BPK 310 - Lecture 8
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
Transient negative effects of acute exercise
Fatigue
Accumulation of metabolic wastes
Dehydration, fluid balance disruptions
Electrolyte disturbances
Muscle damage and delyaed onset muscle soreness
Oxidative stress
Inflammation
Fatigue, Description, Risk, Mitigation Strategy
Decrease in force or power production in response to contractile activitiy, can lead to task failure, the inability to sustain a force or pwoer adequate to accomplish a physical task. can be peripheral or central
risk of peripheral: certain - more important for high-intensity exercise, this is at muscle
risk of central: high - more important for prolonged moderate - or heavy - intensity exercise, at the brain
Apply progressive overload, consume CHO during exercise, pacing
Accumulation of metabolic wastes, Description, Risk, Mitigation Strategy
Amino acid ocidation and purine deamination producce nitrogenous wastes that can cause central fatigue and are highly neurotoxic (eg. NH4+, urea)
Certain, expecially in prolonged exercise
No mitigation strategy, it just will happen
Dehydration, Description, Risk, Mitigation Strategy
Reduced plasma volume, skin blood flow, thermoregulation
Certain
Consume liquids during exercise, especially in the heat
Electrolyte disturbances, Description, Risk, Mitigation Strategy
K levels rise in blood and intersitium - can interfere with muscle contractions
typically important only for prolonge exercise
Proper hydration and nutrition
Muscle damage (DOMS), Oxidative stress, inflammation, Description, Risk, Mitigation Strategy
Will be described later
High with unaccustomed eccentric contractions (DOMS)
risk is unknown for oxidative stress
High with sevre prolonged and intense exercise (inflammation)
Apply progressive overload, avoid trying to block these responses with drugs
Fatigue can depend on
The muscle fibers recruited
Slow oxidative fibers (type I) are fatigue resistant and will not show a substantial force decrease unless there is no fuel
Fast glycolytic fibers show marked fatigue
How is fatigue caused
Can be caused by limitations in either energy demand, energy supply, or both
Failure to consume energy sufficiently fast for the task (eg. inhibition of demand processes by metabolites)
Failure to supply energy sufficiently fast to meet demand (eg. depletion of substrate)
Hard to find cause of fatigue, but many correlates
Likely fatigue mechanisms at different intensities (at moderate, heavy, severe, extreme)
Moderate: hyperthermia (in the heat), reduced central drive/motivation (central fatigue), muscle damage
Heavy: glyocgen depletion, hyperthemia
Severe: depletion of finite energy store, accumu.ation of fatiguing metabolites, ATP supply issue
Extreme: as for severe, but also contraction coupling failure
Boundaries of exercise domains
Moderate: Upper - LT
Heavy: Lower - LT, Upper - CP
Severe: Lower - CP, Upper - highest power that elicits VO2max before fatigue
Extreme: Lower - highest power that elicits VO2max before fatigue
Central vs peripheral fatigue
Central: progressive reduction in voluntary activation of muscle during exercise
Peripheral: disruption of force-producing ability due to factors at or distal to the neuromuscular junction
Fatigue can occur at all sites along the force production pathway (eg. from motor cortex, to neuromuscular junction, to sarcomere)
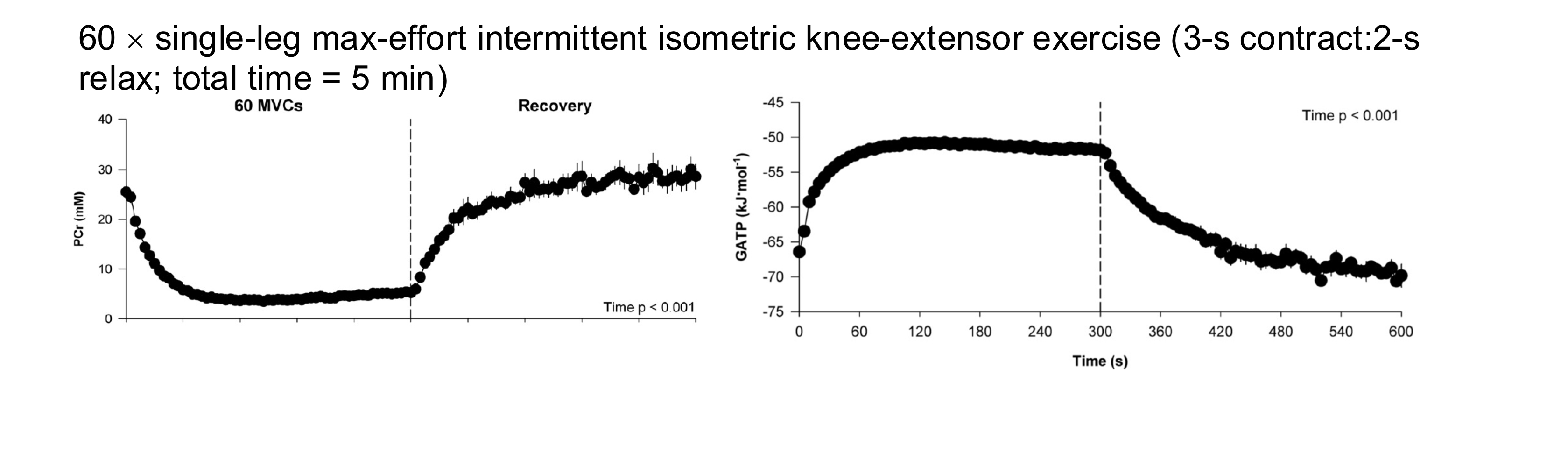
Mechanism of peripheral fatigue, substrate depletion of phosphagens
PCr drops as function of intensity, its depletion is a causal agent of fatigue, and happens very rapidly
ATPs overall concentration is well maintained except for exercise at highest intensities (eg. super max sprints as it drives down stores and ability to produce)
It is possible that ATP concentration varies locallyand that it is depleted at sites of use
Free energy of ATP hydrolysis decreases; i.e less energy availble to do work per hydrolyzed ATP due to a build up of products
Mechanism of peripheral fatigue, substrate depletion of glycogen
Glycogen depletion depends on duration and intensity
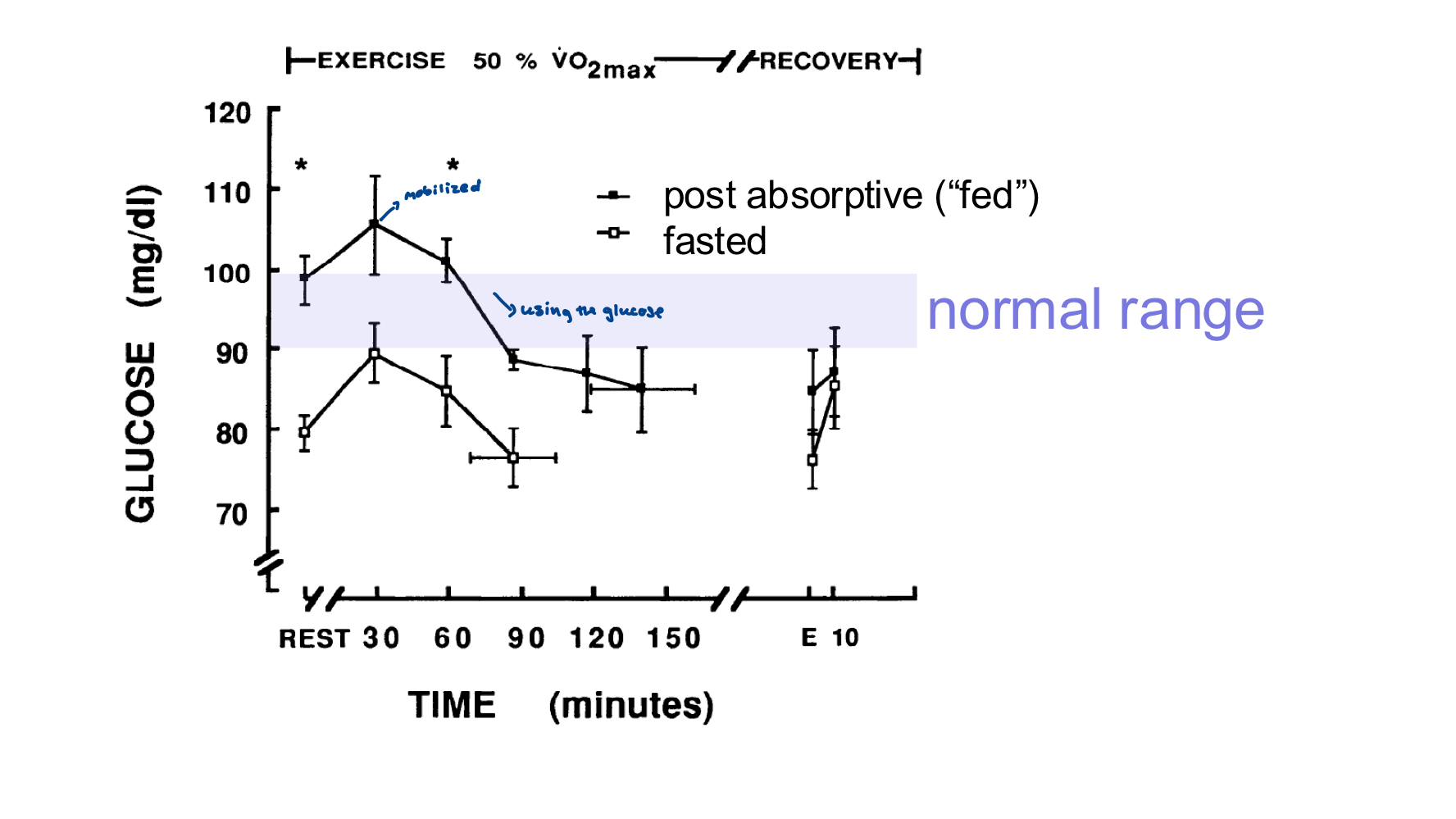
At 50%VO2max, theoretically the stores will not deplete, especially as you commonly consume CHO while doing it
At 75% VO2 max, the stores will deplete (for someone with VO2max = 60) at around 180 mins
At 95% VO2max, the stroes will deplete (for someone with VO2max = 60) at around 60 mins
At 100% VO2max, it would theoretically take 30 mins to deplte glycogen stores but it is not possible to go that long at that intensity due to other issues
**Duration until depletion also depends on persons regular consumption of CHO
Mechanism of peripheral fatigue, substrate depletion, impaired availbility of energy from carbs and lipids
Blood glucose has three sources, liver glucogen, dietary intake, gluconeogenesis from liver (from lactate)
Prolonged exercise near or above LT: liver glycogen depletes, rate of gluconeogensis decreased dut to reduced blood flow to lover → blood glucose levels decrease
Glucose available to brain decreases - exercise feels more difficult
Lipids, cataplerosis (loss of TCA intermediates) decreases fatty acid oxidation, inhibition of fat oxidation enzymes
Mechanism of peripheral fatigue, reduced O2 availability
Adequate O2 is essential to sustain muscular work
Factors decuing O2 transport: decreased blood volume = decreased cardiac output, and blood flow redistribution away from working muscle as the brain still requires a certain amount of blood
This is definitely an issue at high altitude, or during ischemic event, or when hypoxic
Mechanism of peripheral fatigue, metabolite accumulation
Inorganic phosphate, inhibits PFK, and interferes with Ca binding to troponin
H (decreased pH):
causes protons dissociate form several acidic moleucles such as the products of ATP hydrolysis and severeal glycolytic intermediates being weak acids
consequences: can interfer with Xbridge cycling, inhibits PFK and hormone-sensitive lipases, displaces Ca from troponin, displaces O2 from Hb (good for at muscles, not at lungs), low pH affects brain and causes pain, nausea, and disoreintation
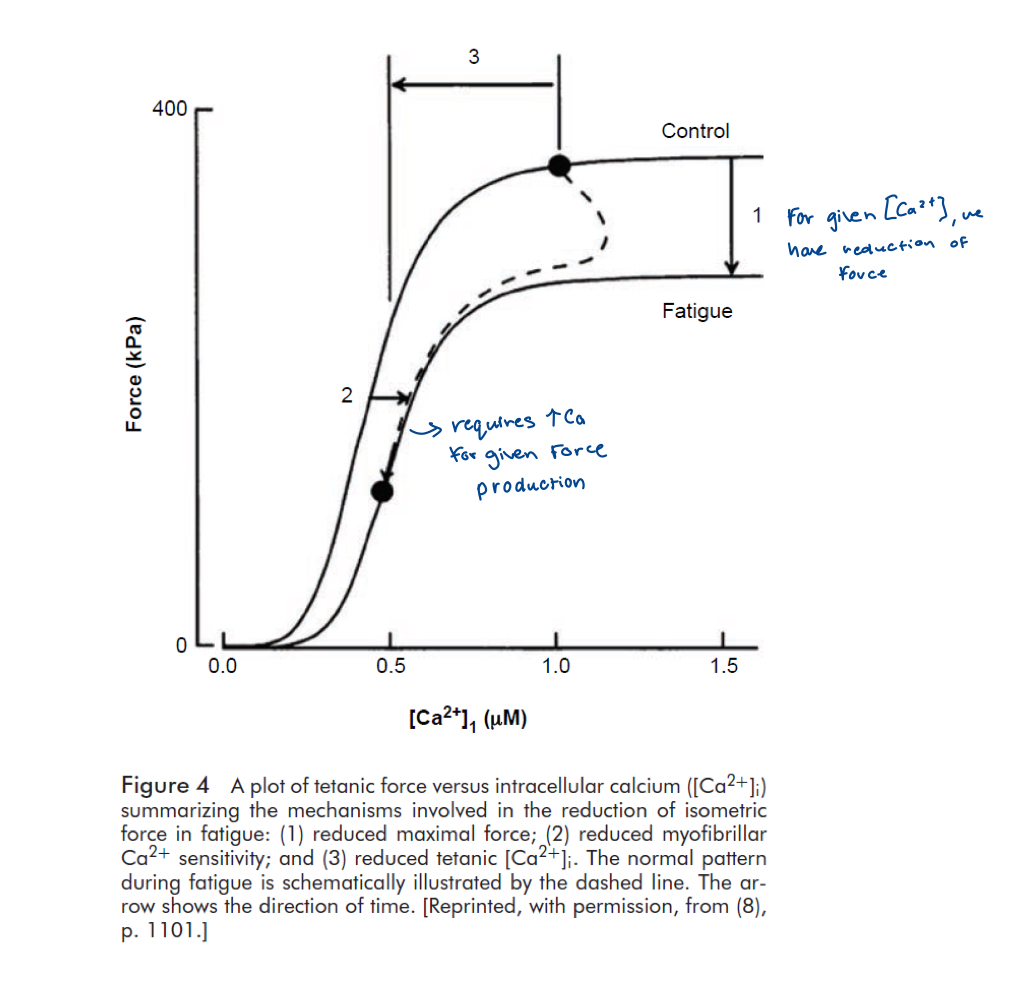
Mechanism of peripheral fatigue, impaired Ca handling
Interference with Ca effects
Sensitivity of contractile apparatus reduced (H, Pi)
Reduced Ca release from SR: loss from SR/slower relaxation due to reduced SR uptake (less recovery = less force production in next cycle)
The muscle metabolic environment is ______ at task failure at different durations of severe-intensity exercise
Would we see the same thing in the heavy-intensity domain?
Similar
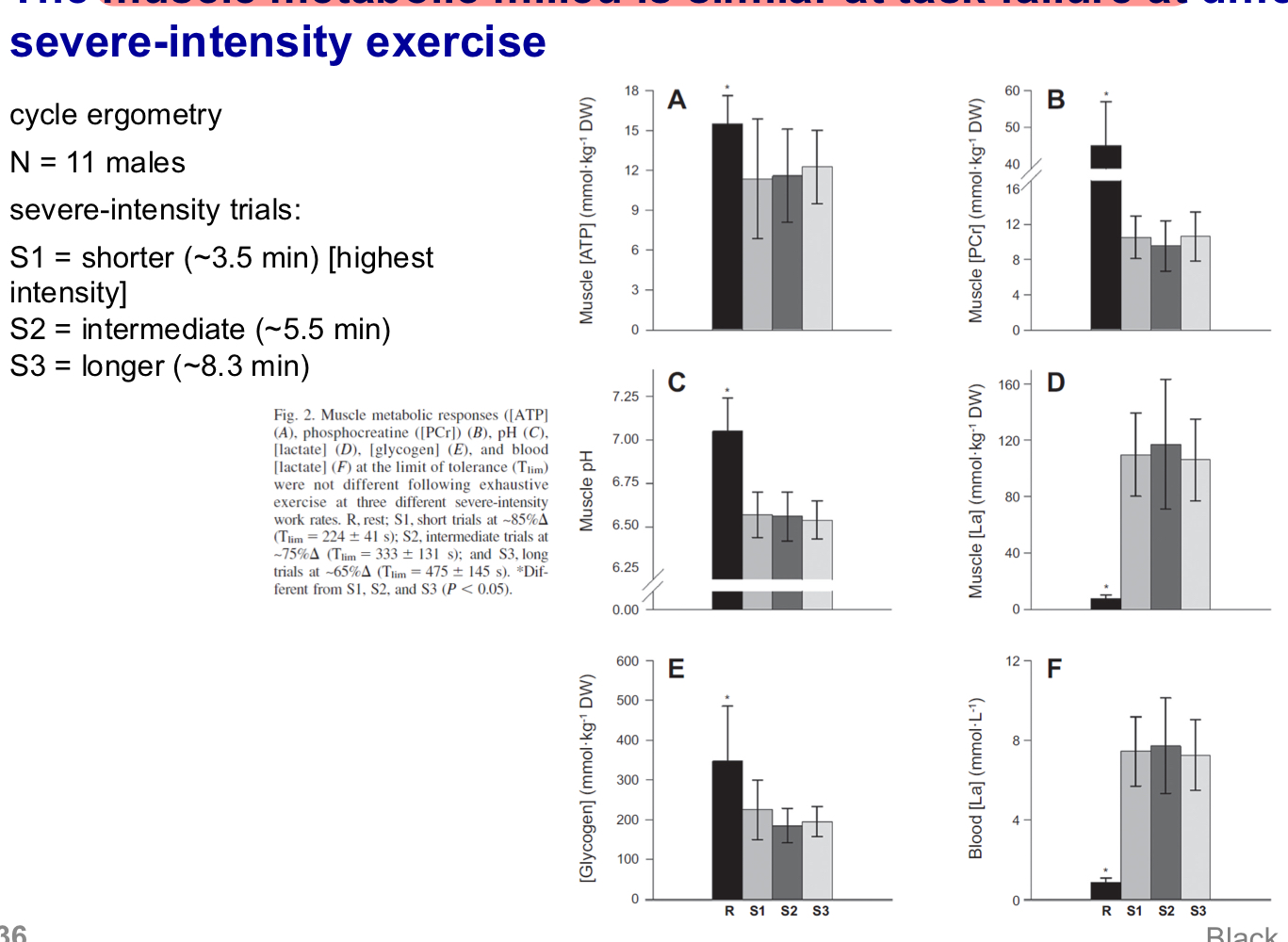
No we wouldn’t, as different mechanisms of fatigue
What is central fatigue and what is the mechanism
The decrease in torque/power secondary to a decrease in voluntary muscle activitiation
Feedback from muscle group III and IV afferents reduces central motor drive, they may exert inhibitroy feedback effects
What is psychological fatigue
Succumb to exertion-related discomforts
Pain, nausea, weakness, dyspnea, side stitch, cramp, hunger, sleepiness, etc.
Following exercise, we need recovery which consists of:
Rplenish substrates: phsophagens, glycogen, lipids
Dispose of emtabolites that impair force production
Restore fluid and electrolyte balance
Dissipate heat
Repair damage
Manage inflammation
Precise recovery kinetics will depend on many factors:
Degree of substrate consumption/metabolite accumulation (volume and intensity of exercise)
Recovery context: availability of substrates, environmental conditions
Fitness of individual
Timescale
Time allowed for or taken by a process for a sequence of events
Express in the different units of time: seconds, mins, hours, etc.
Phosphagen recovery
Requires O2 supply
With intact circulation 90% of PCr can recover in 4 minutes, and 100% at ~5 mins
Time course of glycogen replensihment during recovery
Can take 24hrs (~1-2 days) to recover
But depends on CHO availability, complete resynthesis requires a high dietary intake of carbs during at least a two-day period.
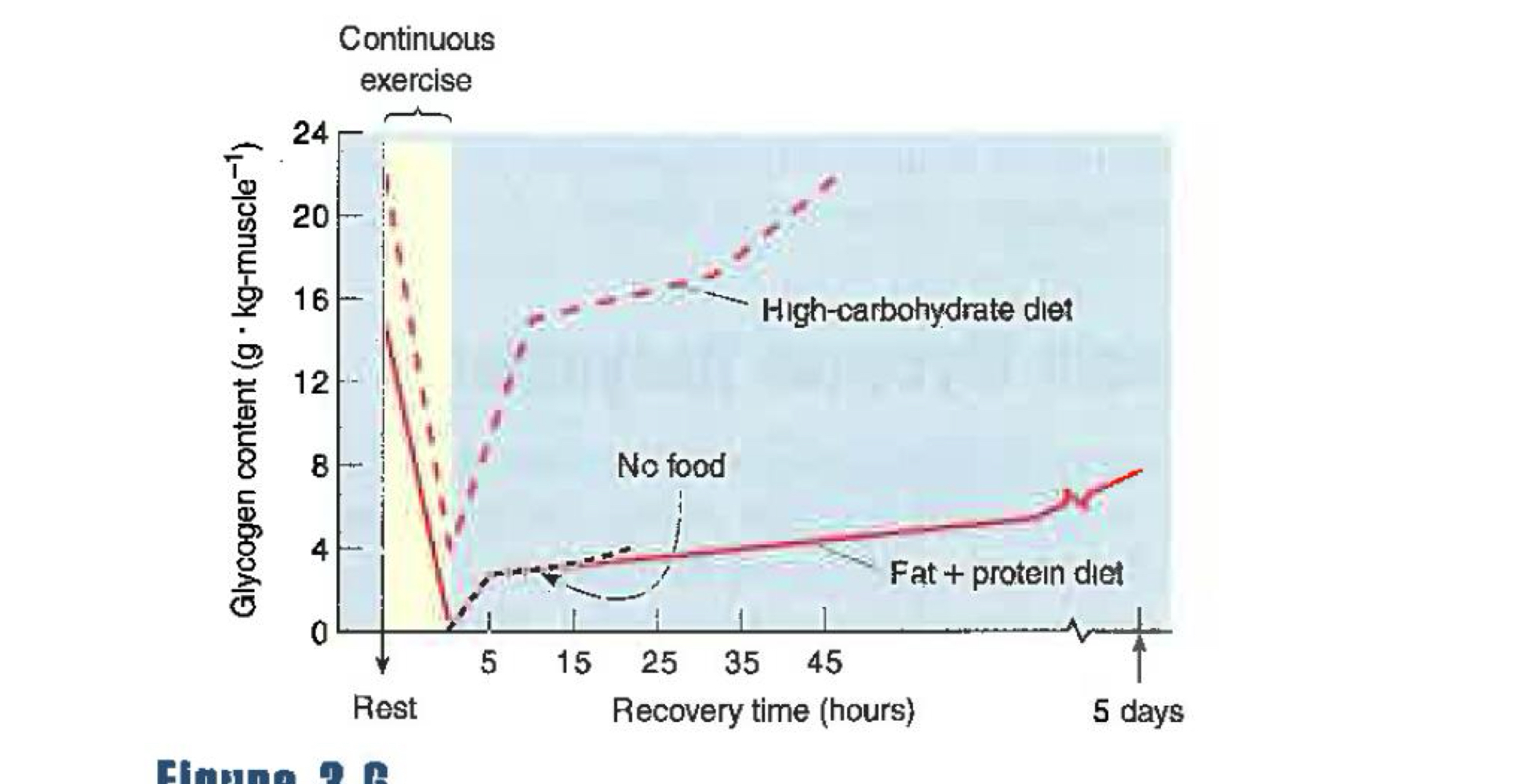
Glycogen will accumualte more rapidly after intense intermittent exercise, and following intermittent exercise a significant amount of glycogen is resynthesized during the first 2 hours of recovery even in absence of food intake. Still, complete resynthesis requires 24 hours
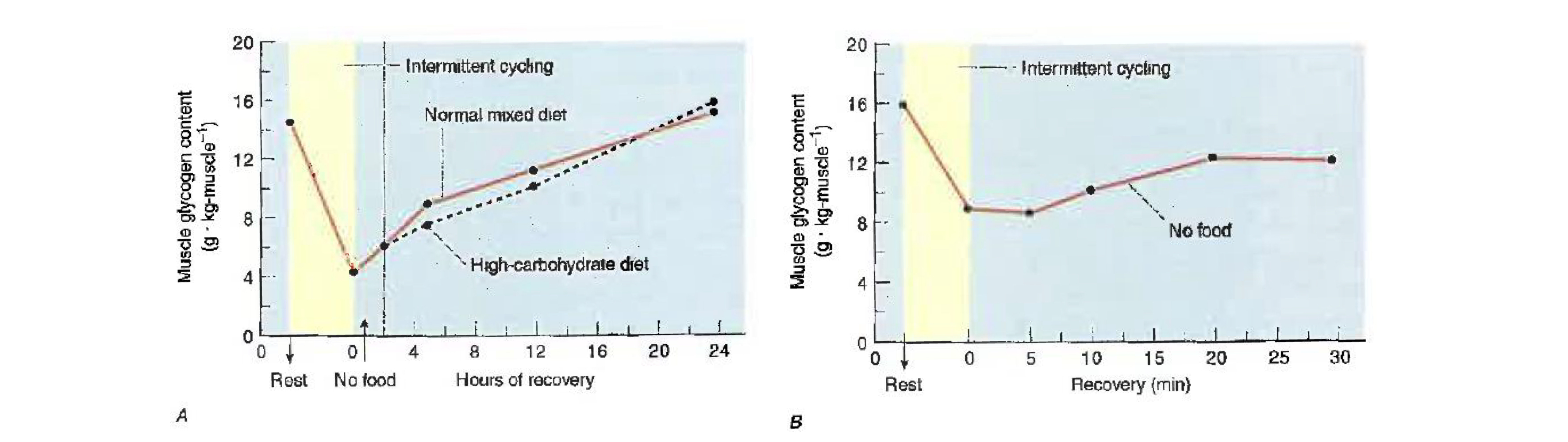
Why might differences exist between post-continuous and intermittent exercise in glycogen recovery
Amount deplete: continous > intermittent
Availability of precursors: higher with intermittent (higher glucose release during intense exercise)
Fibre type differences: type II fibers resynthesize glycogen faster than type I and they are recruited more during intense intermittent exercise
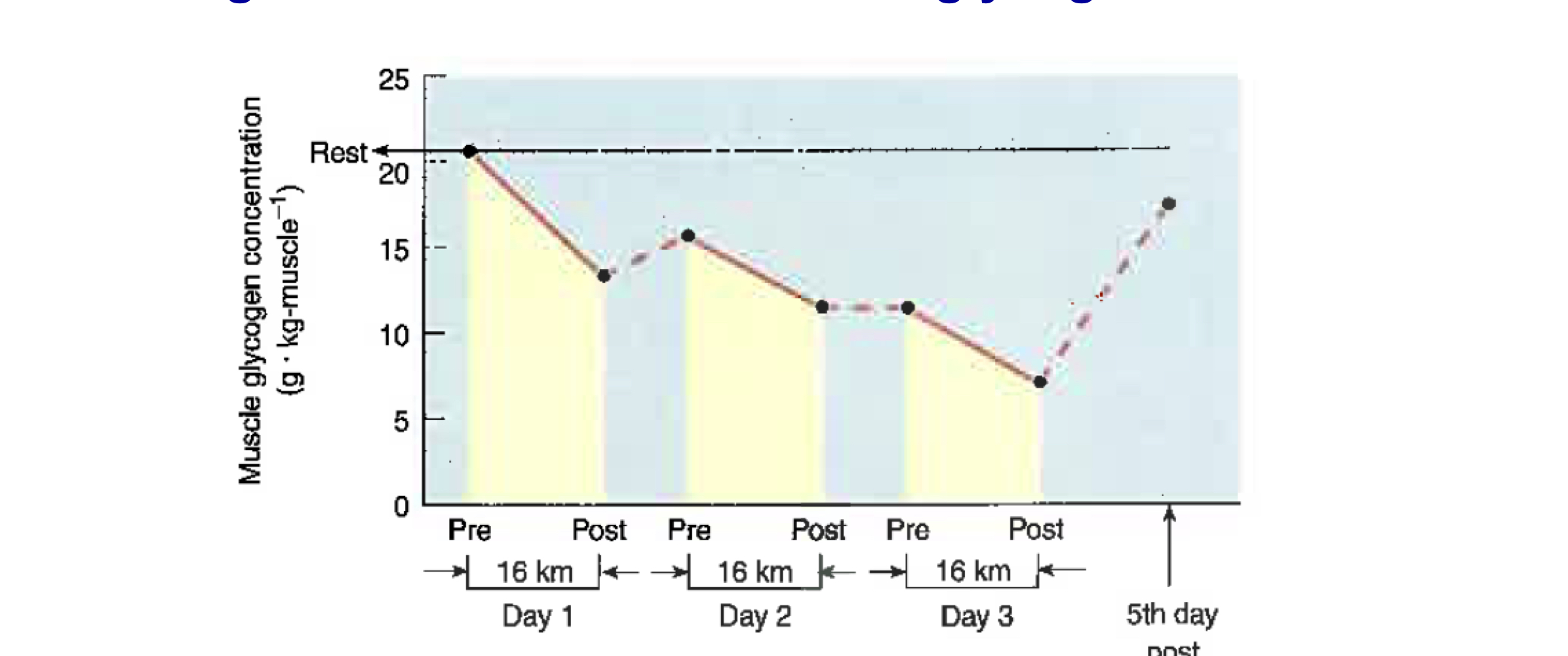
Since glycogen progressively depletes in response to successive exercise bouts, what what happens as a result of consecutive training bouts
It results in overall lowered glycogen
Eg. muscle glycogen is progressively depleted during a three-day pariod when 16km are run each day
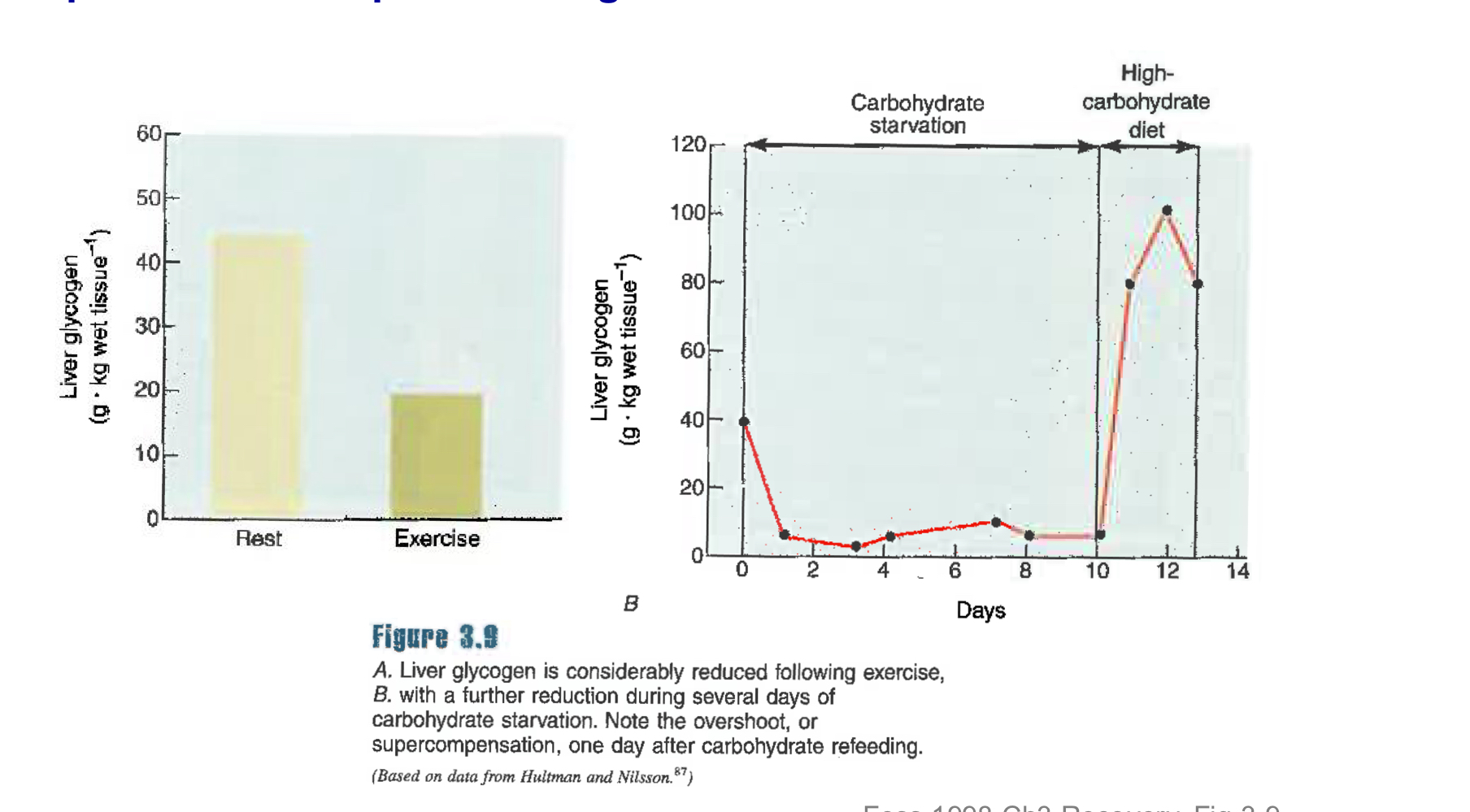
Liver glycogen depletes with?
Exercise and starvation and can “supercompensate” in response to high-CHO diet
Maximizing post-exercise glycogen resynthesis
Type and amount: carbohydrate (1-1.5 g/kg/hr) should be consumed, ingestion of carb:protein mixture may enhance glycogen resynthesis but only if less-tahn-optimal CHO is consumed (<0.8/g/kg/hr)
Timing:
Biphasic - initial rapid resynthesis 30-60 min post-exercise if exogenous CHO is available (possible due to insulin-independent GLUT4 translocation).
Slow resynthesis (80% slower) via insulin-mediated pathways
Glycogen resynthesis rates highest when feeding occurs immediately after exercise. Nevertheless, glycogen levels will recover no matter the time of feeding, just more slowly
If rapid recovery is sought = feed as soon as possible after exercise
Lactate recovery kinetics and fates
Lactate is important for replensighing glycogen and for supplying other energy processes
Timescale = minutes to hours
Lactate is removed from blood and muscles during recovery from exhausting exercise, in general 25 mins of rest-recovery are required to remove half of accumulated lactate
It will be metabolically converted to glucose, protein, glycogen, CO2, and H2O (oxidized).
Oxidation occurs primarily in type I skeletal muscle fibers
Lactate recovery kinetics: passive vs. active
Active recovery (i.e light exercise during recovery) causes faster lactate removal, primarily due to increased oxidation by working type I muscle fibers.
For untrained subjects recovery exercise that produces fastest/optimal rate of lactate removal in one in which VO2 is between 30-45% max
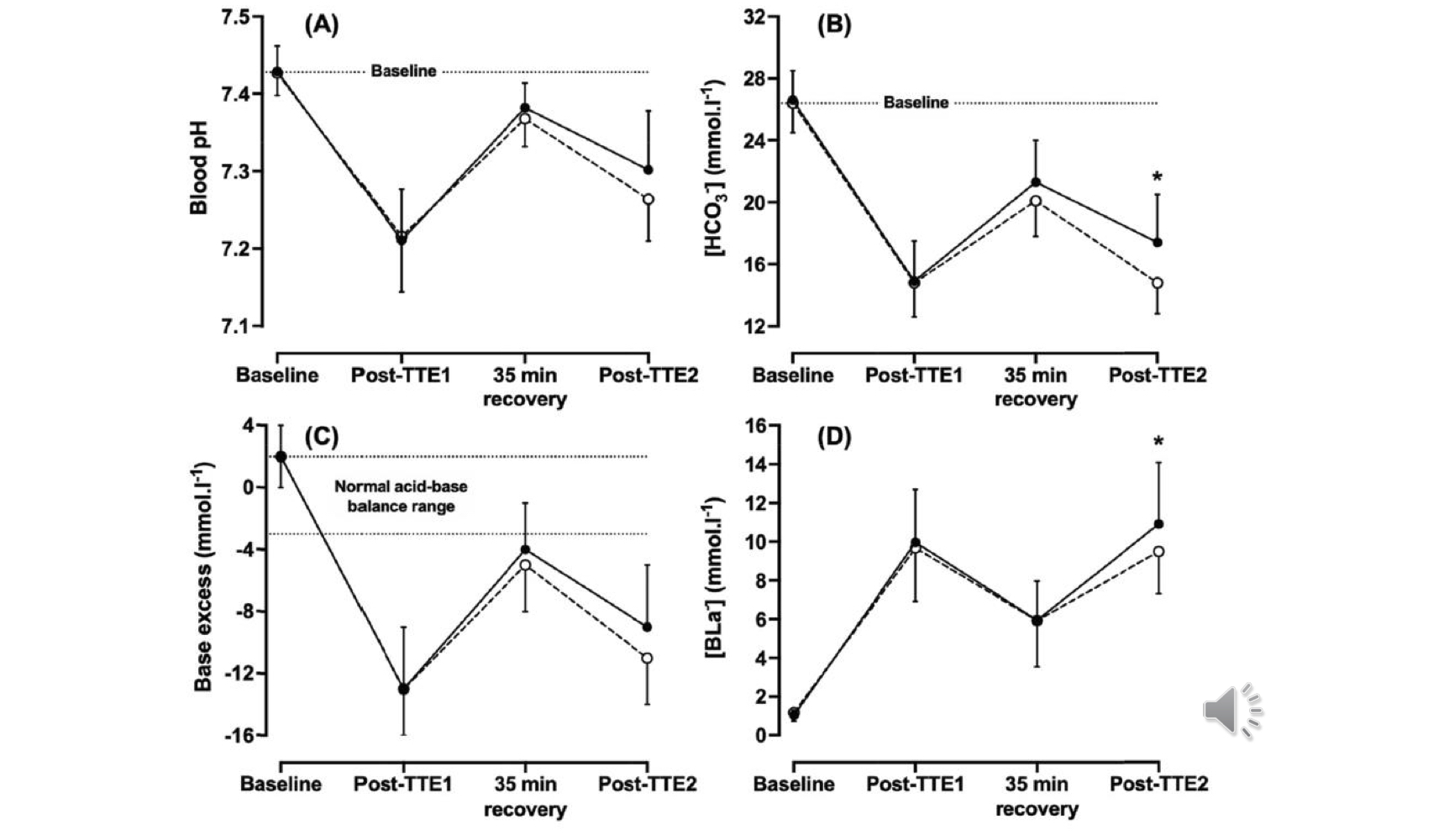
Blood pH, bicarbonate, lactate levels following time-to-exhaustion tests with 35 min recovery between
blood pH: recovers almost to baseline within 35 min recovery
HCO3: recovers about ½ within 35 min recovery
blood lactate: is still heightened within 35 min recovery
Recovery of lipids, amino acids, and electrolytes
Depends on type (eg. continous, intermittent), intensity and duration of exercise
Lipids
arterial FFA increase post-exercise due to blood flow redistribution
blood FFA and glycerol levels are elevated for hours )12+) post-exercise (energy source for recovery)
Amino acids
liver gluconeogenese enhanced post-exercise
Electrolytes
muscle and arterial; recoveries typically follow first-order kinetics
pH - minutes to hours
K - recovers in minutes (5-30)
Pi - recovery in minutes (5-10)
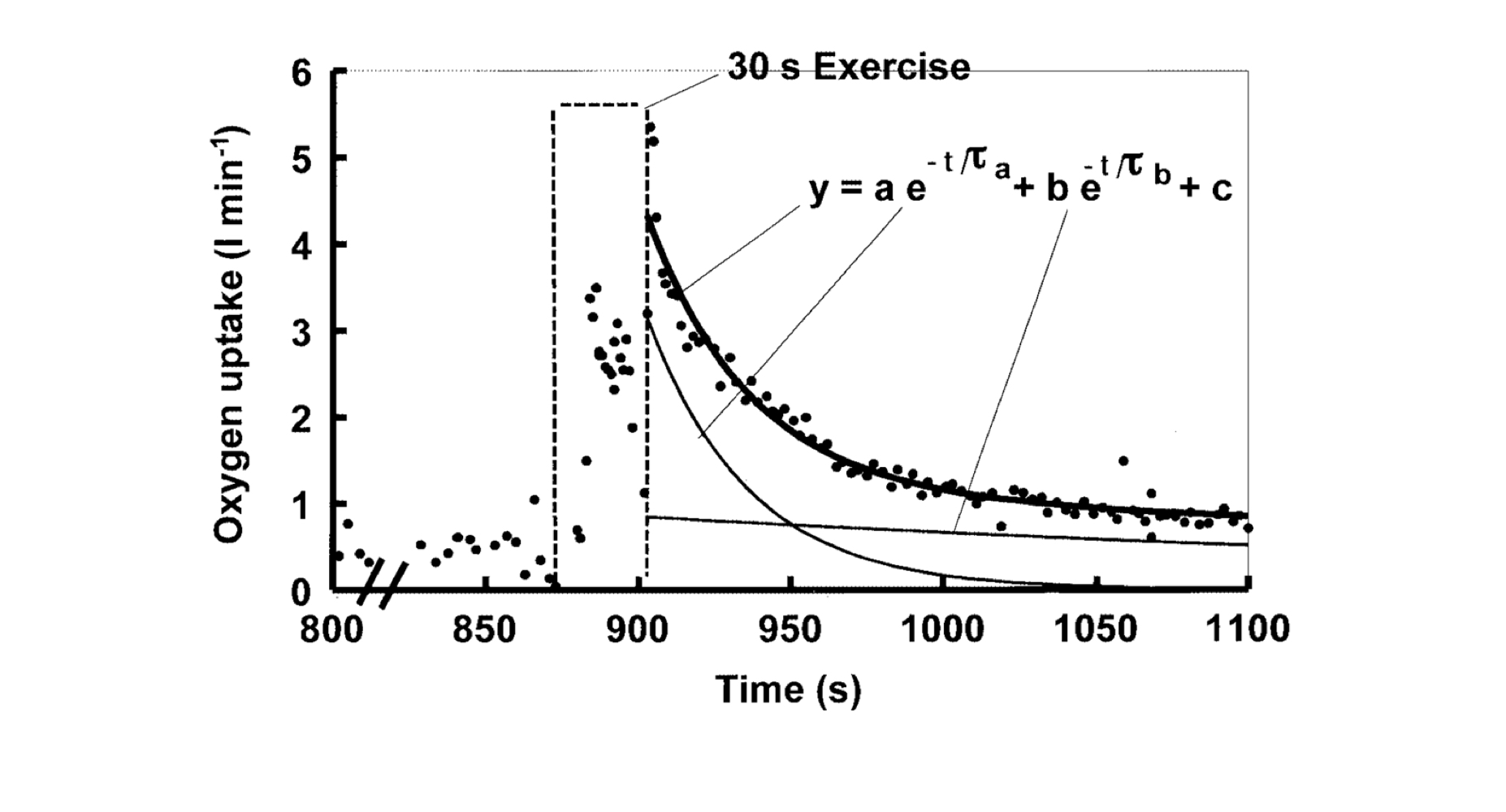
Excess post-exercise O2 consumption
“recovery oxygen”
Area under the VO2 curve above resting VO2
timescale = minutes
Provides oxygen for oxidative phosphorylation, which supplies energy for recovery processes
Kinetics are biphasic
Kinetic components of excess post-exercise O2 consumption
Fast component: ~0.5-4 L O2
resaturate myoglobin with O2
replensih phosphagens
O2 cost od increased Ve and cardiac work
Slow component: ~5-14 L O2
elevated body temp
catecholamine-stimualted metabolism
O2 cost of increased Ve and cardiac work
increased Na-K-ATPase activity
Some negative effects of exercise are considered “damage” these are:
Oxidative modifications of proteins (oxidative stress)
Muscle damage and soreness
Inflammation
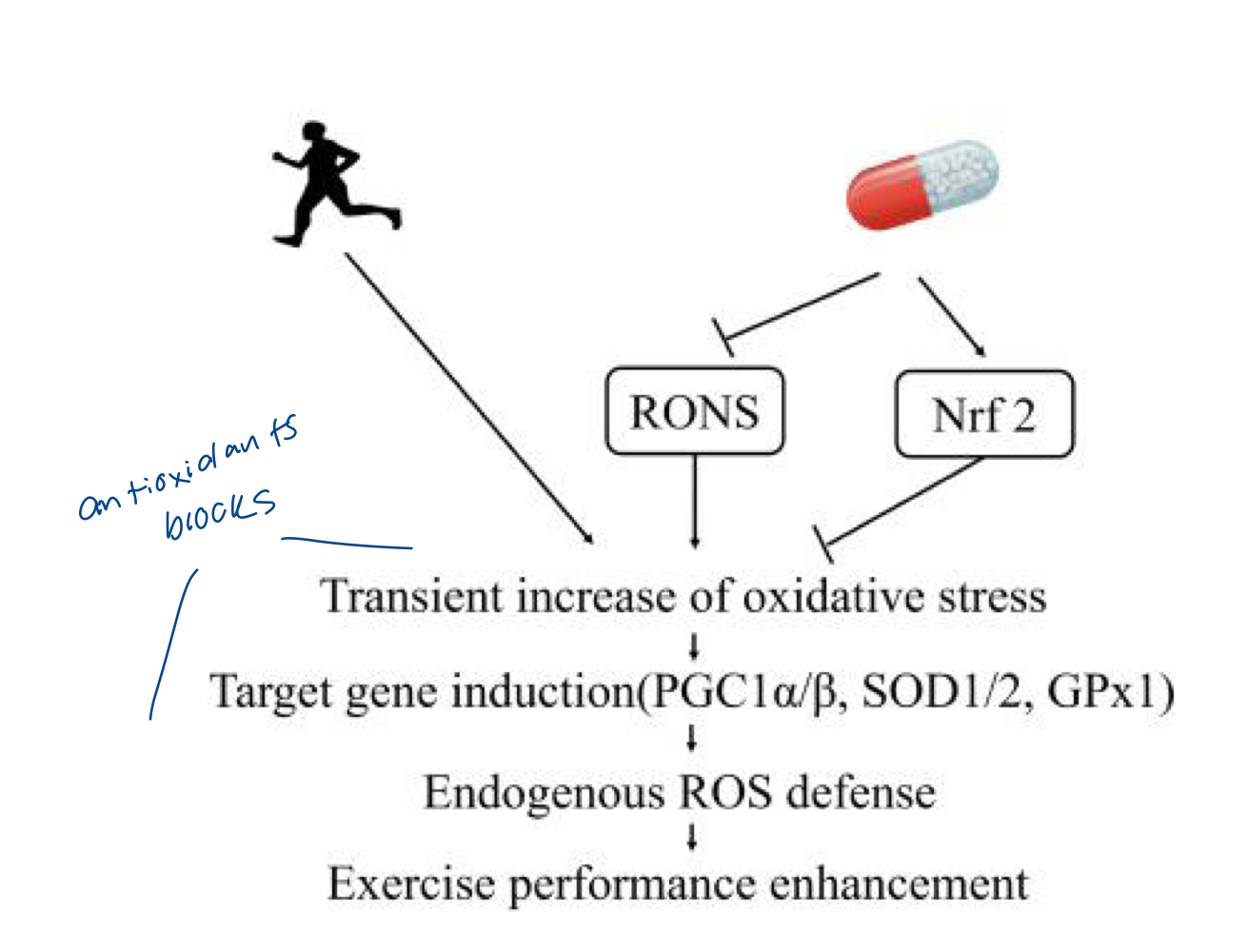
Muscle contration increases rate of free radical production, this does what?
They exert positive and negative effects on the cell
Primary reactive oxygen and nitrogen species (eg superoxide, O2-, H2O2) produced inv arious sites inside and outside muscle cells, happens by accident in ETC or any time we use O2
Positive effects:
help maintain force production (Ca handling), glucose uptake, insuling signalling
Promote exercise training adaptations through transcription control
Promotes muscle antioxidant defence
Negative effects:
oxidative stress: excessive or poorly lcocalized free radical oxidize lipids, DNA and proteins
Unfamiliar eccentric exercise causes:
Muscle damage and delayed-onset muscle soreness (DOMS - feel 24-48 hrs and then gets worse over a couple days)
Common training techniques and exercise modalities involve eccentric contractions
Eg. walking/running downhill, climbing or stepping down stairs, lower phase of a bicep curl, landing phase of a jumping exercise
Consequences of muscle damage
Prolonged (days to weeks) loss of function
Reduced strength
reduced mobility
pain
swelling
Second bout effect: same activity again will cause significantly less pain/DOMS
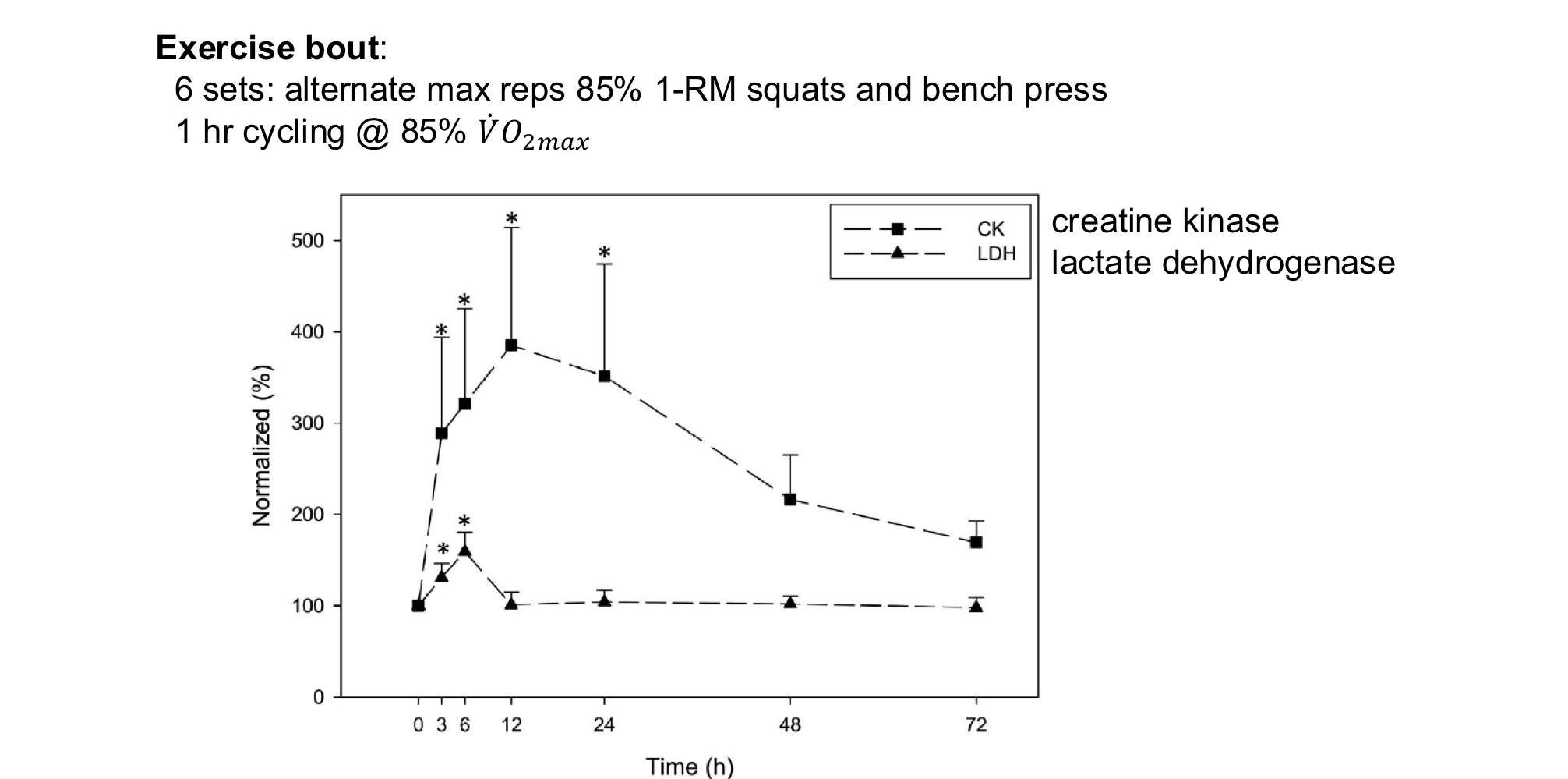
Biochemical and histological symptoms of muscle damage/DOMS
Elevated muscle enzymes in blood: creatine kinase, lactate dehydrogenase, etc
Ultrastructural damage
Immune cell infiltration
Degradation and regeneration of muscle fibers
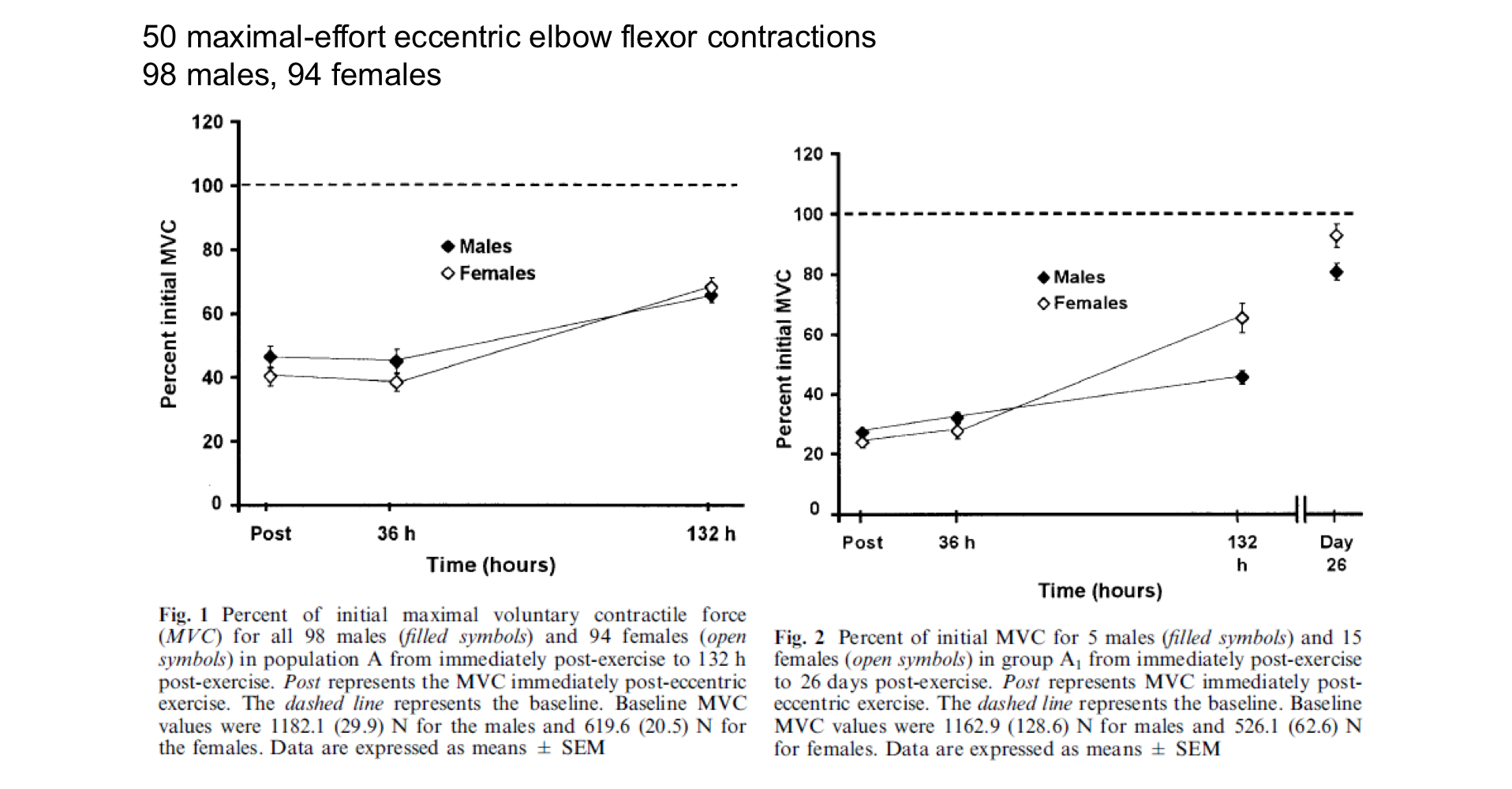
Kinetics of muscle function recovery in response to damaging exercise
Maximal voluntary contraction force normally recovers within ~3 weeks
Muscle enzymes _____ in blood in response to damaging exercise. Which ones?
Accumulates
Creatine kinase and lactate dehydrogenase
Role of muscle damage and repair in the training response is controversial
Muscle damage is limited beyond the resposne to the original eccentric exercise (eg. repeated bout effect, it reacts to damage by producing an adaptive response that endows resistance to subswwequent exercise-induced damage stimuli)
Training is often viewed as a “cycle of breakdown and repair” and that fatigue/damage are necessary to training: NOT nedcessarily true, adaptations to training result from signalling mechanisms that are stimulated from exercise, magnitudes of stimuli are proportion to exercise duration/intensity, so are negative effects of exercise, mostly correlative, perhaps a partly causal relationship between damage processes and training adaptation
Autophagy and mitophagy, cellular process that involves intraceullar degradation of organelles and other components via the lysosomal pathway, exercise-training adaptations require autophagy
Mitophagy pathway
Damaged mitochondria are tagged for autphagy
Mitochondria are enveloped in a membrane formning a complex called an autophagome
A lysosome attached to the autophagosome forming an autolysosome
Enzyme are released and difest the mitochondria
Inflammation caused by exercise
Exercise elicits the acute phase response, the coordinated systemic response to infection or aseptic damage
Cytokines and acute phase proteins have an increase in blood concentration in the hours to days following stimulus
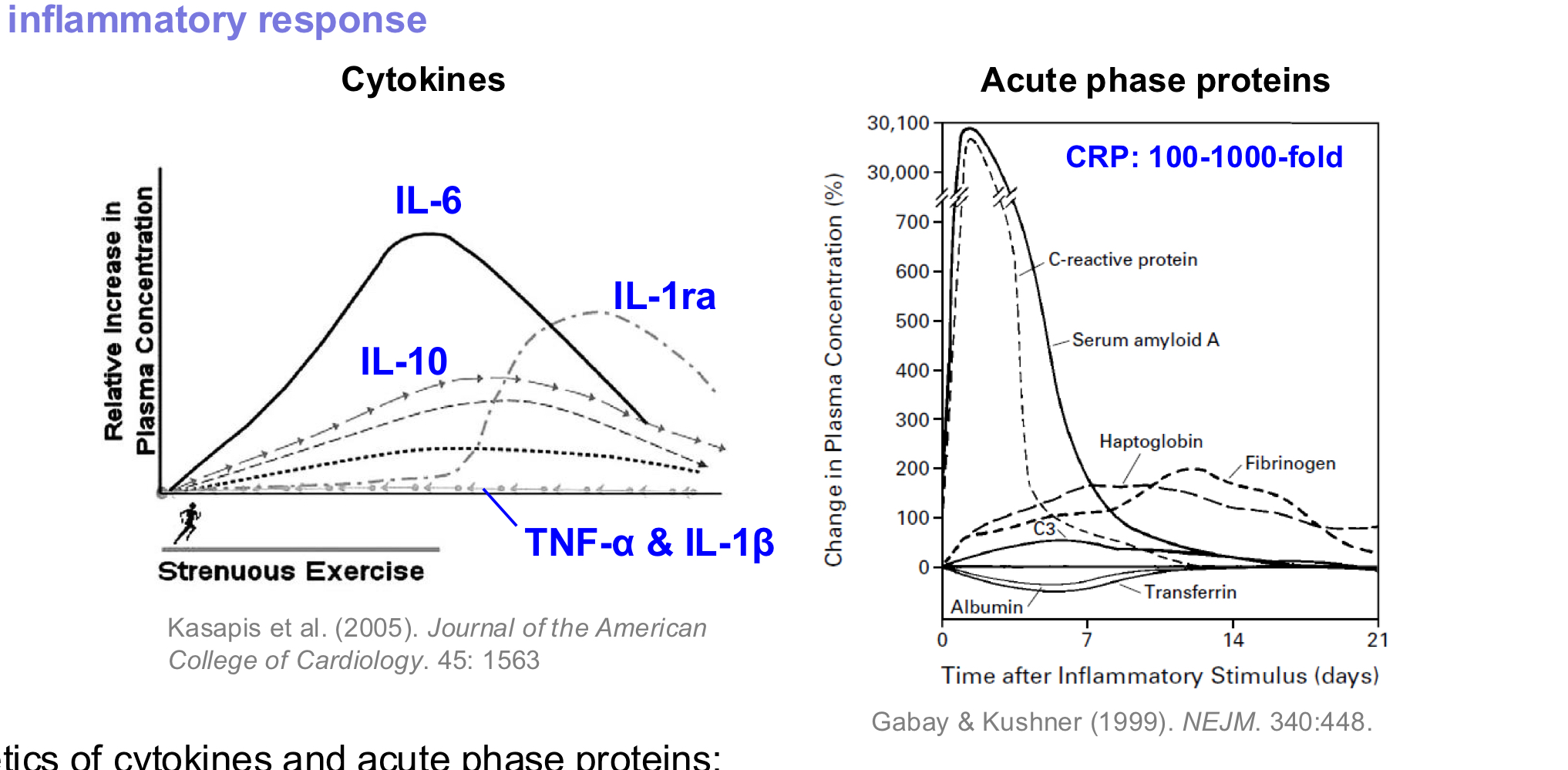
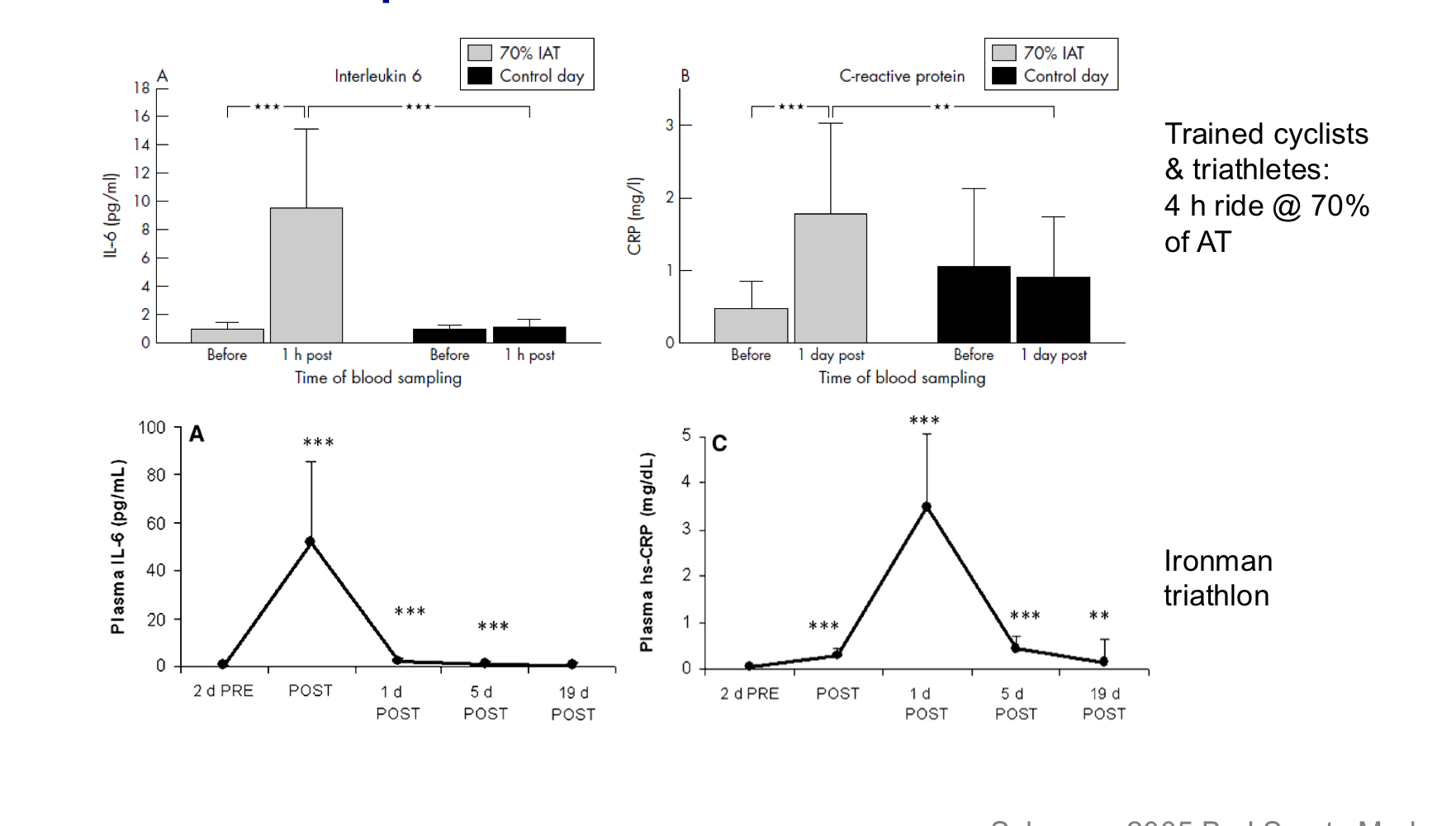
Acute phase response in trained athletes following prolonged strenuous exercise
Elevated IL-6 (interleukin-6) precedes elevated CRP (c-reactive protein)
**both are cytokines that are released in response to acute inflammation
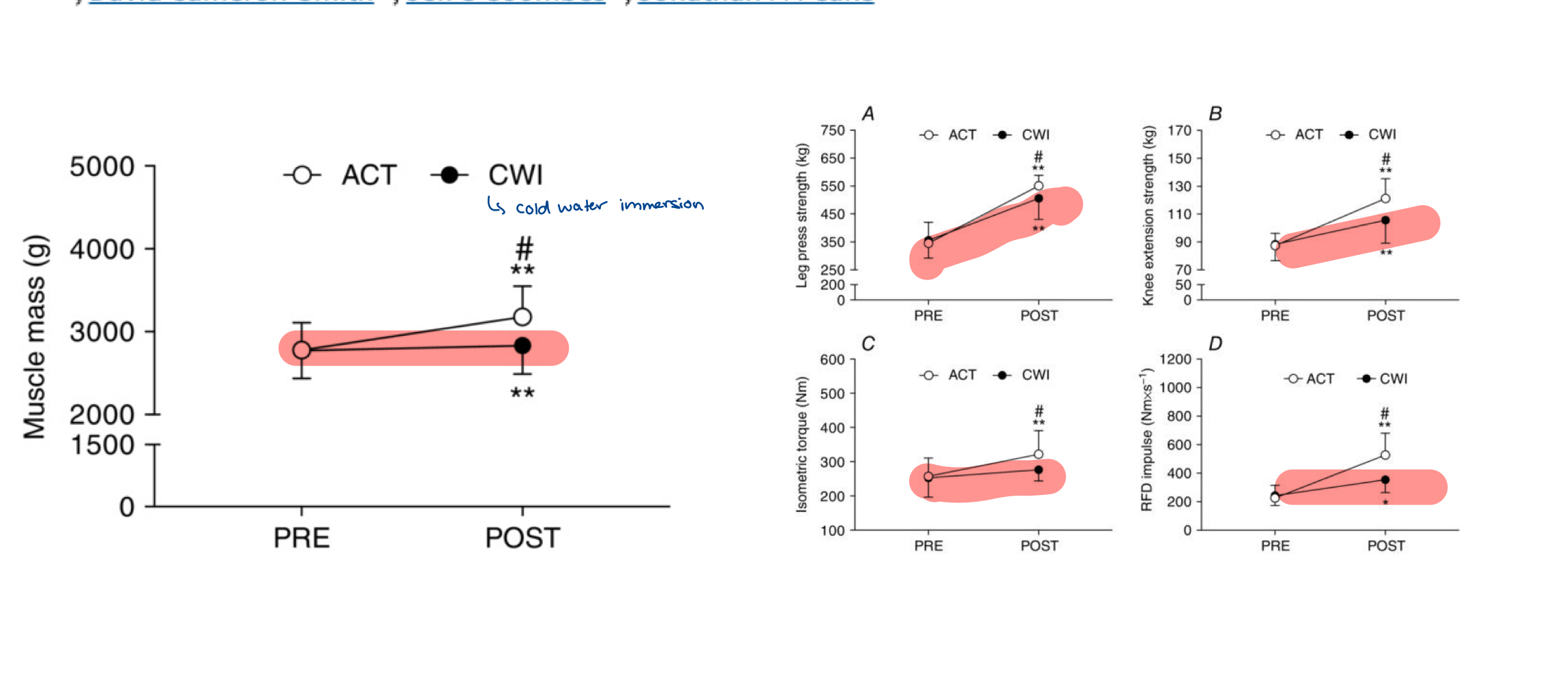
Post-exercise cold water immersion
Attenuates acute anabolic signalling and long-term adaptations in muscle to strength training (blunts training process)
Antioxidants
Research has shown they prevent health-promoting effects of physical exercise in humans
Summary of “damage” due to exercise
Not exclusively bad, they reflext natural physiolgoical processes that have psotiive effects deal with aseptic damage. While exercise may cause inflammation, exercise training reduces chronic low-grade inflatmmation associated with disease
Taking antioxidant or anti-inflammatories may suppress training adaptations
Muscle damage/DOMS result primarily from unaccustomed eccentric exercises
Damage biomarkers are used to monitor athletes during training
After a strenuous competition, feverish due to acute phase response, blood profile resembes that from myocardial infarction