial incontinence
b. Immobility & muscle weakness leads to constipation
c. Inability to express needs & manage clothing
Spatial Perceptual Alterations (select all that apply)
a. Deny illness or own body parts
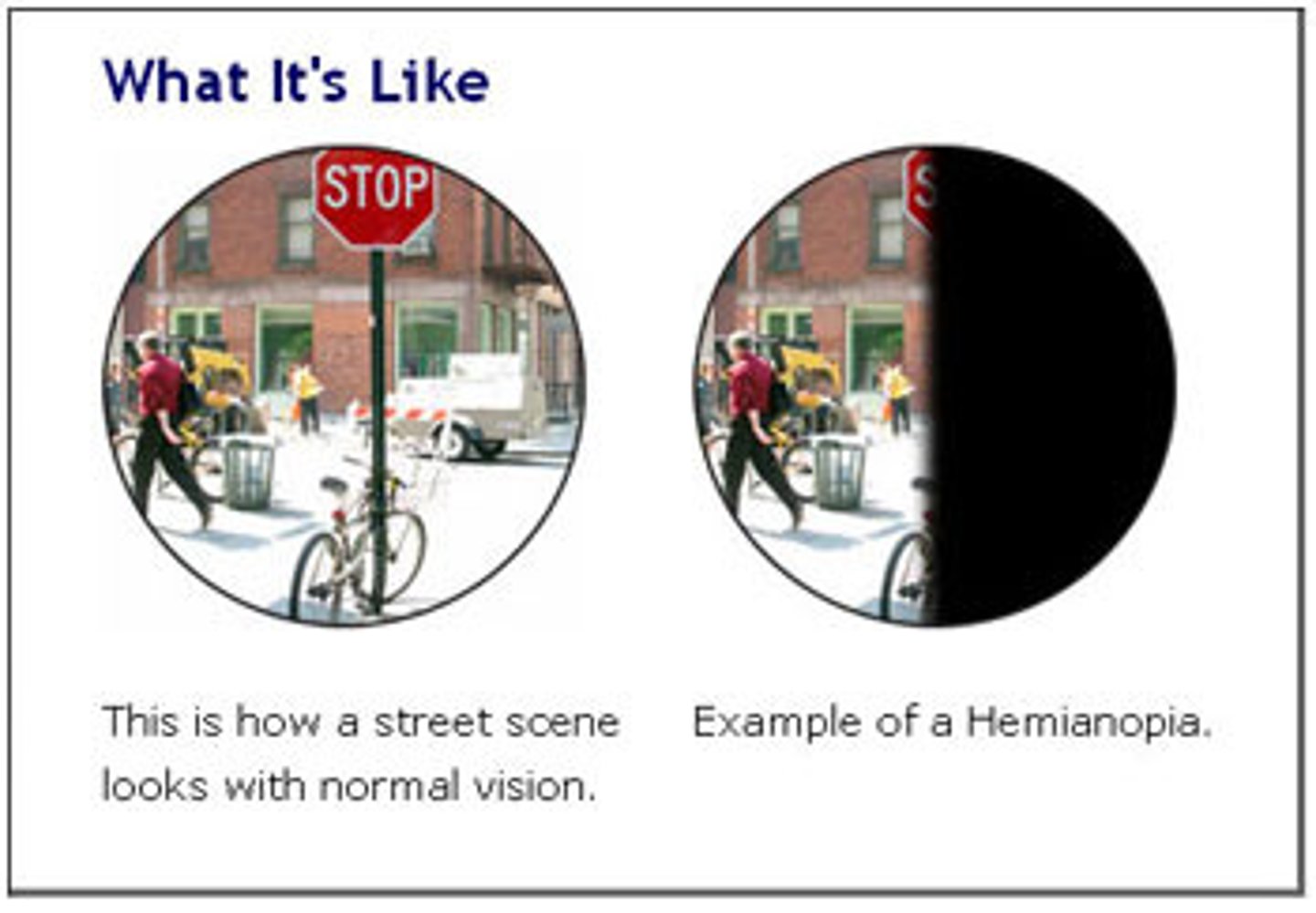
b. Spatial neglect: hemianopsia
c. Agnosia: the inability to recognize an object by sight,
touch, or hearing
d. Apraxia: inability to carry out learned sequent movements on command
Complications of Stroke
Increased intracranial pressure (ICP), aspiration pneumonia, venous thromboembolism (VTE), & joint contractures
Medical Management of Stroke
Reestablish blood flow using tPA (activase) within 3 to 4 hours of onset. Other treatments include ASA (24-48 hours post onset), platelet inhibitors, anticoagulants, & stent retrievers
Nursing Care of Stroke
Initial focus is determining the onset of symptoms. Maintain airway, keep NPO until a swallow evaluation is completed, monitor neuro/cardiac status, & implement VTE/ skin breakdown prophylaxis
Delirium Etiology
Exact cause unknown. A main contributing factor is impaired cerebral oxidative metabolism, multiple neurotransmitters abnormalities may be involved, cholinergic deficiency, excess release of dopamine, & both increased & decreased serotonin activity
Delirium Pathophysiology
A state of confusion that develops over days to hours; the patient has decreased ability to direct, focus, sustain, & shift attention & awareness
Delirium Risk Factors(select all that apply)
a. Demographic characteristics: age 65 or older, male gender
b. Cognitive status: cognitive impairment, dementia, depression, history of delirium
c. Decreased oral intake: dehydration, malnutrition
d. Drugs: alcohol or drug use or withdrawal, aminoglycosides, anticholinergics, opioids, sedative-hypnotics, treatment with multiple drugs, vasopressors
e. Environmental: admission to ICU, pain (especially untreated), restraint use, sleep deprivation, stress
f. Functional status: functional dependence, history of falls, immobility
g. Medical problems: acute infection, sepsis, fever, chronic kidney or liver disease, electrolyte imbalances, fracture or trauma, hemodynamic instability, history of stroke, HTN, hypoxia, neurologic disease, severe acute illness, terminal illness
h. Sensory: sensory deprivation, sensory overload, vision or hearing impairment
i. Surgery: cardiac surgery, noncardiac surgery, orthopedic surgery, prolonged cardiopulmonary bypass
DELIRIUM: Mnemonic for Causes (select all that apply)
a. Dementia, dehydration
b. Electrolyte imbalances, emotional stress
c. Lung, liver, heart, kidney, brain
d. Infection, ICU
e. Rx drugs
f. Injury, immobility
g. Untreated pain, unfamiliar environment
h. Metabolic disorders
Signs & Symptoms of Delirium (select all that apply)
a. decreased ability to focus
b. impaired memory & judgment
c. rapid or incoherent speech
d. irritable, restlessness
e. loss of appetite
f. later manifestations: agitation, misperception, misinterpretation, hallucinations
Medical Management/Nursing Care of Delirium
Treat underlying causes; provide a safe/calm environment, frequent reorientation, & avoid restraints
Dementia Pathophysiology
A decline from the previous level of function in 1 or more cognitive domains: complex attention, executive function, language, learning & memory, perceptual-motor, & social cognition
Middle Stage or Moderate Dementia (select all that apply)
a. Impaired ability to recognize close friends & family
b. Wandering
c. Forgets how to do simple tasks
d. Decreased ability to comprehend
e. Inability to write
f. Neglects hygiene
g. Agitation, restlessness
h. Delusions, hallucinations
i. Behavioral problems
j. Sundowner's syndrome
Dementia Medical Management
Improving or controlling decline in cognition, controlling undesirable behavioral manifestations or symptoms they're having, & providing care for the caregiver
Dementia & AD Nursing Care
Focus on maintaining functional ability, providing a safe environment, & meeting personal care needs while maintaining dignity. Use distraction & redirection for agitation
Alzheimer's Disease Etiology
Don't know the exact cause, likely a combination of multiple factors such as aging (> 65), family history, cardiovascular factors, head trauma
AD Pathophysiology (select all that apply)
a. Changes in brain structure & function.
b. Amyloid plaques buildup first in the hippocampus, eventually spreading to the cerebral cortex causing inflammation.
c. Neurofibrillary tangles are twisted threads composed of tau protein which support the internal structure of neurons - in AD this protein changes causing the structure to collapse & tangle.
c. As plaques & tangles accumulate, they prevent brain cells from communicating leading to widespread cell death, causing the brain to atrophy (shrink).
Dementia & AD Risk Factors
Age, family history, genetics, CV factors (diabetes & HTN), head trauma. Higher incidence in African Americans, Hispanics, & women.
AD Medical Management
No cure exists; medications aim to control decline
Stroke Diagnostic Studies (select all that apply)
a. Non-contrast CT or MRI is essential to differentiate between ischemia & hemorrhagic stroke.
b. Other tests include CTA, MRA, & cerebral angiogram.
c. The NIH Stroke Scale (NIHSS) is the primary tool for documenting neuro status & severity.
Dementia & AD Diagnostic Studies (select all that apply)
a. No definitive test for AD exists except for autopsy. b. Evaluation includes screening tests for cognitive function, ruling out depression, & labs/neuroimaging.
c. PET scans can differentiate AD from other forms of dementia.
d. Neuropsychological testing like MMSE or mini-cog documents the degree of impairment.
Delirium Diagnostic Studies
Confusion Assessment Method (CAM) & laboratory tests (CBC, electrolytes, liver/thyroid function) to find precipitating causes
Glasgow Coma Scale
Used to assess the degree of impaired consciousness by scoring eye opening, verbal response, & motor response. It allows multiple providers to reach the same conclusion regarding a patient's status
Stroke Nursing Diagnoses (select all that apply)
a. Decreased intracranial adaptive capacity
b. Risk for aspiration
c. Impaired physical mobility
d. Impaired verbal communication
e. Unilateral neglect
f. Impaired swallowing
g. Situation low self-esteem
Dementia & AD Nursing Diagnosis (select all that apply)
a. Impaired memory
b. Self-care deficit
c. Risk for injury
d. Wandering
d. Injury from falls
e. Ingesting dangerous substances
f. Injury to others & self with sharps
g. Burns
h. Inability to respond to crisis
Dementia & AD Overall Goals for Patients (select all that apply)
a. Maintain functional ability as long as possible
b. Be maintained in a safe environment with a minimum of injuries
c. Have personal care needs met
d. Have dignity maintained
Dementia & AD Overall Goals for Caregivers (select all that apply)
a. Reduce caregiver stress
b. Maintain personal, emotional, & physical health
c. Cope with long-term effects of caregiving
Patient/Discharge Teaching
Use the FAST acronym for stroke signs (face drooping, arm weakness, speech difficulty, time). Teach AD caregivers to not correct misstatements or faulty memory to reduce agitation.
Stroke/Aphasia Therapeutic Communication
a. Communicate often & meaningfully
b. Allow time for the patient to comprehend & answer
c. Use simple, short sentences
d. Use visual cues
e. Structure conversation so it allows simple answers by the patient
f. Praise the patient honestly for improvements with speech
Dementia & AD Therapeutic Communication (select all that apply)
a. Treat the adult with respect & dignity, even when behavior is childlike
b. Use gentle touch & direct eye contact
c. Remain patient, flexible, calm, & understanding
d. Expect challenging behaviors
e. Give directions using gestures or pictures
f. Simplify tasks. Focus on one thing at a time.
g. Avoid questions or topics that require extensive thought, memory, or words
h. Be flexible. If one approach does not work, try another.
i. Use distraction, changing the subject, redirecting to another activity
j. Provide reassurance
k. Praise sincerely for success
Delegation (select all that apply)
a. LPN/VN: Monitor behavior changes that may indicate physiologic problems, check environment for potential safety hazards, give enteral feedings to patients unable to swallow, if ordered, give ordered meds
b. Supervise AP: Help patients use toilet, commode, or bedpan frequently; provide personal hygiene, skin care, & oral care; help patients with eating; aid patients with daily activities; use bed alarms & surveillance to decrease risk for falls
Early Warning Signs of AD (select all that apply)
a. Memory loss that affects job skills
b. Problems with abstract thinking
c. Difficulty doing familiar tasks
d. Poor or decreased judgment
e. Problems with language
e. Misplacing things
f. Changes in mood & personality
g. Loss of initiative
Dementia & AD Safety/Risk Reduction (select all that apply)
a. minimize risks in home environment: assist caregiver in assessing home environment
b. implement all possible safety strategies: door alarms & high door locks, motion & sound detectors, medical alert bracelet or necklace, remove hazards
AD: Acute & Ambulatory Care (select all that apply)
a. AD patients subject to hospitalization for other problems - can precipitate worsening dementia, development of delirium
b. if early stages: reorient, maintain a consistent routine
c. if moderate to late stages: safety is a priority (can't reorient)
What are nursing strategies to address difficult behaviors for Dementia & AD?
Redirection, distraction, & reassurance (if in mild or early stages). Don't threaten to retrain or call HCP. Exhaust all options before using drugs.
Dementia & AD Caregiver Support (select all that apply)
a. AD disrupts all aspect of personal & family life
b. very stressful, caregivers exhibit adverse consequences
c. caregiving increases risk for development of dementia as chronic & severe stress affect hippocampus
d. assess caregiver expectations
Normal Forgetfulness (select all that apply)
a. sometimes misplaces keys, glasses, or other items
b. momentarily forgets an acquaintance's name
c. occasionally has to search for a word
d. occasionally forgets to run an errand
e. may forget an event from the distant past
f. when driving, may momentarily forget where to turn, but quickly orients self
g. jokes about memory loss
Memory Loss in Mild Cognitive Impairment (select all that apply)
a. frequently misplaces items
b. frequently forgets people's name & is slow to recall them
c. has increasing difficulty finding desired words
d. begins to forget important events & appointments
e. may forget recent events or newly learned information
f. becomes temporarily lost more often, may have trouble understanding & following a map
g. worries about memory loss, family & friends notice lapses
Memory Loss in AD Disease (select all that apply)
a. forgets what an item is used for or puts it in an inappropriate space
b. may not remember knowing a person
c. beings to lose language skills & may withdraw from social interaction
d. loses sense of time, does not know what day it is
e. has seriously impaired recent memory & difficulty learning & remembering new information
f. becomes easily disoriented or lost in familiar places, sometimes for hours
g. may have little or no awareness of cognitive problems
Acute Care of Patient with Stroke: Initial (select all that apply)
1. ABCs!
2. Ensure patent airway
3. Call stroke code or stroke team
4. Maintain adequate oxygenation
5. Assess BP & pulse ox
6. Obtain non contrast -CT scan or MRI immediately
7. Control fluid & electrolyte balance
8. Keep NPO
Donepezil
a. Classification: Anti-Alzheimers's agents, cholinergics (cholinesterase inhibitors)
b. Action: Inhibits acetylcholinesterase, thus improving cholinergic function by making more ACh available
c. Side Effects: Diarrhea, nausea, headache
Rivastigmine
a. Classification: Anti-Alzheimers's agents, cholinergics (cholinesterase inhibitors)
b. Action: Enhances cholinergic function by reversible inhibition of cholinesterase
c. Side Effects: Anorexia, diarrhea, N&V
Galantamine
a. Classification: Anti-Alzheimers's agents, cholinergics (cholinesterase inhibitors)
b. Action: Enhances cholinergic function by reversible inhibition of cholinesterase
c. Side Effects: N&V
Memantine
a. Classification: Anti-Alzheimers's agents, N-methyl-D-aspartate antagonist
b. Action: Binds to CNS N-methyl-D-aspartate (NMDA) receptor sites, preventing binding of glutamate, an excitatory neurotransmitter
c. Side Effects: HTN, diarrhea, headache
Fluoxetine
a. Classification: Antidepressants, SSRIs
b. Action: Selectively inhibits the reuptake of serotonin in the CNS
c. Side Effects: diarrhea, anxiety, headache, drowsiness
Sertraline
a. Classification: Antidepressants, SSRIs
b. Action: Inhibits neuronal uptake of serotonin in the CNS, thus potentiating the activity of serotonin. Has little effect on NE or dopamine
c. Side Effects: diarrhea, dry mouth, nausea, headache
Citalopram
a. Classification: Antidepressants, SSRIs
b. Action: Selectively inhibits the reuptake of serotonin in the CNS
c. Side Effects: abdominal pain, dry mouth, confusion, weakness
Haloperidol
a. Classification: Antipsychotics, butyrophenones
b. Action: Alters the effects of dopamine in the CNS.
Also has anticholinergic & alpha-adrenergic blocking activity
c. Side Effects: Blurred vision, dry eyes, constipation, dry mouth
Risperidone
a. Classification: Antipsychotics, mood stabilizers, benzisoxazoles
b. Action: May act by antagonizing dopamine & serotonin in the CNS
c. Side Effects: Itching/skin rash, dry mouth, nausea, dizziness, headache
Still learning (13)
You've started learning these terms. Keep it up!