Unit 2 - Range of Motion & Joint Integrity
1/270
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
271 Terms
Why is full joint range of motion (ROM) essential?
optimal human movement with less chance of injury
What usually limits movement?
joint structures such as the capsule or bone or by surrounding muscles
What should be done for accurate joint ROM testing?
any muscles that cross two or multiple joints should not be lengthened across all the associated joints
What is kinematics?
Human movement without consideration for the cause of the movement
subcategorized into arthrokinematics and osteokinematics
What is arthokinematics?
Movement of the joint surfaces in relation to one another; articulating bone ends roll, glide/slide, or spin on each other
What is osteokinematics?
Movement of the whole bone from rolling and sliding of the joint surfaces; type of motion measured by goniometry
typically occurs in three cardinal planes of movement with anatomical position as the reference point
What is AROM?
Arc of motion that occurs when the patient moves a joint through its available ROM without assistance from the therapist
What can limit AROM?
pain, weakness or lack of motor control/coordination (therefore must measure PROM also)
Why is it good to screen AROM?
a good musculoskeletal screening procedure to further focus the physical examination.
The amount, quality, and pattern of motion, as well as the occurrence of pain and crepitus, should be noted
What is PROM?
Arc of motion that occurs when the therapist moves the patient’s joint through its available ROM without assistance from the patient
Typically greater than AROM
What affects PROM?
integrity of joint surfaces and extensibility of surrounding soft tissues
Be sure to clearly document AROM vs. PROM to avoid confusion
What normally causes pain during PROM?
often due to moving, length ening, or pinching of noncontractile structures
Pain occurring at the end of PROM may be due to lengthen ing contractile structures and noncontractile structures
Pain during PROM is not due to the active shortening (contracting) of muscle and the resulting pull on tendon and bone attachments
What is end feel?
Characteristic feel to the resistance encountered at the end of normal PROM
What are the normal end feels? Abnormal?
Normal
Hard – bony and abrupt resistance felt at the end of PROM, no further motion can occur (e.g., elbow extension)
Firm – slight “give” felt at the end of PROM due to joint capsule and surrounding non-contractile tissue limitations at end range (e.g., shoulder flexion)
Soft – “mushy” resistance at the end of PROM due to soft tissue compression (e.g., elbow flexion)
Abnormal
empty, muscle spasm, springy block
What is reliability? How to maximize?
The overall consistency of a measurement, repeatability
To maximize reliability, always use the same instrument, positioning, procedure, and therapist (if possible)
What is validity?
The accuracy of a measurement; measuring what is intended to be measured
What affects validity?
poor stabilization of segments, alignment of goniometer as joint axis always moves during measurement
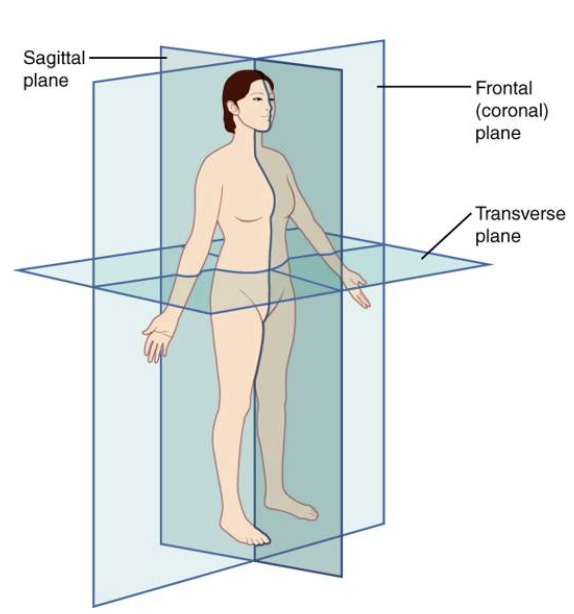
What is the sagittal plane? What movement occurs?
Vertical plane dividing body into right and left sides
“side view”
Flexion and extension occur in this plane
What is the frontal plane? What movement occurs?
Vertical plane dividing body into front and back halves
“front view”
Also known as coronal plane
Abduction, adduction, and spine lateral flexion occur in this plane
What is the transverse plane? What movement occurs?
Horizontal plane dividing body into upper and lower halves
“view from top of the head”
Medial and lateral rotation, pronation and supination occur in this plane
What is a goniometer?
Most widely used instrument for joint ROM measurements
Made of metal or clear plastic with large or small full circle or half circle central protractor calibrated in degrees
Consists of fulcrum, stationary arm, and moving arm
Arms can be used as rulers in in/cm for linear measurements as needed
What is an inclinometer?
Several different types, mechanical and electronic versions, consists of protractor and weight gravity pendulum
aka a bubble gonionmeter
Uses gravity as a reference point
Can be mounted onto a plastic frame
What are inclinometers used to most often measure?
range of motion of the lumbar, thoracic, or cervical spines, but they may be used for any joint, including the extremities
CROM: Cervical range of motion device; placed over patient’s head and secured with Velcro; able to measure all cervical spine movements
BROM: back range of motion device; secured to the patient with two elastic straps; able to measure all lumbar spine movements
Which is considered more accurate: goniometer or inclinometer? Why?
Inclinometers are generally considered to be more accurate because they provide numbers or digital values by being placed directly on the moving body part
Goniometers rely on proper alignment for both the stationary and moving components
What is almost always used to measure shoulder, hip, knee, and ankle motion?
goniometer or inclinometer
What is an electrogoniometer?
converts joint angular motion into an electrical signal
can measure multiple joint movements, but require skill to use; most often seen in research
What is a therabite?
measures temporomandibular joint ROM
What is a tape measure used for?
simple tool to measure ROM and muscle length
most commonly used to measure motion of the spine or the temporomandibular joint.
What is radiography?
gold standard of joint ROM measurement
routine use not recommended due to health risks of repeated exposure to radiation and high costs of procedure
What are smart phones used for in regards to ROM?
photography, video recording (becoming more common due to telehealth)
When are motion analysis systems used?
typically used in research due to high cost and decreased portability of the equipment
What is the single motion recording technique?
Separate documentation of individual joint ROM measurements, i.e., shoulder flexion, extension, abduction, adduction, etc.
Recorded as a range from beginning to end of the motion
What is normal shoulder flexion?
0-180º
What is normal shoulder external rotation?
0-80º (lacks 10º from AAOS standard of 90º)
What is normal elbow flexion?
5-150º (patient is unable to fully extend elbow for zero-degree starting point)
What is normal elbow extension?
-5º (patient is unable to reach elbow extension norm of zero degrees)
What is the two movement recording technique?
Recorded Together with Zero Degrees Between Motions to Denote Neutral Starting Point
Also known as the arc of motion for a joint
Examples for two movements recorded together
Shoulder internal to external rotation: 70-0-90
Elbow flexion and extension: 5-0-150 (patient is able to extend their elbow beyond the zero degree starting point and reaches full elbow flexion of 150 degrees)
What should you be sure to establish?
the zero-degree starting point so you know the patient’s entire range for the motion tested.
What factors affect ROM?
gender
age
build
culture, occupation, recreation
extensibility of skin and subcutaneous tissue
ligament and joint capsule laxity
What is the ROM procedure?
Explain to the patient how and why ROM measurements are performed (use layperson’s terminology)
Position the patient for optimal measurement accuracy
Ensure proper stabilization of the proximal bone/joint segment and support of the moving segment
Estimate PROM measurement and determine end-feel
Palpate bony landmarks and properly align goniometer
Read the goniometer and record the range of motion
Expand on step 1 more: Explain to the patient how and why ROM measurements are performed (use layperson’s terminology)
Show the patient the goniometer (or other measurement tool)
Explain the patient position for the measurements (use “on your back” instead of “supine”)
Keep this brief to avoid confusion, no need to explain the entire procedure from start to finish at this point in the evaluation (you can explain as you go)
Expand on step 2 more: Position the patient for optimal measurement accuracy
Position the patient for optimal measurement accuracy
Place the joint being measured in 0 starting position (may be 90º depending on the movement, e.g., shoulder internal rotation)
Ensure position allows for optimal stabilization of the proximal segment (e.g., humerus for elbow flexion)
Ensure bony landmarks for goniometer placement are properly aligned and can be palpated
Ensure the joint can move through its full available motion and is not blocked by internal (muscle tightness) or external (exam table) forces
Ensure that your patient can achieve the correct testing position; be prepared to modify but maintain alignment as much as possible. Document any difference in position for replication at future appointments or by different examiners if needed.
Expand on step 3 more: Ensure proper stabilization of the proximal bone/joint segment and support of the moving segment
Isolates joint motion to be measured
Prevents substitutions (e.g., lack of pronation may result in patient substituting with shoulder internal rotation and abduction; thus, therapist must stabilize humerus against the body to prevent substitutions during pronation ROM)
Lack of proper stabilization affects reliability of ROM measurement
See individual ROM techniques for specific stabilization and support information
Expand on step 4 more: Estimate PROM measurement and determine end-feel
Ask the patient to move through the desired AROM. Measure AROM if desired.
Move the joint through PROM using proper stabilization and support (see #3 above)
Gently push the part into the tissue resistance felt at the end of the motion to determine the "end feel"
Soft — soft tissue approximation, ie muscle compressing muscle
Hard — bony approximation
Firm — firm tissue resistance from contractile structures, joint capsule, ligaments and surrounding connective tissue
Visually estimate the range of motion in degrees and establishes the quality of the end-feel
State the AAOS standard (normal measurement in degrees) for the movement being measured (see Appendix B in Reese and Bandy textbook)
PROM helps patient understand the movement being performed and examiner to determine if any ROM limitations exist due to pain, tightness, or other causes.
Estimating the ROM helps novice therapist learn to properly read the goniometer
Expand on step 5 more: Palpate bony landmarks and properly align goniometer
Bony landmarks are used because their location does not change with movement
Identify three bony landmarks (at minimum) as targets for the fulcrum, stationary arm, and moving arm of goniometer
Fulcrum can move during ROM as joint axis is not stationary so ensure proper alignment of stationary and moving arms
Pre-set goniometer to estimated PROM from previous step, align with the joint motion being measured, and adjust moving arm reading as needed
Expand on step 6 more: Read the goniometer and record the range of motion
Once in the proper position, read the position of the moving arm on the goniometer scale to report the PROM of the movement being tested (be sure to read the correct scale)
Take the extremity into the opposite direction of the tested motion to establish a zero-degree starting position
Document the patient’s ROM with a beginning and ending point, such as 0-180º
If the patient does not have a zero-degree starting point, document their available range (e.g., unable to fully extend elbow, so elbow flexion measurement starts at 3º and reaches 150º with range reported as 3-150º of elbow flexion).
Expand on step 7 more: Interpretation
Were patient symptoms reproduced or was it painful? Location?
AROM- contractile or passive tissues implicated
PROM- passive tissues implicated
Compare quantity to the AAOS (or AMA) standard in degrees for the movement being measured
Note the end feel obtained for the PROM movement when overpressure is applied
Is it as expected? —> Soft, hard, firm
Not as expected: pathology?
Make note of quality of movement for PROM: was there clicking, crepitus, popping, smooth movement?
What is active assistive range of motion (AAROM)?
refers to when active motion is assisted often by the therapist but potentially also by a device, another person, or the patient themselves
What is gravity resisted range of motion?
Range of motion may be gravity resisted, meaning that the patient is working against the force of gravity to move the body part.
Ex: from the seated position as you lift your arm, the force of gravity is resisting you moving the weight of the part.
What is gravity assisted range of motion?
Range of motion can be gravity assisted, meaning that the patient is positioned in such a way that the force of gravity will move the part
Ex: if you lifted your arm while in the sitting position, the force of gravity will assist in the lowering of your arm. You only have to control it
What is gravity eliminated/minimized range of motion?
the movement occurs in a plane perpendicular to the force of gravity so that gravity is neither assisting or resisting the movement.
Ex: when a patient is too weak to perform an active motion, the therapist may place them in a position where gravity can assist the desired movement.
Gravity minimized motion can be utilized for a patient's strength levels as a progression of passive range of motion or as a progression of passive range of motion following surgery.
What is capsular pattern?
A joint-specific pattern of motion restriction that is due to impairment or pathology
Associated with pathology in the joint and/or capsular fibrosis
What is important to know in patient intervention?
Safety
Strength level
Correct assessment of patient impairments
Appropriate level of intervention
Why is (full) joint motion important in PT?
Joint motion is an integral part of human movement
Full joint motion allows the individual to move efficiently and with minimal effort
Full joint motion allows normal arthrokinematics
Full joint motion allows optimal human function for postures, movements and performance.
What is measured during a patient exam in regards to ROM?
all cardinal plane movements at a given joint
Why do PTs measure joint ROM?
To help determine causes of pain (body structure impairments)
To help identify potential causes of activity and participation limitations
To observe movement patterns that may contribute to inefficient mobility
To support the need for physical therapy intervention
To measure progress toward PT and patient goals
Normal PROM AAOS and AMA values for shoulder flexion?
AAOS: 0-180º
AMA: 0-180º
Normal PROM AAOS and AMA values for shoulder extension?
AAOS: 0-60º
AMA: 0-50º
Normal PROM AAOS and AMA values for shoulder abduction?
AAOS: 0-180º
AMA: 0-180º
Normal PROM AAOS and AMA values for shoulder medial rotation?
AAOS: 0-70º
AMA: 0-90º
Normal PROM AAOS and AMA values for shoulder lateral rotation?
AAOS: N/A
AMA: 0-90º
Normal PROM AAOS and AMA values for elbow flexion?
AAOS: 0-150º
AMA: 0-140º
Normal PROM AAOS and AMA values for elbow extension?
AAOS: 0º
AMA: N/A
Normal PROM AAOS and AMA values for forearm pronation?
AAOS: 0-80º
AMA: 0-80º
Normal PROM AAOS and AMA values for forearm supination?
AAOS: 0-80º
AMA: 0-80º
Normal PROM AAOS and AMA values for wrist flexion?
AAOS: 0-80º
AMA: N/A
Normal PROM AAOS and AMA values for wrist extension?
AAOS: 0-70º
AMA: 0-60º
Normal PROM AAOS and AMA values for wrist abduction (radial deviation)?
AAOS: 0-20º
AMA: 0-20º
Normal PROM AAOS and AMA values for wrist adduction (ulnar deviation)?
AAOS: 0-30º
AMA: 0-30º
Normal PROM AAOS and AMA values for first CMC joint flexion?
AAOS: 0-15º
AMA: N/A
Normal PROM AAOS and AMA values for first CMC joint extension?
AAOS: 0-20º
AMA: 0-50º
Normal PROM AAOS and AMA values for MCP joint flexion of the fingers?
AAOS: 0-90º
AMA: 0-90º
Normal PROM AAOS and AMA values for MCP joint extension of the fingers?
AAOS: 0-45º
AMA: 0-20º
Normal PROM AAOS and AMA values for MCP joint flexion of the thumb?
AAOS: 0-50º
AMA: 0-60º
Normal PROM AAOS and AMA values for MCP joint extension of the thumb?
AAOS: 0º
AMA: 0º
Normal PROM AAOS and AMA values for IP joint flexion of the thumb?
AAOS: 0-80º
AMA: 0-80º
Normal PROM AAOS and AMA values for IP joint extension of the thumb?
AAOS: 0-20º
AMA: 0-10º
Normal PROM AAOS and AMA values for PIP joint flexion of the fingers?
AAOS: 0-100º
AMA: 0-100º
Normal PROM AAOS and AMA values for PIP joint extension of the fingers?
AAOS: 0º
AMA: N/A
Normal PROM AAOS and AMA values for DIP joint flexion of the fingers?
AAOS: 0-90º
AMA: 0-70º
Normal PROM AAOS and AMA values for DIP joint extension of the fingers?
AAOS: 0º
AMA: N/A
Normal PROM values for thoracic and lumbar flexion: schober, goniometer, inclinometer?
schober: 3-5cm
goniometer: 90º
inclinometer: 60º
Normal PROM values for thoracic and lumbar extension: goniometer and inclinometer?
goniometer: 30º
inclinometer: 25º
Normal PROM values for thoracic and lumbar lateral flexion: goniometer and inclinometer?
goniometer: 30º
inclinometer: 25º
Normal PROM values for thoracic rotation: inclinometer?
30º
Normal PROM values for cervical flexion: tape measure, goniometer, inclinometer, crom?
tape measure: 1-4cm
goniometer: 45º
inclinometer: 50º
crom: 50º
Normal PROM values for cervical extension: tape measure, goniometer, inclinometer, crom?
tape measure: 20cm
goniometer: 45º
inclinometer: 60º
crom: 75º
Normal PROM values for cervical lateral flexion: tape measure, goniometer, inclinometer, crom?
tape measure: 15cm
goniometer: 45º
inclinometer: 45º
crom: 45ª
Normal PROM values for cervical rotation: tape measure, goniometer, inclinometer, crom?
tape measure: 10 cm
goniometer: 70º
inclinometer: 80º
crom: 70º
Normal PROM AAOS and AMA values for hip flexion?
AAOS: 0-120º
AMA: 0-100º
Normal PROM AAOS and AMA values for hip extension?
AAOS: 0-30º
AMA: 0-30º
Normal PROM AAOS and AMA values for hip abduction?
AAOS: 0-45º
AMA: 0-40º
Normal PROM AAOS and AMA values for hip adduction?
AAOS: 0-30º
AMA: 0-20º
Normal PROM AAOS and AMA values for hip medial rotation?
AAOS: 0-45º
AMA: 0-50º
Normal PROM AAOS and AMA values for hip lateral rotation?
AAOS: 0-45º
AMA: 0-40º
Normal PROM AAOS and AMA values for knee flexion?
AAOS: 0-135º
AMA: 0-150º
Normal PROM AAOS and AMA values for knee extension?
AAOS: 0-10º
AMA: 0º
Normal PROM AAOS and AMA values for ankle/foot dorsiflexion?
AAOS: 0-20º
AMA: 0-20º