Breast Pathologies, Complications of Menstruation, and WSW
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
Breast Abnormalities Requiring Evaluation
Breast Lumps and Masses
Breast lumps are the most common anomaly found on clinical and self-exam
Most benign but all need evaluation
Unilateral, hard, non-tender or fixed lumps suspicious for cancer
Skin Changes
Erythematous, scaly rash on nipple
Cyclic breast pain → especially related to menses, is benign and may not require imaging
Nipple discharge → bloody, persistent, spontaneous, unilateral warrants further wok up (labs and imaging, surgical consult)
Breast Imaging Screening
Mammogram for asymptomatic women
Craniocaudal view and mediolateral oblique view
Begin screening at 40 years old and screen annually
Women with breast implants should have regular mammographic screening
Dense breast tissue requires U/S
Only seeing one piece if only do mammogram
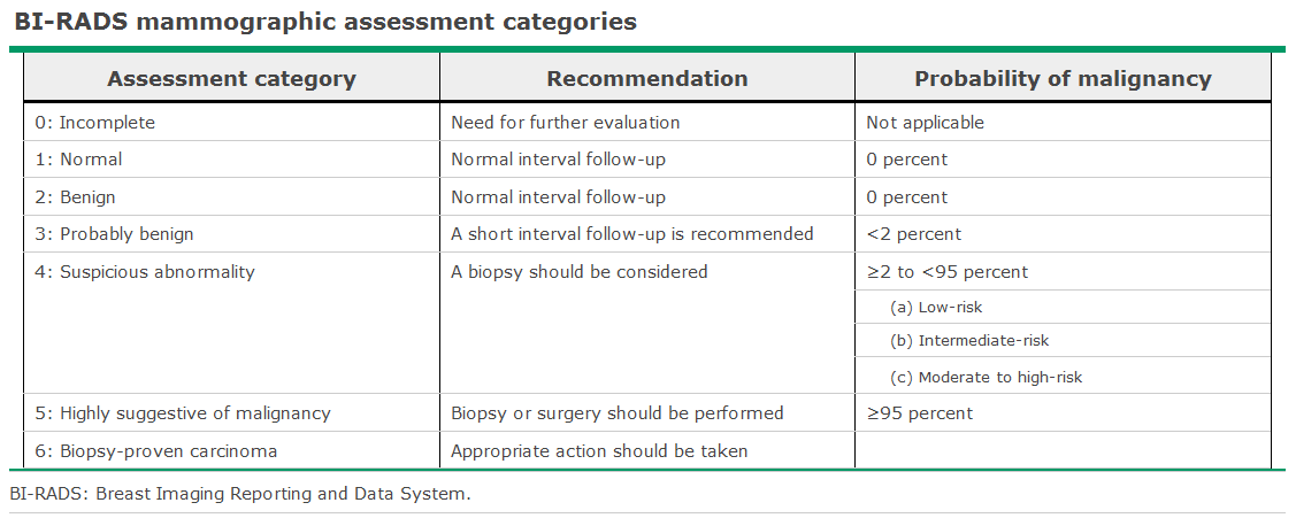
BIRADS 3 → probably benign
Follow up recommended but consider referral to breast specialist
Solid lesions need to be biopsied
Breast Imaging Diagnostic
Mammography for women with clinical symptoms or previous abnormal mammogram
Involves special views
BIRADS
Breast Imaging U/S
Most common imaging study after mammogram
Helps differentiate cystic vs solid mass
Aids in biopsy guidance
In patients with dense breasts → order both mammogram and U/S
Breast Imaging MRI
More sensitive for detecting breast cancers in women at high risk (mutation carriers)
MRI more sensitive than mammography or clinical exam but less specific
Determines architectural features, shape, margins, distortion, septations, and enhancement patterns
Breast Cancer Non-Modifiable Risk Factors (8)
Genetic mutations
Family history of breast cancer
Age (increases with > 50 y/o)
Menarche < 12 y/o
Menopause > 55 y/o
Dense breast tissue
Abnormal breast biopsy
Previous breast cancer
Breast Cancer Modifiable Risk Factors (11)
Nulliparity
First live birth > 30 y/o
Not breastfeeding
OCP use
Prolonged post-menopausal HRT
Obesity
Alcohol use
Tobacco
Sedentary lifestyle
High fat diet and processed foods
Radiation exposure
Breast Cancer Screening
Goals
Detect breast cancer at an early, more treatable stage
Reduce mortality rates by enabling early intervention
High risk individuals require earlier and more frequent screening
BRCA1/BRCA2 mutation carriers → start at 25-30 y/o with MRI and mammogram
Strong family history
History of chest radiation
Breast Cancer Risk Assessment: Tyrer-Cuzick Model
Estimates women’s lifetime and 10-year risk of developing breast cancer
> 20%: should have earlier and frequent screening
Gives percentage regardless of testing for genetic component
Breast Cancer Risk Assessment: Gail Model
Estimate’s 5-year and lifetime risk
Best for average risk women
Ductal Carcinoma in situ
Non-invasive
Abnormal cells confined to the milk ducts
Invasive ductal carcinoma
Starts in milk ducts but invades surrounding breast tissue
Most common type of invasive breast cancer
Infiltrating lobular carcinoma
Starts in lobules and spreads in a single file pattern
More likely to be bilateral
Inflammatory Breast Cancer
Instead of lump, causes breast swelling, redness, warmth, and skin dimpling due to lymphatic invasion
Most aggressive type
Abnormal Uterine Bleeding
Regular cycle length: 24-38 days
Polymenorrhea: < 21 days apart
Oligomenorrhea: > 35 days apart or fewer than 8-9 periods per year
Menorrhagia
Heavy menstrual bleeding: > 80 mL of blood loss per cycle or menstruation lasting longer then 7 days
Patient reports
Soaking through >= 1 pads/tampon every 1-2 hours
Needing to change protection during the night
Passing clots larger than 1 inch
Doubling up on pads or using extra protection
Symptoms of anemia
Metrorrhagia – irregular bleeding
Menometrorrhagia - heavy and irregular bleeding
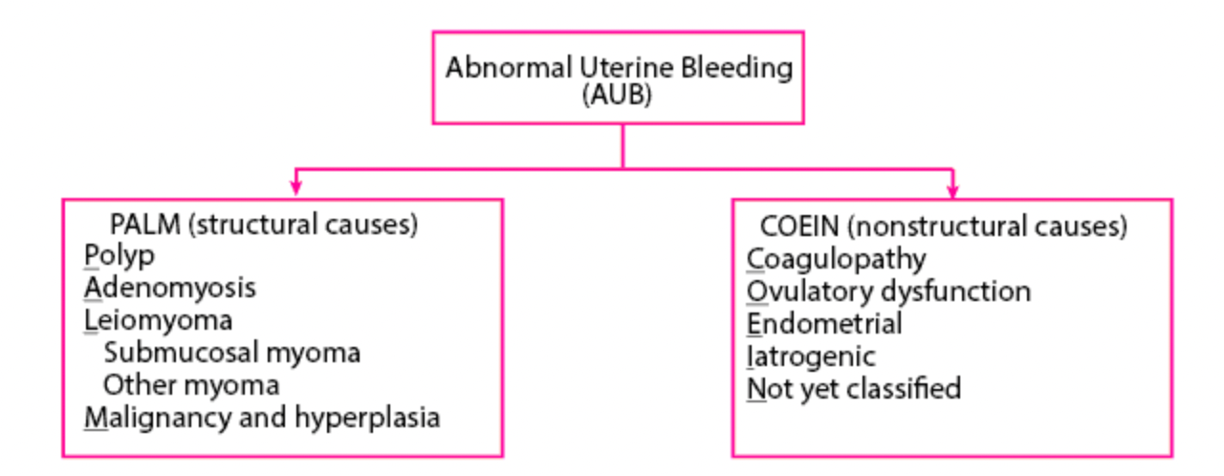
Abnormal Uterine Bleeding Classification
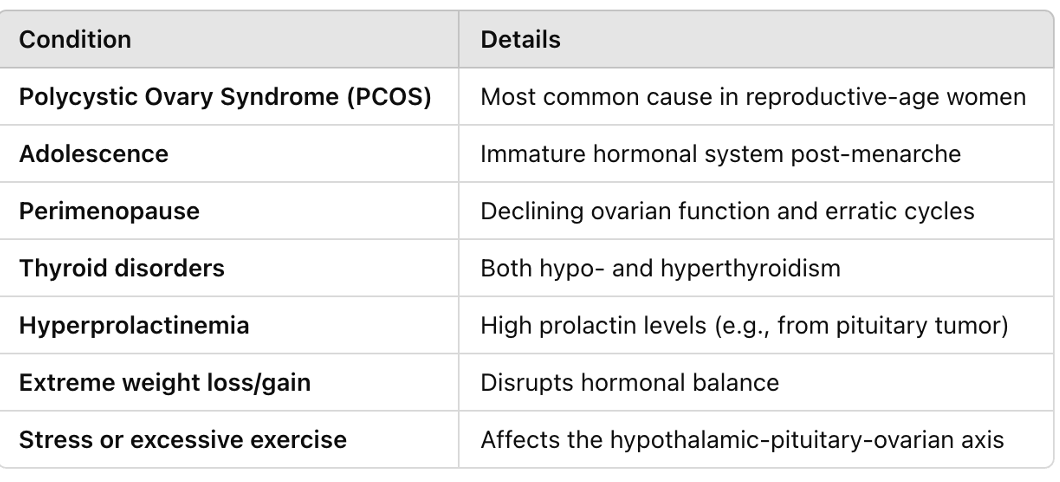
Causes of Abnormal Uterine Bleeding
Adolescence
Most common cause is anovulation → immature HPA
Coagulopathies
Reproductive Years
Once pregnancy ruled out:
Anovulatory cycles (MCC)
Infections
Complications of contraception
Medications: OCPs, corticosteroids
Systemic disease: hyperthyroidism, hypothyroidism, chronic renal failure, leukemia, malignancy
Undiagnosed von Willebrand
Endometrial polyps and fibroids
Perimenopause
Usually anovulatory
Erratic hormone levels
Malignancy (endometrial cancer)
Pregnancy: change of life baby
Medications
Systemic disease
Fibroids
Postmenopausal
Malignancy until proven otherwise (endometrial, cervical, uterine)
Abnormal Bleeding: Anovulation
No regular ovulation → hormone signals that regulate the menstrual cycle get disrupted → irregular, unpredictable, or heavy bleeding
Normal ovulation: ovary releases egg → progesterone produced, which helps stabilize the uterine lining, and without pregnancy progesterone drops and triggers predictable period
Anovulation: no ovulation means no progesterone → estrogen may build up the lining excessively and eventually the lining becomes unstable and sheds erratically or heavily
Causes
Abnormal Bleeding: Diagnosis and Management
Diagnosis
History
Age at menarche
Cycle of length
Inter-menstrual interval
Quantity of bleeding
Inter-menstrual bleeding
Medications
Physical → abdominal and pelvic exam
Labs
Serum hCG to r/o pregnancy
CBC with reticulocyte and platelet count to determine hemodynamic stability
Serum iron, TIBC, and ferritin
Coagulation tests
Thyroid function tests
BUN, creatinine
U/A and stool guaiac if source of bleeding is in question
Other labs depend on age, ovulatory status, risk of sexually transmitted infection and question of systemic disease
Pelvic U/S: cheap and easy
Endometrial biopsy: r/o polyps, hyperplasia, cancer
Need to r/o pregnancy first
Suction some of the cells with long instrument, pull back on tube, and going in and out and twisting
D and C: when endometrial biopsy contraindicated or inadequate or if symptoms persist beyond treatment
Hysteroscopy or direct visualization
Hysterosalpingography: requires x-ray and contrast dye to visualize the uterus and fallopian tubes
Important for patients with fertility issues: can see if fallopian tube is patent or not
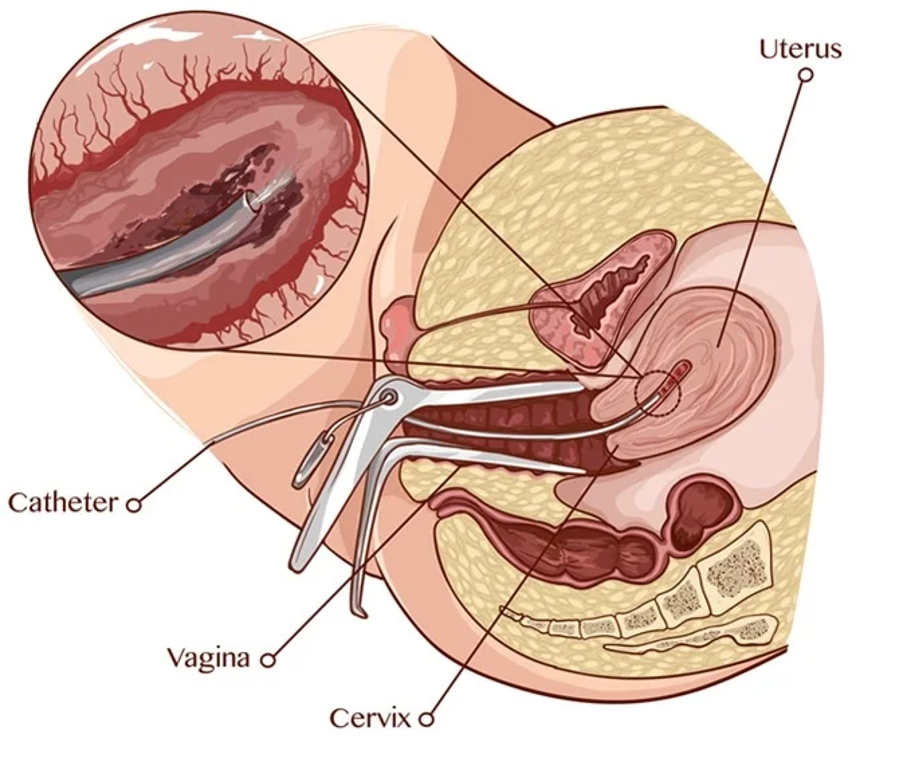
Saline infusion sonohysterography (SIS)
Saline infused into uterus through catheter and trans-vaginal ultrasound evaluates
Separation of cavity walls → better visualization of endometrium
Abnormal Bleeding: Management
Goals
Control bleeding
Prevent further episodes
Restore synchrony to endometrium
Replenish iron stores
Prevent serious long term consequences of anovulation
Preserve desired fertility
Depends on
Amount of bleeding
Cause of bleeding
Age of patient
Ovulatory status
Desire for fertility
Treatment
PALM-COEIN: treat the underlying cause
If due to ovarian anovulation
Combination estrogen-progesterone or cyclic progestin
If peri-menopausal → need to do endometrial biopsy to r/o neoplasia and consider hysterectomy
If patient not interested in fertility preservation can consider endometrial ablation
This is not a birth control option but causes significant scarring of the endometrium → not sustainable for pregnancy
Postmenopausal
Precancerous or malignant disease until proven otherwise
Benign causes like atrophic endometritis and polyps more common
All women with menorrhagia should be started on iron
Mild cases amenable to watchful waiting or treatment with NSAIDs
Abnormal Bleeding: Acute Heavy Bleeding Management
Check vital signs: may need hospitalization
IV fluids, transfusions as needed (hemoglobin < 7)
OCP pack
1 full pack, double up the first couple days to help stop bleeding
Do not put in if have risk of blood clots
Aygestin (norethisterone) → high dose progesterone
Give for 5 days - 1 week
Will see withdrawal bleeding
May be given to someone going in for a surgery to stop bleeding
Lysteda (tranexamic acid) → prevents enzymes in the body from breaking down blood clots
Taken just on period
Depo provera injection (medroxyprogesterone)
If no response to medical treatment within 12-24 hours → surgery
D and C
Balloon tamponade
Uterine artery embolization
Hysterectomy is rare and life saving only
Abnormal Bleeding: Chronic Management
Fix the underlying problem
Antifibrinolytic therapy
Lysteda 650 mg
2, 3, 5: 2 pills 3 times a day for 5 days
Contraindication if coagulopathy disorder
Coordinate endometrial sloughing
Best for anovulation
Progesterone for withdrawal bleed
Combination OCP, patch, or ring: can also provide withdrawal bleed
Endometrial suppression
To lighten bleeding and/or create amenorrhea
OCPs, POPs, Nexplanon
Extended cycle (seasonal, every 3 months menses, only bleed 4 times a year): OCPs, NuvaRing
Depo provera injection (medroxyprogesterone)
Levonorgestrel: IUD
Prevents ½ of women from hysterectomy
Very effective
Abnormal Bleeding: Refractory Prolonged Heavy Bleeding Management
Medical agents
GnRH antagonist: Danazol
GnRH agonists: Leuprolide
Last resort: produce medical menopause
May require surgery
D and C
Endometrial ablation
Hysterectomy
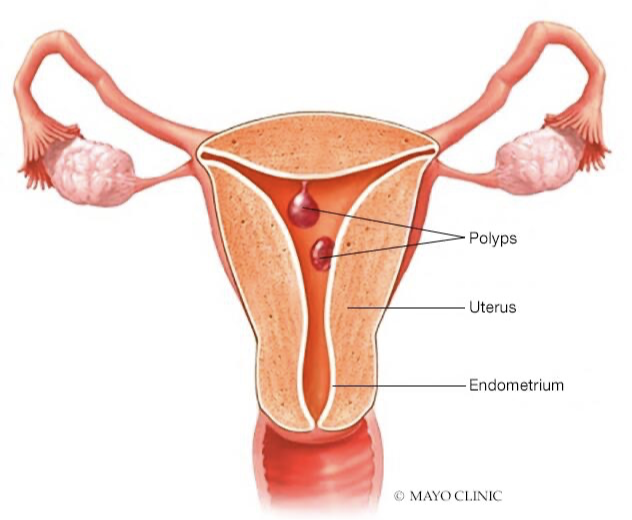
Abnormal Bleeding: Polyp
See inter-menstrual bleeding
Can often not be seen on exam: need pelvic exam or hysterectomy
Can use sonohysterography: separates endometrium to better see structural issues (may be difficult to see on U/S)
Endometrial biopsy may return fragments of polyp
Needs to be removed
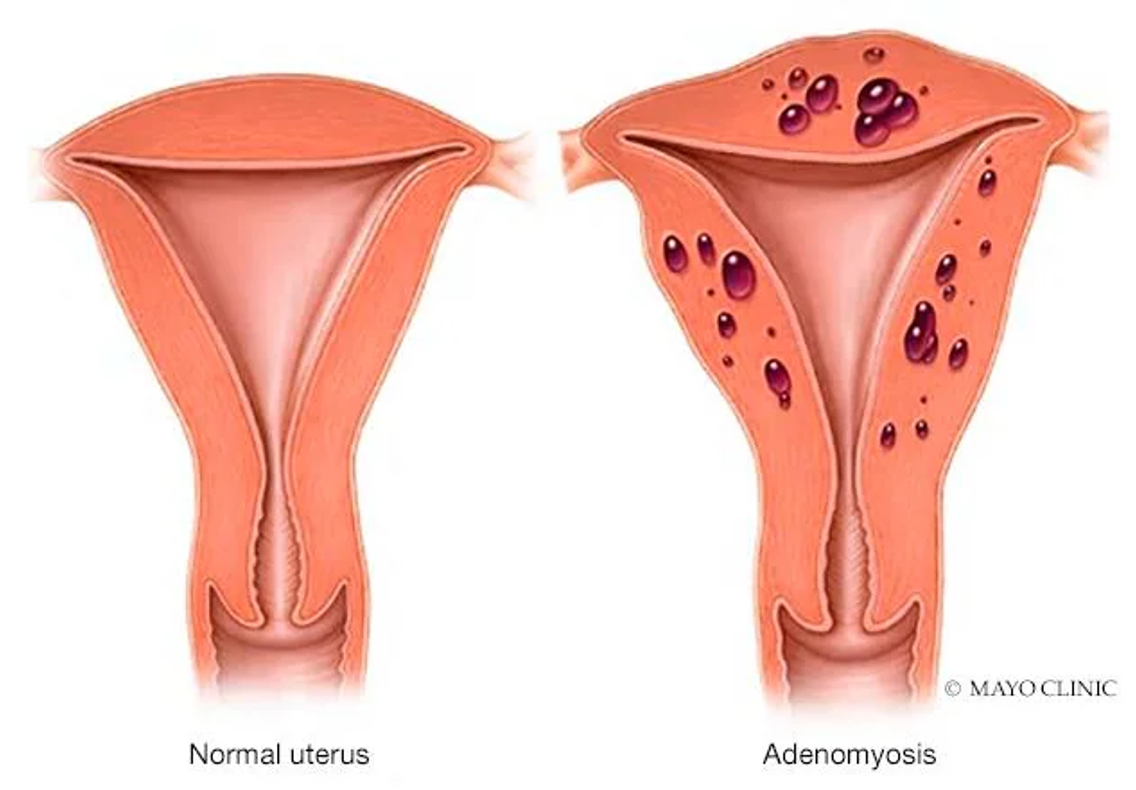
Abnormal Bleeding: Adenomyosis
Endometrial cells from the lining of the uterus grow into the muscle wall
Causes
Painful cramps
Heavy, prolonged menses
Dyspareunia
Boggy appearance/texture
Treatment
Depends on severity
Conservative
Hormonal methods
Hysterectomy
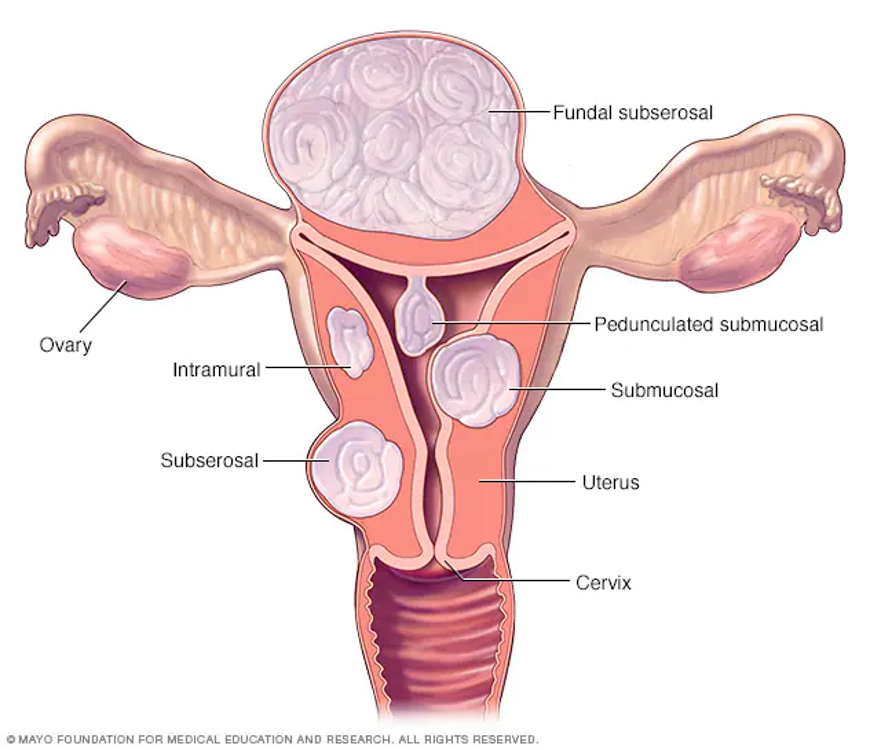
Abnormal Bleeding: Leiomyoma
Fibroids: tumors of uterine wall
Worry about submucosal: won’t be able to compress vessels well post-partum, which can lead to post-partum hemorrhage
Causes:
Heavy vaginal bleeding
Prolonged bleeding
Often asymptomatic
Treatment
Depends on severity
Hormonal methods
Myomectomy (removal of fibroids)
Uterine fibroid embolization
Hysterectomy
Abnormal Bleeding: Malignancy and Hyperplasia
Hyperplasia is precursor to uterine cancer
Any post-menopausal bleeding is a red flag
Should not see thickened lining (> 4 mm) on U/S in post-menopausal women
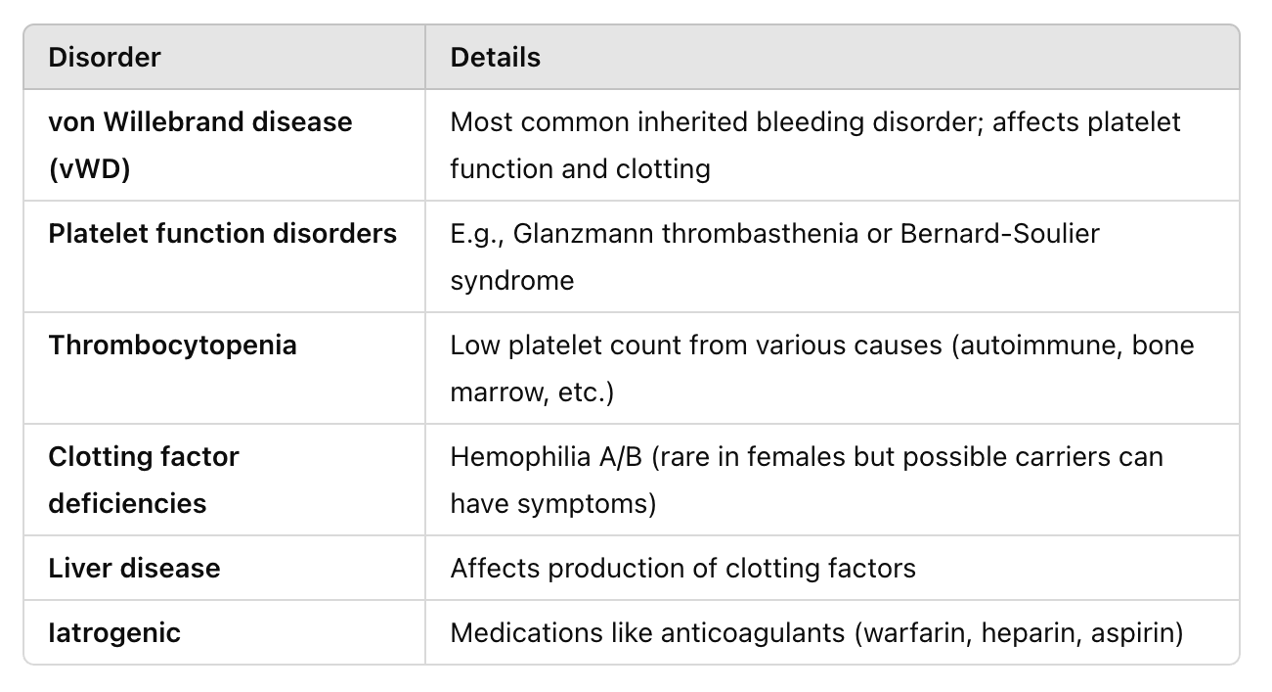
Abnormal Bleeding: Coagulopathy
Abnormal bleeding caused by a bleeding disorder
Von Willebrand Disease
The most common inherited bleeding disorder worldwide
Inadequate platelet adhesion and thrombus formation → easy bruising, frequent nose bleeds, bleeding gums, heavy menstrual periods, prolonged bleeding after cuts or surgery
Diagnostic labs
Decreased plasma vWD factor
Decreased VIII activity
Prolonged bleeding time
Treat with vasopressin (single infusion effective for minor bleeding episodes like menorrhagia)
OCPs effective for repeated, severe menorrhagia due to vWD
WSW Statistics
Lesbian and bisexual women report higher rates or certain diagnoses
Sexual minority of women have higher rates of forgoing or delaying medical care than heterosexual women
WSW are often under-screened for pap smears due to provider assumptions regarding lower risk of cervical cancer
Some are rarely asked about sexual orientation
Many fear negative experiences when disclosing sexual orientation
Five P’s
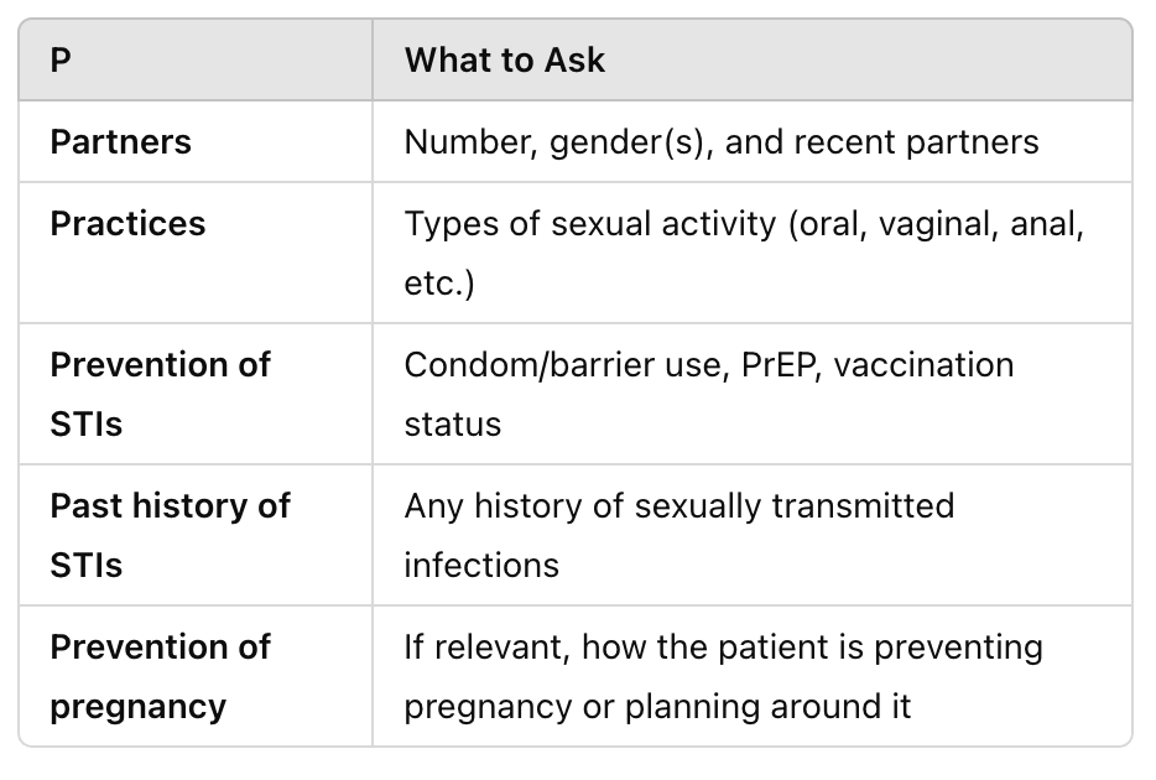
Sexual History Questions for All Patients
Are you sexually active with women, men, or both
How many sexual partners have you had in the past 5 years
Does your current partner have sex with women, men, or both
Describe your sexual contact
Is your sexual contact with someone who shared needed for injection drug use
During sexual contact do you use barrier methods
If active with men, what is your method of birth control
Do you or your partners have any history of STIs
Do you have any further concerns about sex or STIs
STI Transmission
Can occur through
Skin to skin contact
Mucosal contact
Digital/vaginal/anal contact
Shared penetrative sex toys
Oral-anal contact
Exchange of vaginal secretions or blood
Common STIs
HPV: most common STI
Transmitted skin to skin
Cervical cancer risk
HSV 1 and 2
Bacterial vaginosis
Very common
Not an STD but sexually associated due to disruption of normal vaginal flora
Trichomonas
Chlamydia and gonorrhea → less common via female to female transmission
Syphylis: increasing rates in women via oral/genital contact
HIV rare in female to female transmission
STI Predisposing Factors
Multiple sexual partners
Shared sex toys without cleaning/barrier use
Inconsistent barrier protection
History of male sexual partners
Substance use
History of sexual trauma
Misperception of low risk
Under screening by providers
STI Screening Recommendations
Screen based on behavior, not identity
Routine screenings
PAP/HPV
HPV vaccination
Chlamydia and gonorrhea
HIV screening at least once
Syphylis based on risk
Trichomonas
STI Prevention
Safe sex practices, as with any sexual contact between any gender
Use condoms on shared sex toys
Clean toys between use
Use dental dams for oral genital contact
Avoid sharing toys without barriers
Wash hands between genital contact
Cancer in WSW
Increased risk of
Ovarian cancer
They may not use hormonal contraceptives
Using OCPs for 5 years reduces ovarian cancer by 50%
Endometrial cancer
Nulliparity is a recognized risk factor for endometrial cancer
Breast cancer
Nulliparity, birth to only once child, and no history of breast feeding
Hormones released during pregnancy and breast feeding are thought to be cancer protective