Shock and Sepsis: Pathophysiology, Types, and Management Strategies
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
What is shock?
A condition in which tissue perfusion is inadequate to deliver oxygen and nutrients to support vital organs and cellular function.
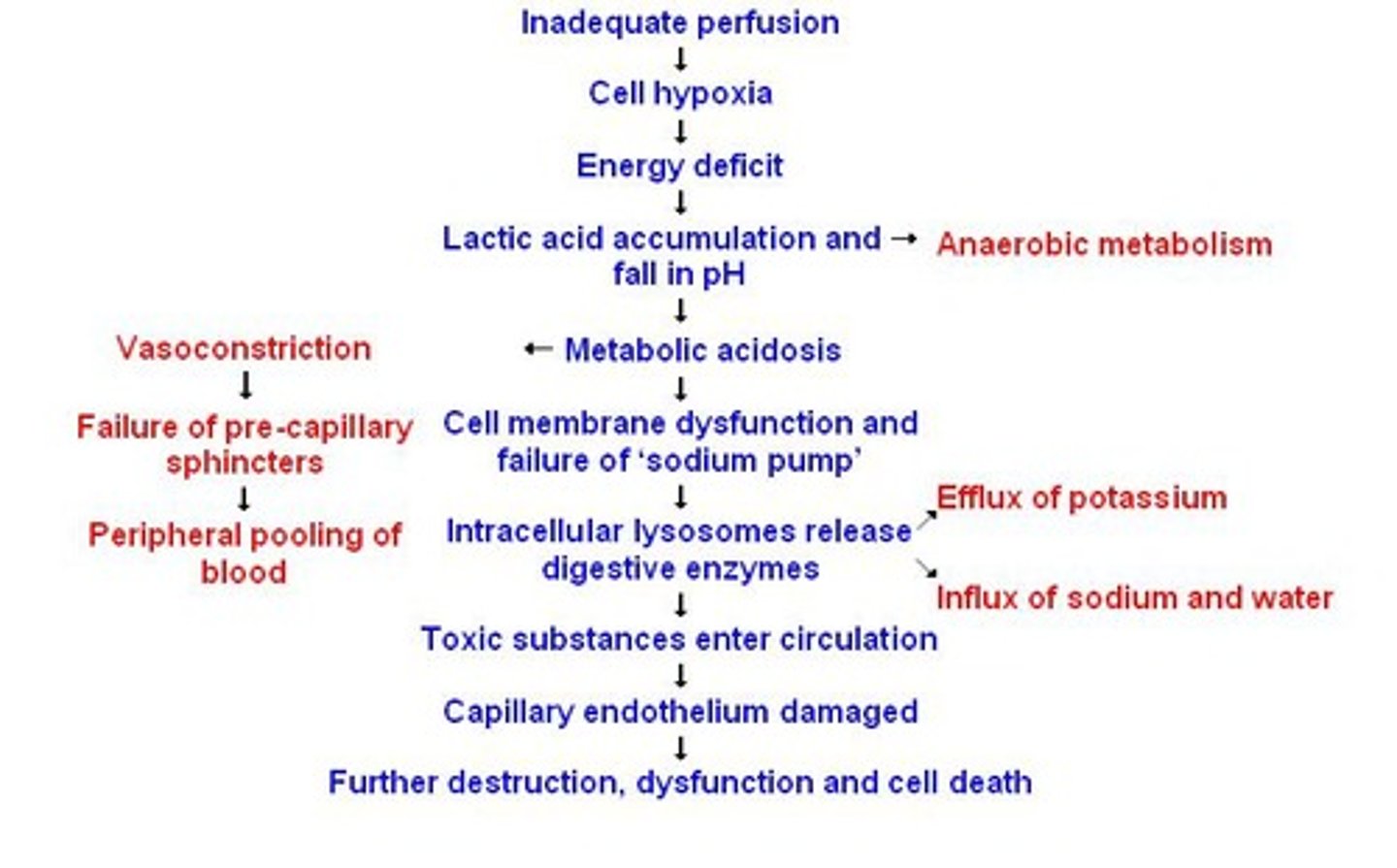
What are the consequences of inadequate tissue perfusion?
It results in severe metabolic acidosis and cellular death, affecting all body systems.
What are the four types of shock?
Cardiogenic, hypovolemic, distributive, and obstructive.
What characterizes cardiogenic shock?
Pump failure or myocardial impairment.
What characterizes hypovolemic shock?
Decreased intravascular volume, typically 10-15% or more due to hemorrhage or severe dehydration.
What characterizes distributive shock?
Widespread vasodilation and increased capillary permeability, seen in spinal, anaphylactic, and septic shock.
What characterizes obstructive shock?
Mechanical blockage of the heart chambers and great vessels, such as a massive pulmonary embolus.
What is the normal range for mean arterial pressure (MAP)?
70-110 mm Hg.
What happens when MAP falls below 65 mm Hg?
Tissue perfusion becomes compromised, leading to anaerobic metabolism and production of lactic acid.
What are the stages of shock?
Initial, compensatory, progressive, and irreversible.
What occurs during the compensatory stage of shock?
Increased heart rate, vasoconstriction, and attempts to restore tissue perfusion and oxygenation.
What are the clinical findings in the progressive stage of shock?
Decreased blood pressure and MAP, hypoperfusion of all organs, and mental status deterioration.
What defines the irreversible stage of shock?
Severe organ damage, unresponsive to treatment, and likely inability to survive.
What are common physical assessment cues in shock?
Increased heart rate, cool clammy skin, decreased urine output, and altered mental status.
What is hypovolemic shock?
A condition caused by too little circulating intravascular fluid volume.
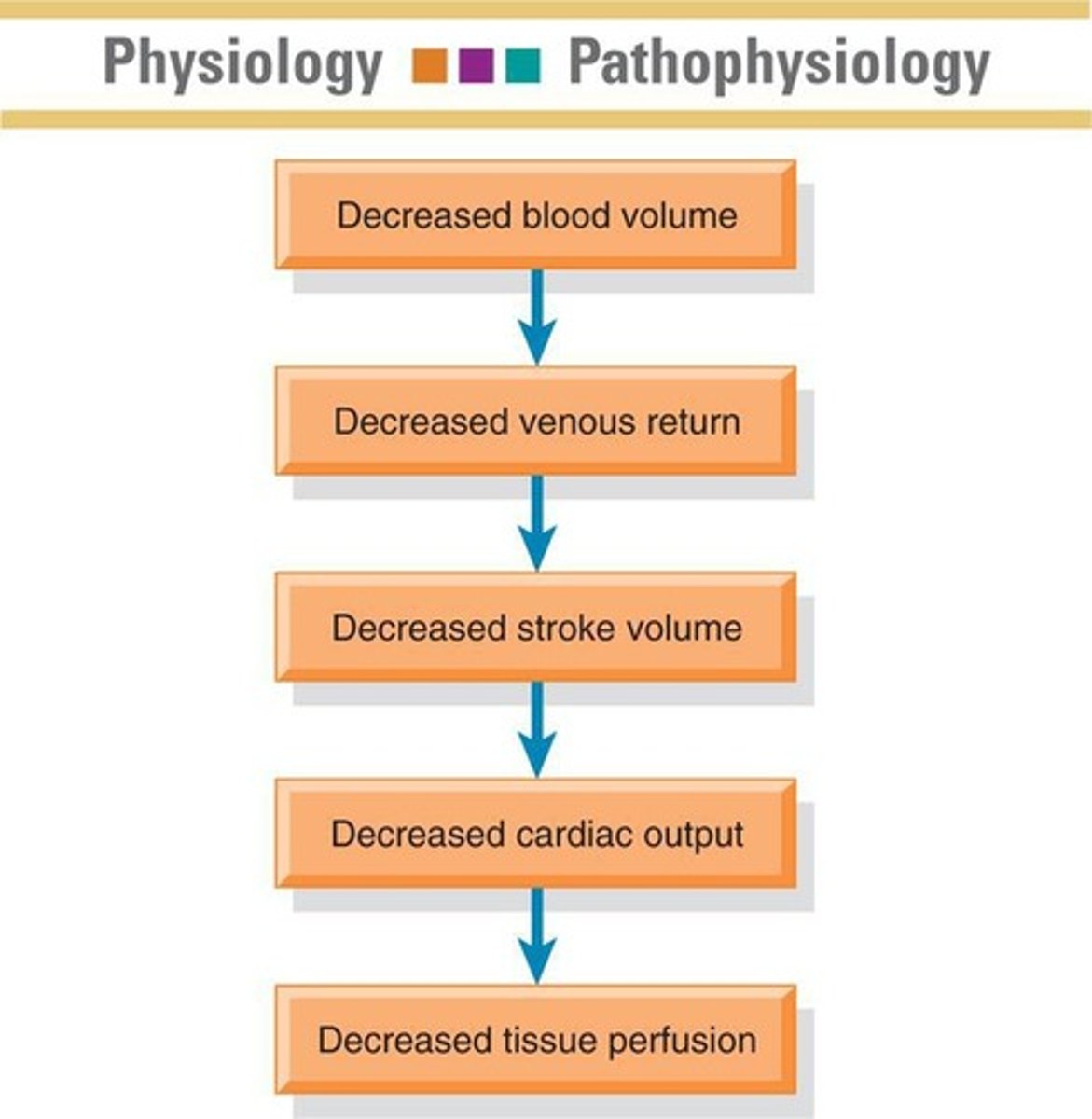
What are the hemodynamic changes in hypovolemic shock?
Decreased cardiac output, decreased central venous pressure, and increased systemic vascular resistance.
What is the Modified Trendelenburg position used for?
To increase venous return until fluid resuscitation can be initiated.
What types of fluids are commonly used in shock management?
Crystalloids and colloids.
What is Lactated Ringer's solution used for?
It is an isotonic solution that acts as a volume expander and buffers acidosis.
What is the primary use of packed red blood cells (PRBCs)?
To restore blood volume when hemoglobin is less than 7.0 g/dL.
What is the goal of management in shock states?
To improve tissue perfusion and maintain aerobic metabolism of cells.
What are the signs of metabolic acidosis in shock?
Increased respiratory rate and potential confusion due to decreased oxygen delivery.
What is the role of vasoactive medication therapy in shock?
To support blood pressure and improve cardiac output.
What are the nursing management strategies for hypovolemic shock?
Administering blood and fluids safely and implementing other supportive measures.
What is the significance of early identification and treatment in shock?
It is crucial for improving outcomes and preventing progression to irreversible shock.
How does the body compensate during the compensatory stage of shock?
By shunting blood from the skin, kidneys, and GI tract, leading to cool skin and decreased urine output.
What are the potential complications of fluid administration in shock?
Fluid overload, electrolyte imbalances, and potential for pulmonary edema.
What can multiple blood transfusions result in?
Coagulopathies (bleeding disorders)
When should vasopressor drugs be used?
Only after fluid replacement has been achieved and the patient's MAP remains < 65 mmHg.
What is the first intervention before starting vasopressor therapy?
Fluid replacement.
What is sepsis?
Life-threatening organ dysfunction caused by dysregulated host response to infection.
What defines septic shock?
A subset of sepsis with circulatory and cellular/metabolic dysfunction associated with higher risk of mortality.
What does SIRS stand for?
Systemic Inflammatory Response Syndrome.
What triggers SIRS?
Uncontrolled inflammation in response to trauma, infection, burns, pancreatitis, or shock.
What are the indicators of SIRS?
More than 2 of the following: hyperthermia, leukopenia, tachypnea, hypothermia, altered mental status, leukocytosis, tachycardia, immature bands-left shift, hyperglycemia.
What is Disseminated Intravascular Coagulation (DIC)?
A complication of activated SIRS resulting in rapid depletion of platelets and fibrinogen.
What are assessment cues for DIC?
Diffuse petechiae, ecchymosis, bleeding from membranes, prolonged coagulation studies.
What is Multiple Organ Dysfunction Syndrome (MODS)?
Altered function of two or more organs in an acutely ill patient where homeostasis cannot be maintained without intervention.
What is the Modified Early Warning Score (MEWS)?
A scoring system for assessing patient status based on vital signs.
What does the SOFA tool assess?
Mortality prediction based on the dysfunction of six organ systems.
What lab cultures should be obtained in suspected sepsis?
Blood (aerobic and anaerobic), urine, sputum, wound cultures.
What does a lactate level > 2 mmol/L indicate?
Decreased tissue perfusion.
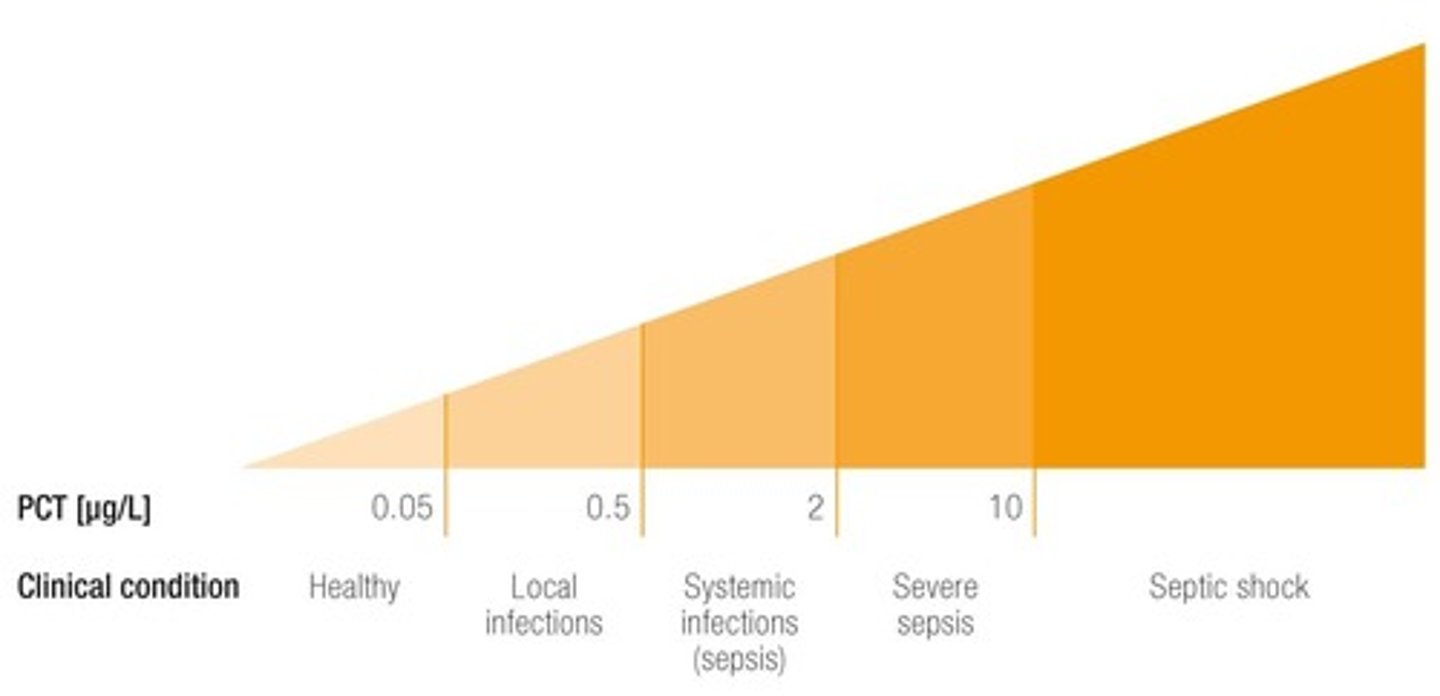
What is Procalcitonin (PCT)?
A prohormone indicating bacterial invasion and differentiating sepsis from non-infectious systemic inflammatory reactions.
What does C-reactive protein (CRP) measure?
The presence of acute inflammation.
What hemodynamic changes occur in the warm phase of septic shock?
Increased cardiac output, decreased CVP/RAP, decreased PAP, decreased PCWP, decreased SVR, increased heart rate.
What hemodynamic changes occur in the cold phase of septic shock?
Decreased cardiac output, increased CVP/RAP, increased PAP, increased PCWP, increased SVR, increased heart rate.
What is the purpose of the Sepsis Bundle?
To implement a group of interventions that improve outcomes for sepsis when executed together.
What is the initial fluid resuscitation goal for sepsis?
30 ml/kg of intravenous crystalloid fluid within the first 3 hours.
What is the preferred vasopressor for septic shock?
Norepinephrine (Levophed).
When should corticosteroids be administered in sepsis?
Only if fluids and vasopressors fail to restore hemodynamic stability.
What is the target blood glucose level for patients with sepsis?
140-180 mg/dL.
What is recommended for stress ulcer prophylaxis in sepsis?
Use of H2 receptor blockers or proton pump inhibitors.
What is the recommendation for deep vein thrombosis prophylaxis in severe sepsis?
Daily subcutaneous low-molecular weight heparin (LMWH) and compression devices.
How does aging affect shock response in older adults?
Older adults have a decreased ability to compensate for shock states due to physiological changes.