Lecture 7: Sexual Function and Sex-Related Disorders
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
difficulties studying sexual behaviour
-private subject
-multiple axes of measurement - wide range of specific behaviours
inter-individual variation → diverse across individuals, cultures and time
intra-individual variation → varies within individuals e.g., life events, well-being
neural mechanisms underlying sexual behaviour
-hypothalamus
-critical for observable copulatory behaviours of rodents
-raises level of motivation engage in copulatory behaviour → sends excitatory signals to other cortical regions which then sends actions to motor systems
medial preoptic area (neural mechanisms underlying sexual behaviour)
-critical for male copulatory behaviour
-lesions or drug inhibition of this area abolish such behaviours in males → and also in females where some behaviours are observed
-stimulation of the MPAO elicits these behaviour
hypothalamus (neural mechanisms underlying sexual behaviour)
-critical for clearly observable copulatory behaviours of rodents
-ventromedial nucleus appears critical for the display of female copulatory behaviour
-electrical stimulation of VMN facilitates lordosis in response to a male
complication of neural mechanisms in animal models (underlying sexual behaviours)
-in animal models there are other functions and neural mechanisms apart from hypothalamus:
reward system → sexual rewards
olfactory circuits → pheromones and odours
lordosis circuits → back arched thanks to contraction reflex of the muscles
mice sex life (neural mechanisms underlying sexual behaviours)
-mice sing to each other as part of courtship
-chemical in the tears of juvenile mice deters female mice from copulation
complications of neural mechanisms in humans (underlying sexual behaviour)
-human sexual behaviour is more complex and multidimensional than that of other mammals
-the male-female binary has utility when we are thinking comparatively about sexual behaviour but this is a reductionist approach to a complex issue
Kinsey (early and foundational studies of human sexual behaviour)
-taxonomy of human sexual behaviour based on thousands of interviews
-studied types/frequencies of certain behaviours in the population
-shocking for the 40s
-widely cited despite statistical and sampling issues
Masters & Johnson (early and foundational studies of human sexual behaviour)
-detailed study of human sexual behaviour and sexual disorders in 50s/60s
-measured aspects of sexual intercourse and masturbation in a lab setting
-established highly influential 4 stage model for human sexual behaviour → sexual response cycle
desire, plateau, orgasm, resolution
-widely cited but has been revised
recent work (studies of human sexual behaviour)
-refined terminology, identified additional variability in ‘normal’ cycles and attempted to determine the neuroanatomical correlated of components of the cycle
-3 major components linked to distinct brain systems: wanting, liking and learning
-numerous fMRI studies of sexual function → however methodological limitations as in lab setting and cannot move head
wanting phase (studies of human sexual behaviour)
-cognitive planning to acquire sexual stimulus
liking phase (studies of human sexual behaviour)
-affective component
learning (studies of human sexual behaviour)
-can be good or bad
-plasticity that feeds into how people may approach sexual behaviour
sexual orientation (sexual behaviour)
-biological sex, gender identity and sexual behaviour
-animal models → interference with sexual differentiation can lead to displays of sexual behaviours typically associated with the opposite chromosomal sex and to same-sex preferences
-but limited translation to humans → no good lab model that encompasses the cognitive and emotional aspects of human sexuality
sexual differentiation models (sexual orientation)
-perinatal sex hormone exposure
-castration/ovariectomy
-lesioning of hypothalamic nuclei
sexual identity (sexual orientation)
-captures aspects of both gender identity and sexual orientation
fraternal birth order effect (sexual orientation)
-the more brothers a biological male has, the more likely they are to identify as homosexual
-15-29% of gay men may owe their sexual orientation to this
-robust across cultures
-older sisters or younger siblings have no effect
-effect remains if older brothers raised in different households but not for adopted or stepbrothers → implies the effect relates to maternal factors → maternal immunization hypothesis
maternal immunization hypothesis (FBOE)
-immune systems are linked to decreased or increased expression of certain chemical pathways
-suggests repeated exposure to male foetus leads to certain feedback cycle between the internal physiology of the womb and subsequent foetus that impacts on expression of sexual behaviours and identity
-very little understanding of why this happens
evidence against FBOE
-when analysed in a meta analysis with weighted studies, the specific association between the number of older brothers and homosexual orientation is small, heterogenous in magnitude and not specific to men
-existing research exaggerated by small-study effects
hormone factors (sexual orientation)
-some evidence suggests perinatal hormone exposure in humans can modulate same-sex/opposite sex preferences
neuroanatomical factors (sexual orientation)
-specific hypothalamic nuclei may play a role in sexual preferences
-there are differences in the sizes of these nuclei between homosexual/heterosexual males/females
genetic factors (sexual orientation)
-evidence from family/twin studies for a moderate genetic influence on sexual orientation
-up to 40% of variance in sexual orientation of males may have a genetic basis
-up to 20% of variance in sexual orientation of females may have a genetic basis
-several specific genetic markers associated with sexual orientation → but none were predictive of sexual orientation
gender bias in sex research
-typically done on males
-preferentially done on male animal models
argue that it avoids the complexity of the oestrogen/menstrual cycle → makes it easier to control variables in the study
defining sexual dysfunction or pathology
what is normal?
what is acceptable to others?
what is acceptable to oneself?
what is maladaptive?
deviation from statistical normality (defining sexual dysfunction or pathology)
-arbitrary
-relies on extensive and accurate data → hard to obtain in this area
-cross-cultural granularity
-ultimately subjective → what number of standard deviations from the mean constitutes abnormal?
deviation from social norms (defining sexual dysfunction or pathology)
-powerful influence on social judgement
-socially normal isn’t always adaptive or functional
-subjective perception of norms often differs from actual norms
-cultural and historical variation
-political influences
-circularity → norms can create and define pathology
distress (defining sexual dysfunction or pathology)
-a focus on emotional/psychological well-being
-persistence or frequency of distress may be important
-requires awareness and acknowledgement that some individuals may not experience distress
-social norms and the protection of others
deficits in normal function (defining sexual dysfunction or pathology)
-focus on social, interpersonal and occupational functioning
-maladaptive behaviours may not hurt self or others but could cause other problems in life
-some maladaptive responses may have reasonable basis → need to avoid unhelpful pathologising
-can cut across individual life choices
-can ignore individual experiences/impact
-interacts with social norms
sex and gender-related disorders
sexual dysfunction
paraphilic disorders
gender dysphoria
sexual dysfunction (sex and gender-related disorders)
-relates to problems with experiencing the human sexual response cycle
-types are categorised according to phases of the human sexual response cycle:
desire → male hypoactive sexual desire disorder
plateau → female sexual interest disorder, erectile disorder
orgasm → female orgasmic disorder, delayed ejaculation, early ejaculation
resolution → sexual pain disorders
diagnosing sexual dysfunction (sex and gender-related disorders)
-must be an impact on:
subjective distress
functioning
-symptoms must be persistent or recurrent
-concerns over pathologising intra or inter-individual differences
-more common in females but may be a gender bias in reporting problems
risk factors for sexual dysfunction (sex and gender-related disorders)
-gender related
-certain health conditions
-sexual abuse
causes (sexual dysfunction)
-may be psychological and/or biological
-hard to determine
treatments (sexual dysfunction)
-symptom focussed
-psychotherapy
-biological → drugs or devices
paraphilic disorders (sex and gender-related disorders)
-any intense and persistent sexual interest, other than sexual interest in genital stimulation or preparatory fondling with phenotypically normal physically mature, consenting human partners
-to qualify, satisfaction must entail either distress/harm to the individual or to another person
types of paraphilic disorders (sex and gender-related disorders)
not typically directed at another person → fetishistic disorder, transvestic disorder
directed at a non-consenting person → exhibitionist, frotteuristic, pedophilic, voyeuristic
involves experiencing or inflicting suffering → sexual mascochism and sadism disorders
risk factors (paraphilic disorders)
-being male
-hypersexuality
-pedophilic disorder:
past sexual abuse
attachment problems
psychiatric comorbidity
substance abuse
causes (paraphilic disorders)
-little understood
-possibly psychodynamic
-cognitive or biological factors may play a role
-most research focussed on pedophilic disorder
treatments (paraphilic disorders)
-behavioural techniques
-cognitive therapies
-hormonal or drug treatments
gender dysphoria (sex and gender-related disorders)
-disparity between an individual’s assigned gender and their perceived gender that causes distress or impairment
-often co-morbid with anxiety and depression
diagnosing gender dysphoria (sex and gender-related disorders)
marked and persistent cross-gender identification
significant distress or impairment
lack of physical intersex condition
psychological model (gender dysphoria)
-suggest that GD has a neurobiological basis but is closely associated with the individual’s interaction with the external world, their self perception and the feedback received in return
-introduced concept of ‘brain gender’ → gender identity-specific brain architecture and organisation
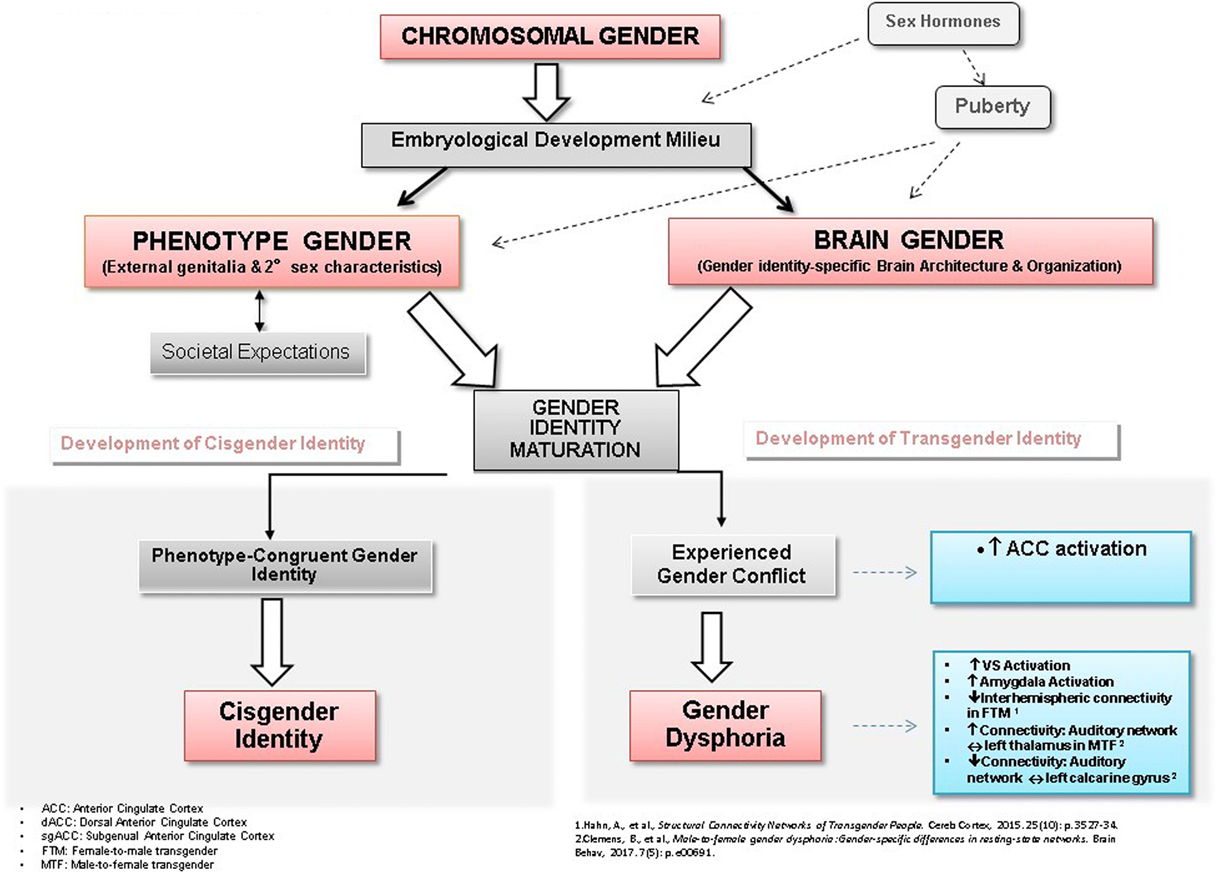
4 stages of gender identity (gender dysphoria - psychological model)
chromosomal gender
phenotypic gender
brain gender
experienced gender
issues with psychological model (gender dysphoria)
-possibly downplays environmental and brain plasticity aspects
-binary in nature → does not include consideration of non-binary gender identity
-causality regarding brain differences not well-established by the evidence
risk factors and causes (gender dysphoria)
-weak
-paternal relationship for males and childhood abuse for females
-little support for notion that parental attitudes or behaviours play a role
-biological factors may include in-utero hormone exposure
-evidence for differences in brain structures is mixed
-evidence from twin studies for heritability → no single gene found
treatments (gender dysphoria)
-psychological treatments → behavioural and cognitive
some success but clients often resistant
-gender reassignment surgery → often leads to satisfactory outcomes but may not alleviate other psychological co-morbidities