Terms you need to know for Population Health and Epidemiology
Population Health
The health outcomes of a group of individuals and distribution of health outcomes within communities
Community-Oriented Primary Care (COPC)
focused on providing care to a defined population (combines primary care and population health)
Public Health
to promote and protect the health of people and the communities where they live, learn, work, and play
How many eras of public health?
Six eras
Health Protection Era (Antiquity-1830s)
Authority-based control
Hygiene Movement Era (1840-1870s)
sanitary conditions
Contagion Control Era (1880-1940s)
germ theory
Medical Care System Era (1950s-mid-1980s)
modification of risk factors
Health Promotion/Disease Prevention Era (mid-1980s-2000)
individual behavior and disease detection
Population Health (2000s)
coordination of public health and healthcare delivery
Three subsets of Population Health
Healthcare systems, traditional public health, and social policy
High Risk Approach
Focuses on those with the highest probability of developing the disease
Advantages of High Risk Approach
Strategy is tailored to the individual, patient and provider motivation, cost effective
Disadvantages of High Risk Approach
Temporary, doesn’t address underlying problem, more cases may arise
Population Approach
Focuses on entire population and aims to reduce the risk for everyone (improving the average)
Advantages of Population Approach
Large potential for societal impact, sustainable change, impact a range of health outcomes
Disadvantages of Population Approach
minimal benefit to individual, limited motivation, hard to implement, expensive
Social Determinants of Health (SDOH)
the conditions in which people are born, grow, live, work, and age
BIG GEMS
Behavior (smoking, physical activity)
Infection (can directly or indirectly cause some diseases)
Genetics (rarely the most important factor)
Geography (Malaria)
Environment (can be physical, built, or social)
Medical care (includes access and quality)
Socioeconomic-cultural
Three ways that SDOH can lead to different health outcomes
Quality of care
Access to healthcare
Life opportunities, exposures, and stresses
Socioeconomic Status
An individual’s position within a hierarchical social structure in relation to others, typically based on income, education, and occupation
Socioeconomic Gradient in Health
The poorest of the poor, around the world, have the worst health
Three ways Socioeconomic Status is measured
Education, Income, Occupation
Ways in which work can influence health (Clougherty, 2020)
social status and prestige, physical and chemical hazards, work organizations, work insecurity and unemployment, psychosocial job stressors, job demands, control, rewards received for efforts, gender and race differences
Racism
A system of structuring opportunity and assigning value based on the social interpretation of how we look (“race”)
Three levels of Racism
Institutionalized, Personally-mediated, Internalized
Six mechanisms linking Racism and Health
Institutional discrimination can restrict socioeconomic attainment and group differences in SES and health
Segregation can create pathogenic residential conditions
Discrimination can lead to reduced access to desirable goods and services
Internalized racism can adversely affect health
Racism can create conditions that increase exposure to traditional stressors
Experiences of discrimination may be a neglected psychosocial stressor
Health Disparities
Differences in the incidence and prevalence of health conditions and health status between groups
Health Disparities based on
Race or ethnicity, religion, SES, gender identity, sexual orientation, can think of others
Health Equity
the goal; the opportunity for everyone to attain his or her health potential
Difference between Health Disparities and Health Equity
Health equity is the goal and health disparities are the metrics we use to measure progress towards that goal
Health Inequities
Systematic and unjust distribution of social, economic, and environmental conditions needed for health
Epidemiology
The study of the distribution and determinants of health-related states in specified populations, and the application of this study to control health problems
Incidence
Counts new cases, measures risk
Prevalence
Counts all cases, measures burden
Risk Factors
Determinants increase the likelihood of a negative health outcome OR decrease the likelihood of a positive health outcome
Protective Factors
decrease the likelihood of a negative health outcome OR increase the likelihood of a positive health outcome
Salutogenesis
Factors that support human health and well-being
Pathogenesis
Factors that cause disease
Four uses of clinical epidemiology
Diagnosis, Prognosis, Prevention, Treatment
Diagnosis
screening and diagnostic tests
Prognosis
prediction of the course of disease (studies of survival)
Primary Prevention
prevent disease (addressing risk factors)
Secondary Prevention
early disease detection and/or intervention
Tertiary Prevention
reduce impact of diagnosis
Three elements of Biopsychosocial Model
Biological, Psychological, Sociological
Biological examples
physical health, disability, genetic vulnerabilities
Social examples
peers, family circumstances, school
Psychological examples
social skills, coping skills, self-esteem
Biosocial examples
drug effects
Biopsychological examples
temperament, IQ
Psychosocial examples
family relationships, trauma
5 levels of Social Ecological Model
Individual, Interpersonal, Institutional, Community, Societal
Individual level
targeted education (knowledge, attitudes, beliefs)
Interpersonal level
social marketing to change social norms (influence of family/friends)
Institutional level
policies and education (local politics, major regional employers)
Community level
advocacy groups (schools, churches, sports, clubs)
Societal level
policies and laws (cultural values, norms)
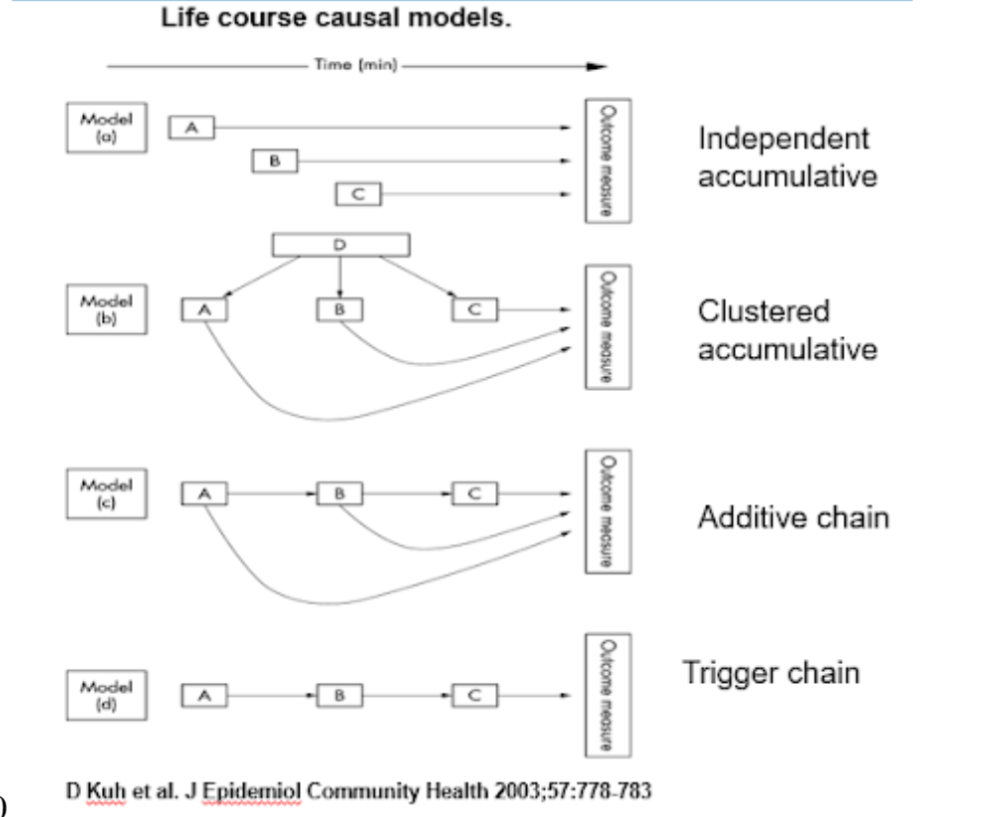
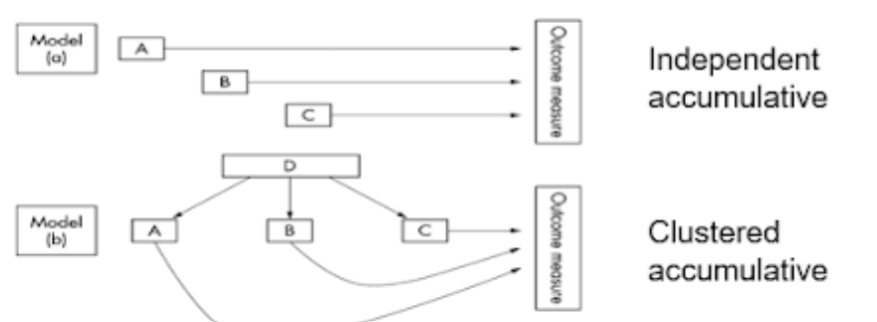
Life Course Theory
Health status reflects current and prior living conditions
The Life Course Theory includes
Chains of Risk, Accumulation of Risk, Critical and Sensitive Periods
Accumulation of Risk Model
Exposures or insults gradually build up
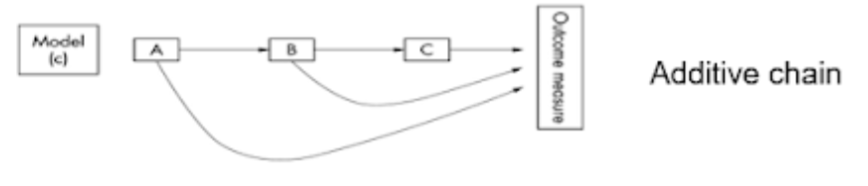
Chains of Risk Models
Sequence of linked exposures that raise or reduce disease risk
Chains of Risk: Additive Model
Each exposure increases the risk of subsequent exposure and has an independent effect on disease
Chains of Risk: Trigger Effect
Earlier exposures have no effect on disease risk without the final link in the chain
Critical Period
A limited time window in which an exposure can have adverse or protective effects on development and subsequent disease outcome
Sensitive Period
A time period when an exposure has a stronger effect on development and subsequent disease risk than it would at other times
Affordable Care Act - 2010
Aimed to lower health care costs, cover the uninsured and improve quality of care
Prevention and Public Health Fund
First mandatory funding dedicated to improving the public health system by improving health outcomes, enhancing healthcare quality, and restraining the growing healthcare costs
Four elements of National Prevention Strategy
Healthy and Safe Communities
Clinical and Community Preventive Services
Empowered People
Elimination of Health Disparities
Physical Activity Guidelines for Adults
150-300 minutes a week of moderate intensity aerobic physical activity or 75-150 minutes a week of vigorous intensity physical activity
Physical Activity Guidelines for School-Aged Children and Adolescents
60 minutes or more of moderate or vigorous intensity physical activity daily, muscle and bone strengthening at 3 days a week