lecture 6/7- sleep disorders 1 (narcolepsy + insomnia)
1/28
Earn XP
Description and Tags
narcolepsy, insomnia
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
what is narcolepsy? prevalence + age of onset (4)
irresistible =, recurring short episodes of sleep accompanied by cataplexy (elicited by strong emotion)
most prominent symptom: excessive daytime sleepiness
~1/2000 people
starts at age 15-25
symptoms of narcolepsy (4)
daytime sleepiness
cataplexy
sleep paralysis
hypnagogic hallucinations
how can narcolepsy be debilitating? how do patients feel after an attack? (3)
intrudes into wakefulness at any time → recurs throughout the day
each attack can last for minutes/hours
patient feels refreshed after attack and enters refractory period where attack is unlikely
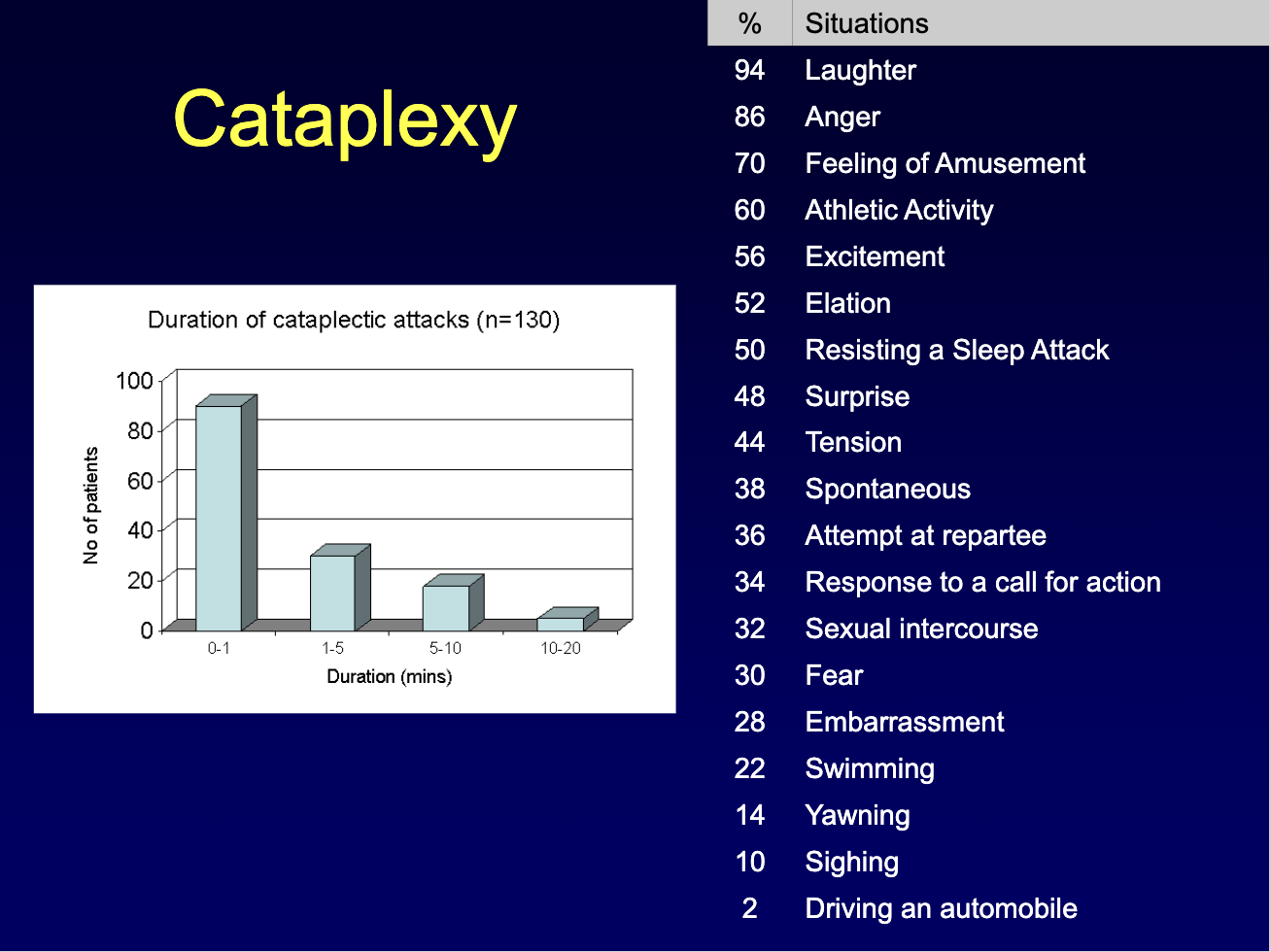
describe cataplexy, what is it, what causes it, effects? (3)
loss of muscle tone during wake resulting in total collapse, slight bucking of knees, or drooping of jaw
caused by intense emotion ie. laughter/anger
causes speech to slur, eyesight impaired
describe the sleep paralysis associated with narcolepsy onset vs offset paralysis (5)
typically occurs when falling asleep/waking up
total inability to move/speak
fully conscious + aware of paralysis
sleep onset → rare
sleep offset → more common occurs when waking from REM sleep
hypnagogic hallucinations associated with narcolepsy (3) how are they different from other hallucinations (2)
vivid perceptions → visual, auditory, tactile, kinetic
sensation of threat, suffocation, floating, spinning, falling
occur at transition from wake to sleep/REM to sleep
40-80% experience this
different from other hallucinations:
ppl know they are not real
only occur around sleep
cataplexy, sleep paralysis, hypnagogic hallucinations are all pathological manifestations of ___ and point to a problem in the ____ since the medulla + ____ actively suppress ___ during REM and ____ can be induced with injections of cholinergic/glutamatergic agonist into the ____, medulla, or ___
REM
brainstem
pons
muscle tone
cataplexy
brainstem
pons
REM latency & narcolepsy: what’s the hallmark finding on MSLT, and what does it imply? (3)
Narcolepsy hallmark: sleep-onset REM on MSLT (REM within ~2–3 min)
Normal tired people almost never enter REM on MSLT
Short REM latency can occur with high REM pressure (REM deprivation / stopping REM-suppressing drugs), but narcolepsy is mainly REM timing at sleep onset, not necessarily more or stronger REM
current treatments for narcolepsy (2) what are their shortcomings (2)?
excessive sleepiness treated with stimulants, naps, xyrem (GHB)
cataplexy treated with REM suppressing drugs like antidepressants
problems: tolerance to stimulants
treatments focused on symptoms not cause
potential causes for narcolepsy (3)
hereditary component → only 30% concordance in monozygotic twins → susceptibility
associated with antigens for a major histocompatibility complex on chromosome 6 also seen on MS/rheumatoid arthritis
may be an autoimmune disease
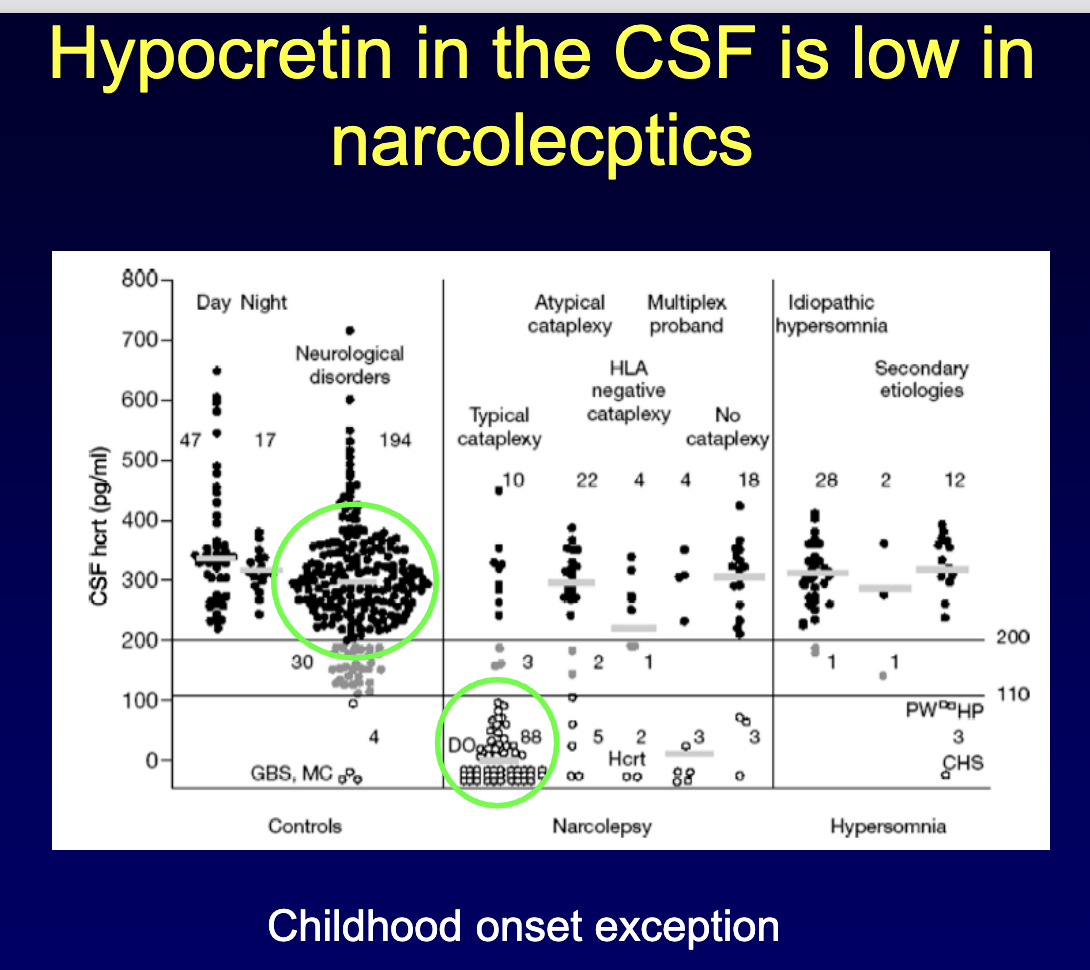
narcolepsy is caused from the loss of cells containing ____ in the ____
hypocretin (orexin)
hypothalamus
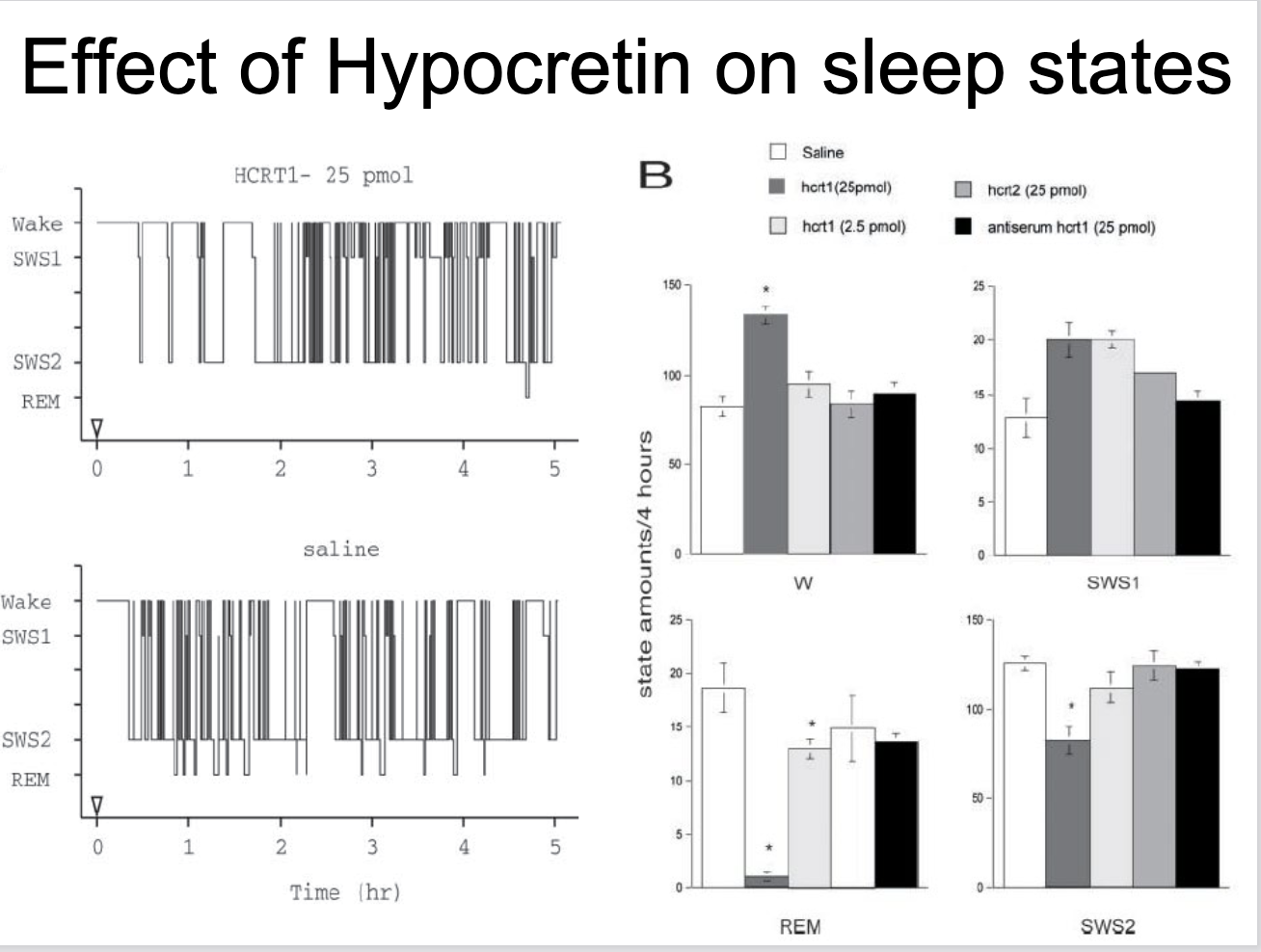
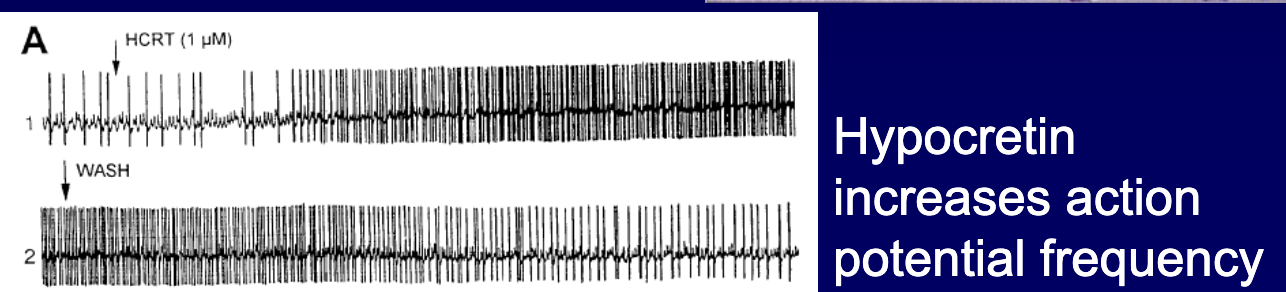
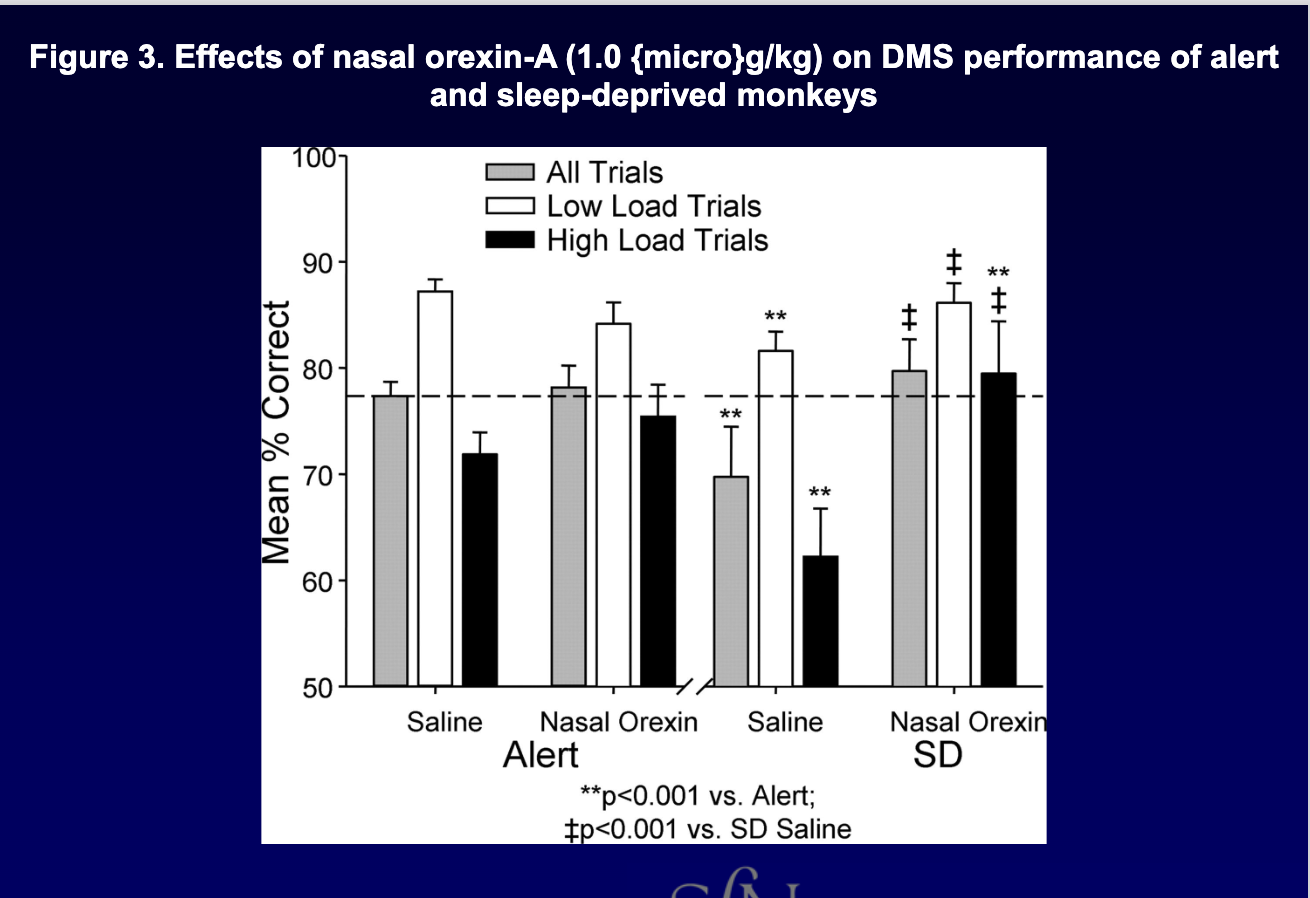
which arousal systems does orexin activate + what is the evidence
excites/stabilizes wakefulness by activating arousal systems (TMN/LC/raphe)
evidence: applying hyprocretin increases action potential firing rate in these neurons
what might future treatments for narcolepsy try to do?
develop drugs that activate HCRT2 receptor to promote arousal
In hypocretin-knockout mice, what did viral hypocretin gene therapy do, and what were the limitations? (2)
Viral delivery (herpes) of hypocretin gene → normalizes CSF hypocretin, reduces cataplexy, normalizes nighttime REM
Limitations: KO isn’t the typical human cause; effect fades ~after 1 week
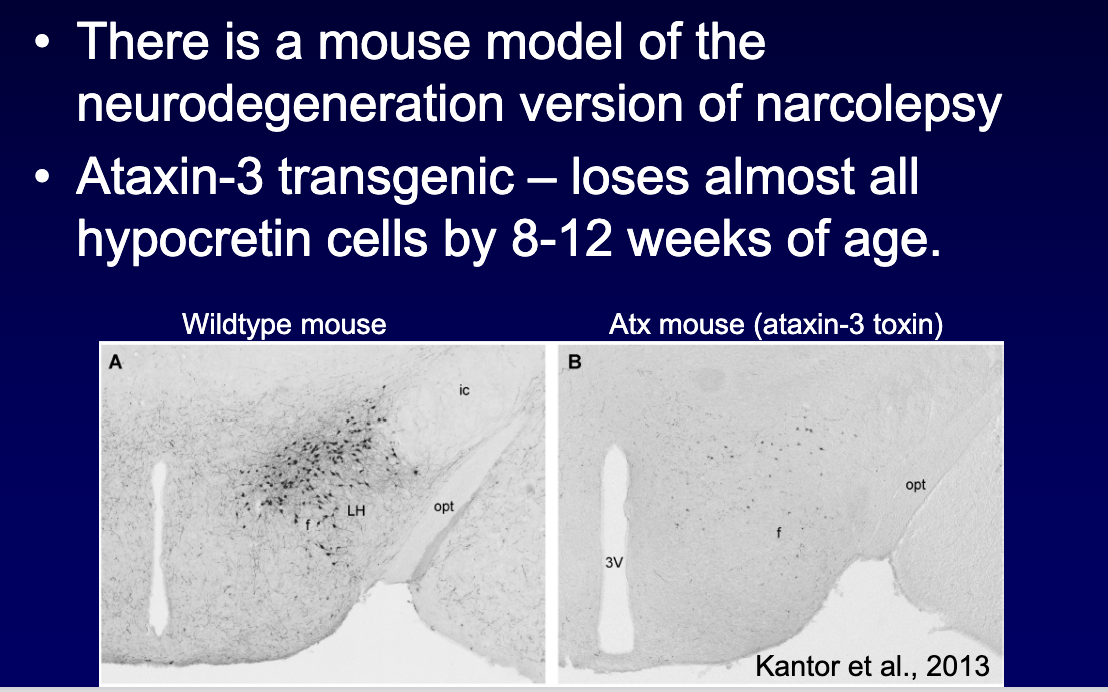
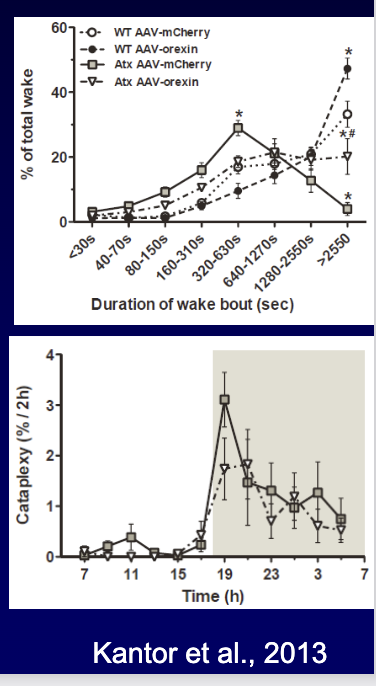
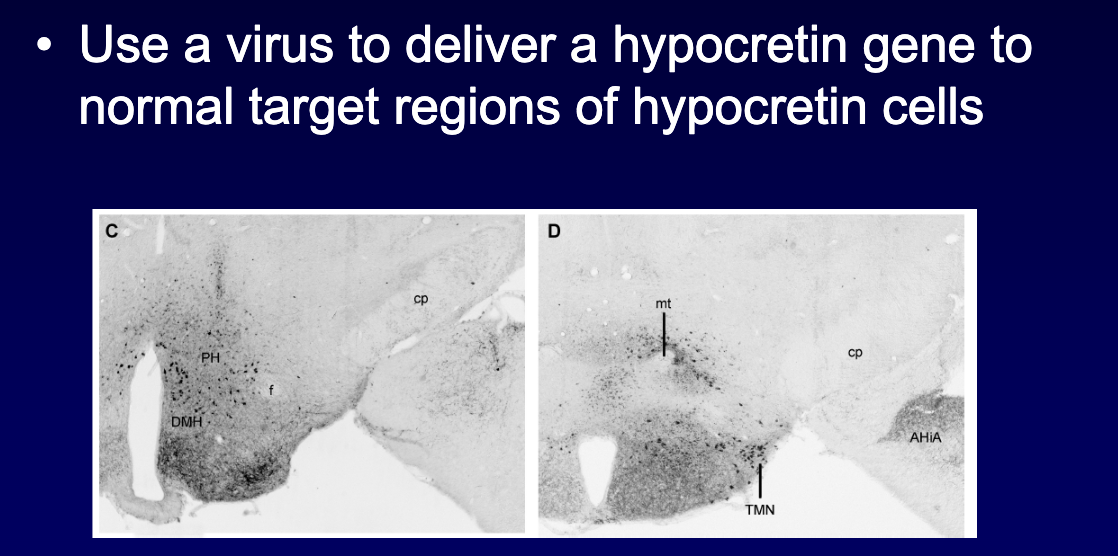
In the ataxin-3 (hypocretin-cell loss) narcolepsy model, what did hypocretin gene therapy improve? (3)
Virus delivered hypocretin to target regions → improved REM, NREM, and wakefulness
Normalized wake bout duration
Maybe small drop in cataplexy (depends on area treated)
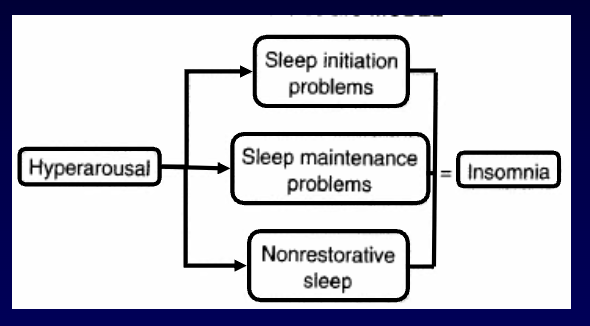
insomnia is characterized by ____ where sleep ___ and/or ___ become difficult with ___% of adults saying they have some symptoms while ___% say it is chronic.
hyperarousal
initiation and/or maintenance
30-40%
10-15%
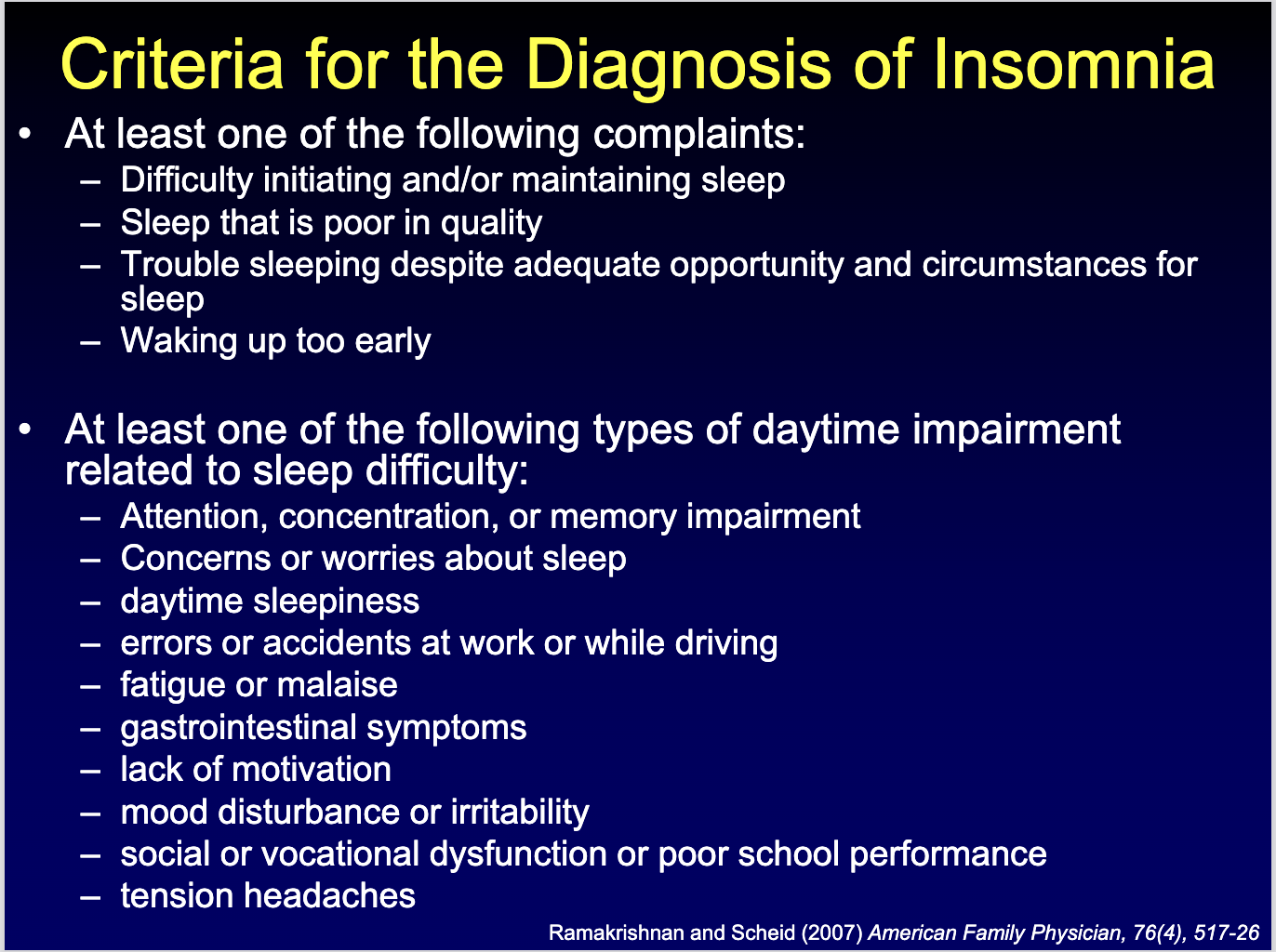
criteria for the diagnosis of insomnia (name a few)
causes for acute (3) vs chronic insomnia (2)
acute insomnia (<30 days)
situational stressors
environmental stressors
death/illness of a loved one
chronic insomnia (>30 days)
medical/psychiatric/sleep disorder
circadian disruption
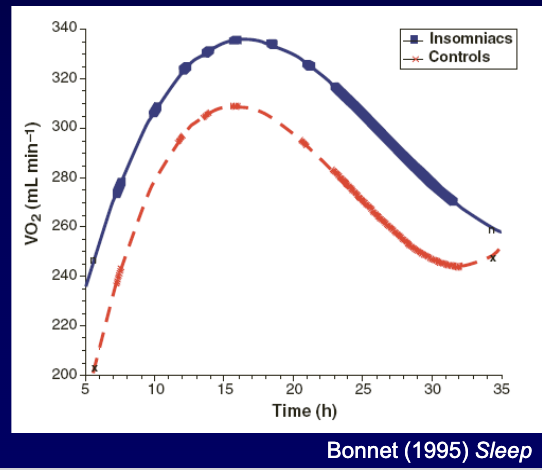
Physiological (hyperarousal) model of insomnia: core idea, evidence, and main weakness? (3)
Core idea: elevated physiological arousal during the normal sleep period is incompatible with sleep continuity (arousal vs sleep are mutually exclusive)
Evidence: poor sleepers show higher arousal measures (HR, respiration, temperature, muscle tone), especially at sleep onset (sometimes ↑ 24h metabolic rate)
Weakness: doesn’t explain how insomnia develops or why it persists/promotes sleeplessness
Cognitive model of insomnia: what are the 3 P’s and what does each mean? (3)
Predispose: worry-prone / stress-reactive → easier to become hyperaroused
Precipitate: stress triggers worry/problem-solving → arousal → insomnia starts
Perpetuate: insomnia becomes focus of worry/rumination → keeps insomnia going
Cognitive model: two “other features” that maintain insomnia?
Selective attention to sleep-related threats (keeps arousal high)
Distorted perception of deficits: focus on daytime problems, over-detect deficits, blame sleep loss (even if not the cause)
Behavioural models of insomnia: what’s the key idea of sleep hygiene, and what’s the stimulus control model? (2)
Sleep hygiene: good advice, but poor hygiene isn’t necessary or sufficient → hygiene alone usually won’t cure insomnia
Stimulus control: insomnia is maintained by conditioning (bedroom paired with wake activities) → weaken bed=sleep link
Stimulus control: 2 key rules + what does CBT evidence suggest about insomnia?
Rules: use bed/bedroom for sleep (and intimacy) only; if you can’t sleep, get up and leave the bedroom
CBT improves symptoms (~50% acutely) and patients may keep improving → suggests insomnia isn’t purely behavioural (cognitive/arousal factors matter too)
Neurocognitive model: what causes acute vs chronic insomnia, and what’s the key “worry” point? (3)
Acute insomnia: cognitive + behavioural factors
Chronic insomnia: behavioural factors + classical conditioning of arousal
Worry/rumination extends wake but isn’t the root cause: “worry because awake,” not “awake because worry.”
Neurocognitive model: 3 arousal dimensions + key EEG marker; plus 2 other modulators of insomnia.
Arousal dimensions: somatic, cognitive, cortical
Cortical arousal marker: high-frequency EEG (14–45 Hz) during sleep onset/NREM
Other modulators:
Homeostasis impaired (less delta power / lower % SWS after deprivation)
Circadian phase shifts (sleep-onset insomnia = delayed clock; early awakening = advanced clock)
non-pharmacological treatments for insomnia include (6)
CBT
exercise
relaxation therapy
sleep restriction (paradoxical intention therapy)
stimulus control therapy
temporal control measures
pharmacotherapy for insomnia (6)
hypnotics may be the best choice for immediate relief → treat serious symptoms but don’t address root cause
benzos
sedating anti-depressants
non-benzos benzodiazepines receptor agonist
antihistamines
antipsychotics
general advice for insomnia (7)
follow bedtime routine
keep bedroom quiet, dark, at comfortable temp
exercise regularly
drink less caffeine
avoid alcohol/smoking
eat regular meals
bedroom only for sleep/intimacy
insomnia is usually comorbid with other disorders like (6)
pain
substance use/abuse
breathing disorders
cardiovascular disorder
endocrine
mental health