Spine - Spinal Cord & Pathology
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
brain and spinal cord
the CNS consists of the
cerebrum, cerebellum, brain stem
the brain consists of the
midbrain, pons, medulla oblongata
the brainstem consists of
meninges, cerebrospinal fluid, spinal column
medulla passes thru foramen magnum to become the spinal cord. It is protected by ______ and cushioned by _______ ______ & protected by the bony ________ ______
conus meddularis
pointed end of spinal cord
L1-2
where does the spinal cord end?
31
how many pairs of spinal nerves exit on both sides through the bony intervertebral and sacral foramina
cauda equina (horse tail)
refers to spinal nerves that extend from the conus thru the foramina to innervate the body and transmit sensory impulses back to the brain
epidural space
between the skull/vertebrae and dura mater
dura mater
tough outer meningeal covering
subdural space
between dura and arachnoid mater
arachnoid mater
delicate middle meningeal layer
subarachnoid space
below arachnoid and above pia mater, contains CSF
pia mater
delicate inner layer adhered to brain/cord; contains blood vessels
myelography
a surgical aseptic imaging of the spinal cord & nerve root branches with contrast injected into the subarachnoid space of the thecal sac to outline the spinal cord & nerves
subarachnoid space
into what part of the spinal cord is a myelogram injected
L3-4; C1-2
most common area for a lumbar puncture is ______ or sometimes ______
trendelenburg
pt placed in __________ position to move contrast to cervical and thoracic areas
hyperextended
pt’s neck will be ___________ to avoid contrast entering the cisterna magna behind brain stem (causes headache)
C2 and C6-7
most spinal fx occur where?
C1
least common spinal fx?
ligament/cord
MRI is best imaging for _________ injuries
61%
plain x-ray detects spine injury only ________ percent of the time

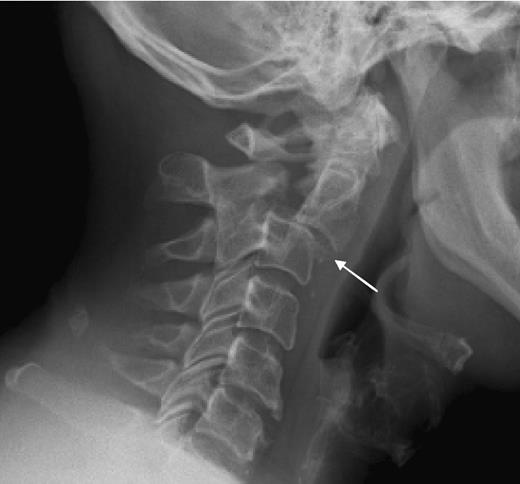
clay shoveler’s fx
avulsion fx of the spinous process C6-T1, results from hyperextension of the neck

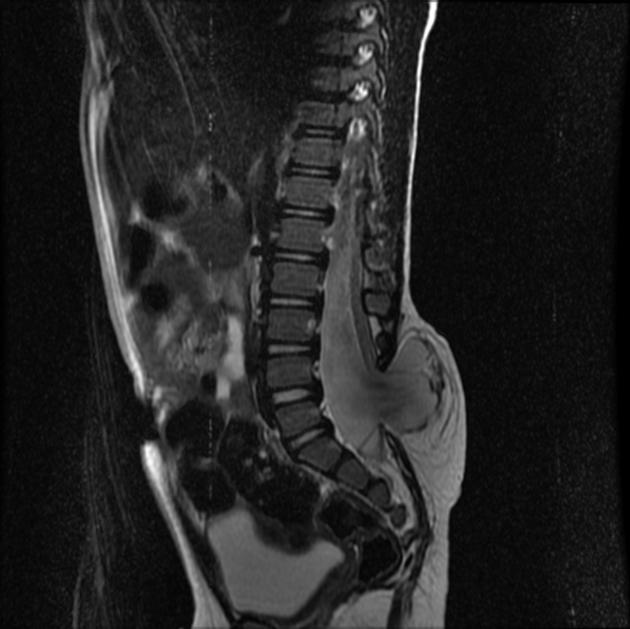
compression fx
collapse of body from osteoporosis, kyphosis, trauma, or pathologic disease. Anterior wedge collapses, changing the shape to a wedge, best demoed on a lateral spine

chance fx
fx through body & posterior elements of a vertebra (lap seat belt- not common anymore)
hangman’s fx
fx of anterior arch/pedicles of C2 w/ or w/o subluxation of C2 on C3, occurs w/ extreme hyperextension
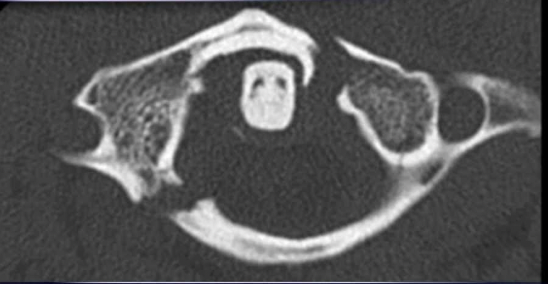
jefferson fx
fx of anterior and posterior arches of C1 caused by severe axial loading (fall on head), best demoed by open mouth views
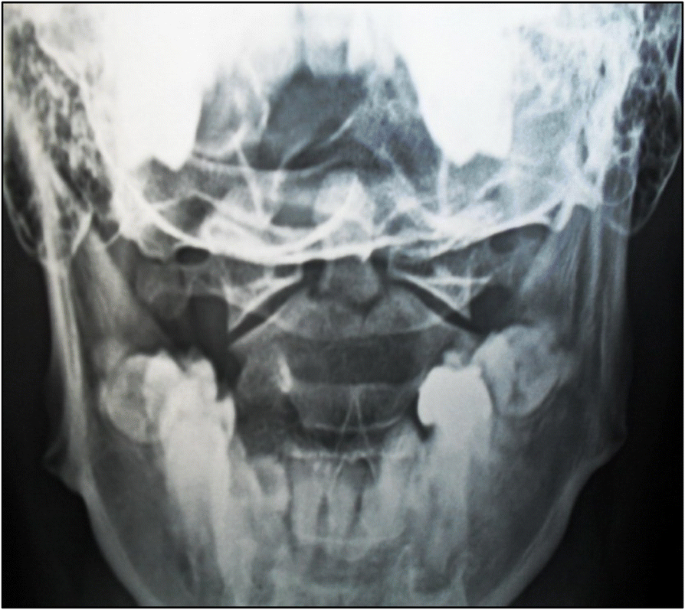
odontoid fx
fx of dens and/or lateral masses or arches of C2, demoed by open mouth view

teardrop fx
comminuted vertebral body w/ triangular fragments extending from body; caused by compression & hyperflexion of c-spine, best demoed on lateral or CT

unilateral subluxation of facet
1 zygapophyseal jt misaligned from overflexion, distraction & rotation during trauma

bilateral locks facet
if extreme subluxation, both zygapophyseal jts at same level can be disrupted, creating locked facets

herniated nucleus pulposus (HNP)
when nucleus pulposus protrudes through fibrous cartilage layer into spinal canal, presses on spinal cord or nerves causing pain & numbness in extremities, most frequently L4-5
sciatica
low back pain radiating down the leg due to HNP pressing on the sciatic nerve
scheuermann’s disease
common abnormal scoliosis & kyphosis, more common in young females
spondylitis
inflammation of vertebra
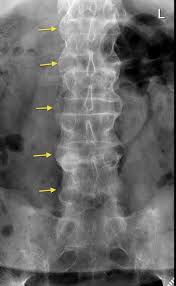
ankylosing spondylitis
systemic illness (predominantly in men 20-40) variant results in pain and stiffness in SI, intervertebral & costovertebral joints, along w/ abnormal union of spinal joints, complete rigidity of spine, usually seen in SI jts (bamboo spine)

spondylosis
neck stiffness from degeneration of disks, may affect the zygapophyseal jts and intervertebral foramen
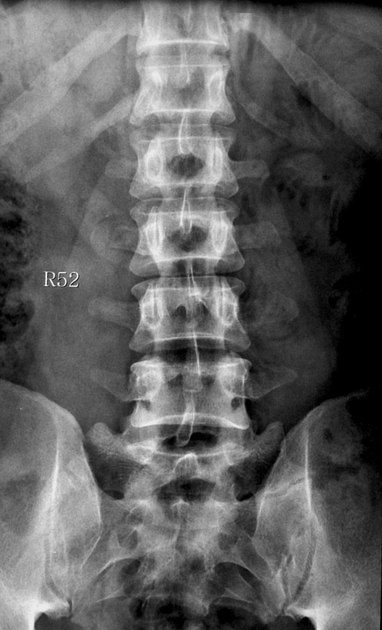
transitional vertebra
vertebra looks like adjacent spinal region (most common in LS region, or cervical/lumbar rib)

spina bifida
congenital; posterior aspects of vertebra don’t develop exposing part of the spinal cord (varies greatly in severity)
spina bifida occulta
mild form where there is a defect in the posterior arch of the L5-S1 vertebra without protrusion in the vertebra

meningocele
semi severe form of spina bifida; meninges protrude thru the undeveloped opening
myelomeningocele
most severe form of spina bifida where meninges and spinal cord protrude through the opening
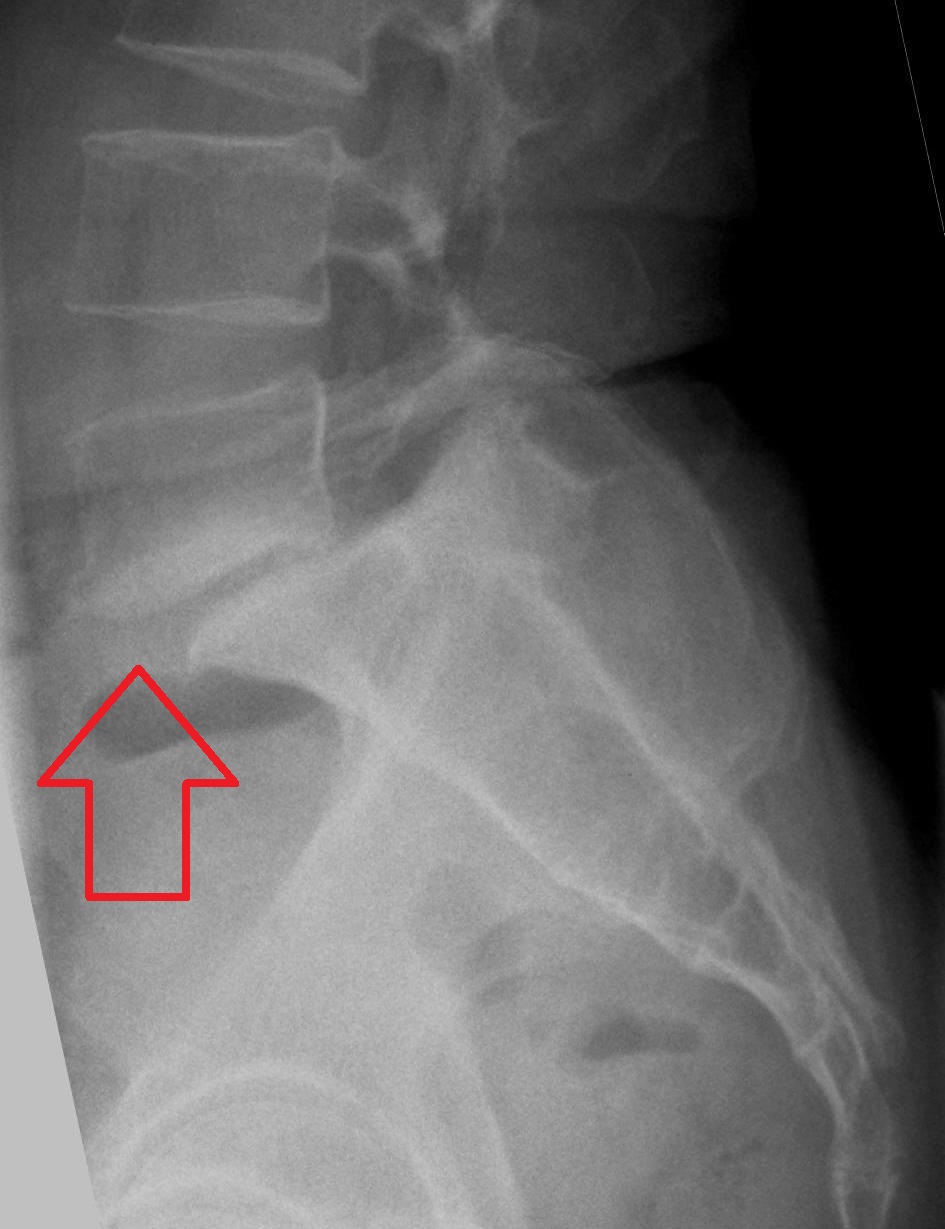
spondylolisthesis
forward movement vertebra on another, most common at L5-S1, due to spondylosis of pars or severe osteoarthritis

spondylolysis (lumbar)
separation of pars interarticularis (neck), most common at L4-5
arthrodesis
surgical immobilization by fusion to adjacent vertebra
laminotomy
done to decompress the spinal cord or nerves by removing a portion of the lamina that is impinging on the cord or nerve
laminectomy
decompression surgery where the entire lamina is removed that is impinging on the spinal cord or nerves
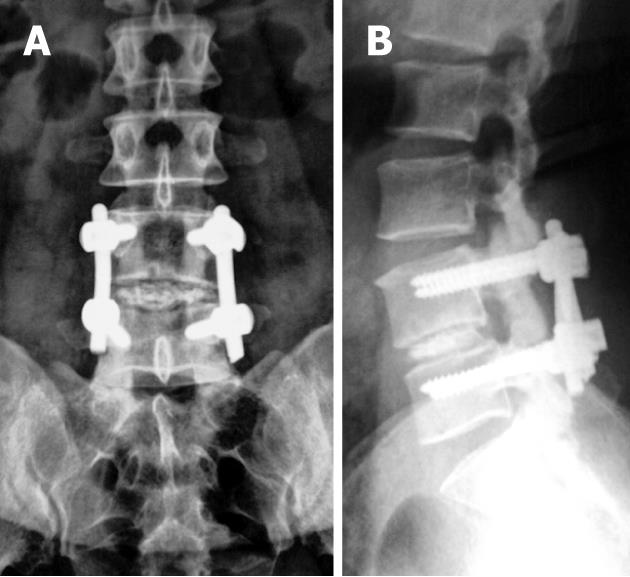
spinal fusion
using rods, plates, & screws to stabilize vertebra
microdiskectomy
microscopic surgery to remove protruding disk fragments by making a small hole in the annulus without removal of any bone from the vertebra
epidural steroid injection
ESI
median (nerve) branch block
MBB
radiofrequency ablation
RFA