Human Development Final Exam Review
Unit 1: Intro and Theoretical Perspectives
What is the difference between growth and development?
Growth is physical growth refering primarily to things like height and weight.
Development encompases a broader range of changes such as functional and behavioural changes, skill acquisition, and overall progress toward maturity.
Three areas of development.
Physical Development are changes in the body and brain. E.g., height and weight, fine and gross motor skills, puberty, and sensory changes
Cognititve Development refers to learning skills, attension, memory, language aquisition and skills, thinking, reasoning, and creativity. It involves the development of skills like problem-solving, decision-making, and understanding.
Socioemotional Development focuses on emoitons, personality, and social realtionships. It encompasses the growth of a child’s capacity to understand, manage, and experss emotions,a s well as form and maintain relationships with others.
Nature vs. Nurture
A crucial debate in understanding human development, emphasizing the roles of genetics and environment in shaping individual differences. This discussion includes examining how inherited traits and family dynamics influence behavior, personality, and overall growth. While genetics provide the foundation for certain traits however, the environment plays a significant role in how those geens are expressed and how we develop. E.g., someone might have a geentic predisposition towards aggresssion, but thier environment can either exacerbate or mitigae this tendency. Epigenetics also plays a cruicial role as environmental factors can change which genes are expressed therefore immpacted biological traits. The environment can also negatively impact a person preventing them from reaching their biological potential (i.e., height because of malnutrition).
Nature Traits
Pysical features like height, weight, eye colour, hair colour, and skin colour
Predisposition for diseases like mental illnesses, cancer, and heart disease
Nurture Influences
Social relationships
Culture and religion
Socioecenomic factors
Parenting styles
Education
Each of the following concepts below can be linked to a developmental theorist studied in this course. Identify the thoerist the concept amtches with and explain whtat the concept means.
Unconscious mind
Theorist: Sigmund Freud
The unconscious mind is part of the mind that contains thoughts, memories,a nd desires that are below the surface of conscious awareness but still influence behaviour. Freud believed that many of our actions are driven by unconscious motoviations, especially those rooted in childhood exxperiences.
Trust vs. Mistrust
Theorist: Erik Erikson
This is the first stage in Erikson’s psychosocial theory of development (birth to 18 months). In this stage, infants learn whether or not they can trust the world base don how consistently and lovinfly thier needs are met by caregivers. A strong sense of trust leads to secure developmenet.
Idenity vs Identity Confusion
Theorist: Erik Erikson
This is the fifth stage of Erikson’s thoery (adolescence). During this period, teens explore different roles and ideas to develop a personal identity. Success leads to a strong sense of self, while failure results in confusion about one’s place in society.
Positive Reinforcement
Theorist: B.F. Skinner
Positive reinforcement is a concept in operant conditioning where a desirable stimulus is added after a behavior to increase the likelihood of that behavior happening again (e.g., giving praise or areward after a child cleans their room).
Fixation
Theorist: Sigmund Freud
Fixation occurs when an individual remains stuck in one of Freud’s psychosexual stages due to unresolved conflicts. E.g., fixation at the oral stage may lead to habits like smoking or nail-biting in adulthood.
Egocentrism
Theorist: Jean Piaget
Egocentrism refers to the difficulty young children (especially in the preoperational stage, ages 2-7) have in seeing things from another person’s perspective. Piaget observed that children often assume others share their thoughts and viewpoints.
Id, Ego, Superego
Theorist: Sigmund Freud
These are three parts of the personality according to Freud:
Id: Operates on the pleasure principle; seeks immediate gratification
Ego: Operates on the reality principle; mediates between the id and the external world
Superego: Represents internalized societal norms and morals; acts as the conscience
Jean Piaget’s thoery of intellecctual development: Children progress through four distinct stages of cognitive development: sensorimotor, preoperational, concreate operational, and formal operational. These stages are characterized by qualitative differences in how children think and reason, with each stage building upon the previous one.
Stages:
Sensorimotor Stage (0-2 years)
Infants learn primarily through their senses and actions, developing objet permanence (understanding that objects continue to exist when out of sight) and basic motor skills.
Preoperational Stage (2-7 years)
Children develop symbolic thinking, language, and pretend play. However, they struggle with logical reasoning and conservation (understanding that properties of objects remain the same despite changes in appearance).
Concrete Operational Stage (7-11 years)
Children begin to think logically about concrete events and develop concepts like conservation, reversibility, and classification.
Formall Operational Stage (12 years and older)
Adolescents develop the capacity for abstract thought, hypothetical reasoning, and deductive logic.
How it differs from Montessori’s theory: Montessori provides a specific educational model that emphasizes individualized learning, self-directed activity, and a prepared environment with specific materials designed to foster development. Piaget emphasizes how thinking develops in stages and focuses on the internal processes of the mind. Montessori emphasizes what supports learning and focuses on the external environment and freedom within structure.
Unit 2: Neurospcyhology and Prenatal Development
Each of the following terms below is related to brain development. Explain each term’s function or role in brain development.
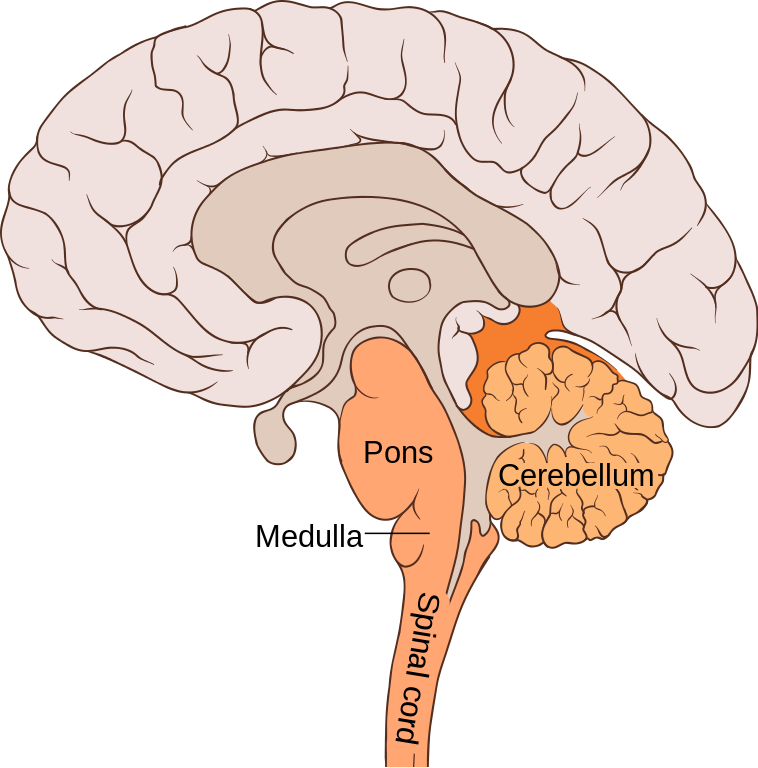
Brain Stem
Is in the lowest part of the brain (just above the back of the neck) and controls many vital functions, such as breathing, heart rate, and blood pressure, and the nervesand muscles used in seeing, hearing, walking, talking, and eating.
Prefrontal Cortex
A part of the frontal lobe located at the front of the brain, responsible for higher-level cogntive functions, personality, and decision-making. It plays a crucial role in planning, working memory, social behaviour, and emotional regulation.

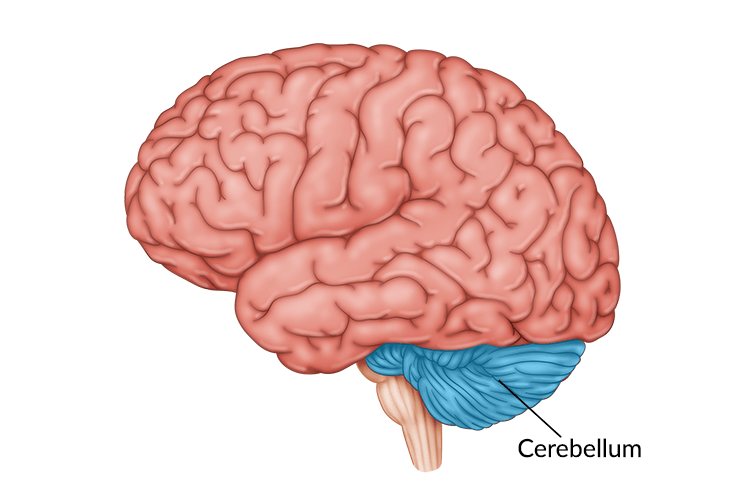
Cerebellum
Plays a crucial role in coordinating voluntary movements, maintaining balance and posture, and enabling motor learning. It ensures that we can stand, walk, and move without falling.
Corpus Callosum
Vital structure in the brain, acting as a bridge of nerve fibers that connects the left and right cerebral hemispheres. This connection facilitates communication and coordination between the two sides of the brain, enabling them to work toegther for various functions like sensory processing, motor control, and higher-level cognitive tasks.
:max_bytes(150000):strip_icc()/Corpus-Callosum-58d16cd45f9b581d727aa487.jpg)
Neural Pathways
The brain’s information super highways, formed by interconnected neurons that transmit signals between different parts of the brain, or between the brain and rest of the body. These pathways are curcial for everything from basic bodily functions to complex cognitve processes like learning and memory.
Pruning
The natural process of eliminating unnecessary or weak connections between neurons (synapses). This process helps to refine neural circuits and improve the brain’s efficiency, making it more adaptable to handle new information. It begins in early childhood and ocntinues to adulthood. Different regions of the brain prune at different times, with the visual cortex pruning earlier than the prefrontal cortex.
Synapses
Specialized junctions where nerve cells (neurons) communicate with each other or with other types of cells like muscle cells. These junctions are crucial for transmitting nerve impulses, enavling the nervous sytem to function. Synapses can be either chemical, using neurotransmitters to carry signals, or electrical, where ions flow directly between cells.
Dendrites
The afferent component of a neuron that branches extensively into a dendritic tree, tapering distally with each successive branch. Dendrites play a curical role in receiving tand processing synaptic signals in the brain. They receive information from other neurons, called pre-synaptic neurons, or from the environment. The signals from pre-synaptic neurons come in the form of neurotransmitters.
Neurotransmitter
Chemcial messengers that transmit signals between neurons or from neurons to other cells like muscle or gland cells. These molecules play a curical role in various bodily functions, including mood, movement, and sleep.
Cephalocaudal Development
The pattern of growth that proceeds from the head down, following the head-to-toe direction. This means that during infancy, infants develop control of their head and neck first, followed by their arms and legs. This principle is a fundamental aspect of physical and motor development.
Proximodistal Development
The pattern of growth that proceeds from the center of the body outward to the extremities. This means that infants gain control of their trunk and limbs before they develop fine motor skills in their hands and fingers.
What is conception? Name and describe the three periods of prenatal development.
Conception refers to the fertilizattion of an egg by a sperm marking the beginning of preganancy.
Prenatal development is divided into 3 periods and lasts approximately (266-280) days (10 months).
Germinal period: first 2 weeks after conception, zygote is created
Rapid cell division by the zygote
Blastocyst: group of cells that develop after about 1 week - later turn into the embryo
Trophoblas: outer layer of cells that later provides nutriiton and support for the embryo
Implantation: attachment of the zygote to teh uterine wall: occurs 10 to 14 days after conception
Embryonic period: occurs from 2 to 8 weeks after conception
Begins when blastocyst attaches to uterine wall
Mass of cells is now called an embryo
Three layers of cells: endoderm, mesoderm, and ectoderm
Amnion: a bag that ocntains a clear fluid (amniotic fluid) in which the embryo floats
Umbilical cord: connects the baby to the placenta
Placenta: group of tissues containing mothers and baby’s intertwined blood vessels
Organogenesis: process of organ formation during the first two months of prenatal development - very vulnerable to environmental changes
Fetal period: begins 2 months after conception and lasts until birth
Rapid growth and change
Viability: the age at which a fetus has a chance of surviving outside the womb
Currently 24 weeks: changes with advances in medical technology
Hazars to Development
Teratogen: any agent that can cause a birth defect of negatively alter cognitve and behavioural outcomes
Perscription and non-perscription drugs - known perscription teratogens include antibiotics, some antidepressants, some hormones, and accutane; non-perscription teratogens include aspirin and diet pills
Psychoactive drugs - drugs that act on the nervous system to alter states of consciousness, modify perceptions, and change moods; includes caffeine, alcohol, nicotine
Caffeine - small risk of miscarriage and low birth weight for those consuming more than 150 mg daily; increased risk of fetal death for those consuming more than 300 mg daily; FDA recommends not consuming caffeine or consuming it sparingly
Alcohol - fetal alcohol syndorme: abnormalities in newborn due to mother’s heavy use of alcohol in pregnancy (facial deformities, defective limbs, face and heart, most have below-average intelligence); even light to moderate drinking during pregnancy has been associated with negative effects on the fetus; FDA recommends no alcohol consumtion during pregnancy
Nicotine - maternal smoking can negatively influencce prenatal development, birth, and postnatal development; associated with: preterm briths and low birth weight, fetal and neonatal death, respiratory problems, SIDS, ADHD
Illegal drugs that harm during pregnancy - cocaine, methamphetamine, marijuana, heroin, etc
Incompatible blood types (Rh factor) - can cause mtoher’s immune system to produce antibodies that will attack the fetus
Environmental hazards - radiation, environmental pollutants and toxic wastres
Maternal diseases - sexually transmitted diseases (syphilies, genital herpes, AIDS), rubella, gestational diabetes
Maternal factors - maternal diet and nutrition, maternal age, emotional states and stress
Paternal factors - exposure to teratogens, paternal age
Unit 3: Infancy and Childhood
Define attachment. How does attachment help promote growth and development?
Attachment refers to the strong, emotional bond that develops between an infant and their primary caregiver. This bond is crucial for healthy development, as it provides a secure base from which a child can explore the world and learn to regulate their emotions.
A secure attachment provides a child with a sense of safety and security, allowing them to confidently explore their environemnt, knowing they have a reliable caregiver to return to for comfrot and support.
Emotional regulation - thorugh interactions with a responsive caregiver, a child learns to identify, understand, and mange their emotions, particularly in stressful situations
Social skills development - seccure attachment fosters positive soical interactions, helping children develop empathy, cooperation, and ability to form healthy relationships with others
Cognitive development - by providing a safe and stimulating environment, secure attachment supports cognitive development, including language acquisition, problem-solving skills, and overall learning.
Resilience - children with secure attachments are better equipped to cope with adveristy and bounce back from challenges, demonstrating greater resilience throughout life
Brain development - experiences associated with secure attachment, such as responsive caregiving and a safe environment, positively influence brain development, particularly in areasa related to emotional regulation and higher-level thinking
For each term below, identify whether it is most related ot Harlow, Bowlby, or Ainsworth. Explain the significance of the term in understanding attachment.
Monkey
Theorist: Harry Harlow
Harlow conducted experiments with baby rhesus monkeys using wire and cloth “mothers” to show that comfort and emotional security are more important to attachment than just feeding. His work demonstrated that physical closeness and warmth are key to atttachment, not just survival needs.
Protest’
Theorist: John Bowlby
Bolby observed the “protest despair detachment” response in children seperated from caregivers. “Protest” is the initial phase when a hcild reacts with crying, clinging, or searching for the caregiver. It shows that attachment bonds are strong and distresssing to lose, even temporarily.
Secure Base
Theorist: John Bowlby
The idea that a caregiver provides a secure emotional foundation from which the child can explore the world. This concept is central to Bowlby’s Attachment Theory, showing that secure attachments promote confidence and curiosity in children.
Exploration
Theorist: Mary Ainsworth
In Ainsworth’s strange situation study, securely attached children used their caregiver as a secure base from which to explore the room. The amount and type of exploration a child engages in reflects the quality of attachment, helping to identify secure vs. insecure attachment styles.
Attachment Theory
Theorist: John Bowlby
Bowlby is the ofunder of attachment theory, which explains how early relationships with caregivers shape a child’s sense of security and influence future emotional and social development. It integrates biological and emotional needs as foundationns for healthy relationships.
Critical Age Hypothesis
The critical age hypothesis (CPH) suggests that there’s a specifc time window, primarily in early childhood, during which language acquisiiton is most effective and can lead to native-like fluency. While the exact age rangew is debated, the CPH generally posits that language learning becomes more hclalengin and less successful after this period, often proposed to end around puberty or even later in some cases.
Define the following types of play. Which age gorup(s) is most likley to engage in this type of play?
Unoccupied
THe earliest stage of play in infancy. It is characterized by a baby’s seemingly random movements and explorations of their body and surroundings without a specific goals or adult direction. It’s a crucial period for development, laying the foundation for future learning and interaction. Babies explore using their own limbs, movements, and senses, like kicking their legs or putting thier hands in their mouth. These seemingly random movements help babies develop coordination and control over their bodies.
Onlooker
Children observe other children playing without actively participating. Duriing this stage, a chid will watch another childs activiites, sometimes commenting or asking questions about the play, but won’t join in. This behaviour is common in toddlers around the age of 2 and is an important step in learning social skills and understanding how play works.
Solitary
Also known as independent play is when a child plays alone, engaing in activites without itneraction with others. This type of play is a natural part of early childhood development (three months to two years old) and offers numerous benefit for a child’s growth. It allows children to explore, exp[eriment, and develop important skills at their own pace. E.g., puzzles, drawing, reading, or blocks
Parallel
Children play alongside each other, but not together, typically between the ages of 18 months to 3 years. They might be in the same area, using similar toys, but they are not interacting or influencing each other’s play. This stage is a precursor ot more social forms of play and helps children develop social skills, language, and an understanding of their own and other’s emoitons.
Associative
Children interact wiht each other while playing, but without a common goal or organized structure. It’s astep beyond parallel play, where children play independently near each other, and towards cooperative play, where they work together towards a shared objective.
Cooperative
A type of social play where children actively work together towards a shared goal, often involving treamwork, communication, and rule setting. It’s crucial strage of development, fostering socioemotional and cogntive skills, and typically emerges around ages 4-5.
Play throughout the lifespan
Infancy
(0-2) years
Sensorimotor development: toys like rattles or peek-a-boo games help infants undesrtand object permanence and cause-and-effect
Attachment & bonding: interactive play like tickling or singing stengthens emotional bonds with caregivers and fosters a sense of trust
Childhood
(3-12 years)
Social skills: playing games with others (e.g., tag, board games) teaches turn-taking, cooperation, and conflict resolution
Language & imagination: pretend play like playing house or superheroes encourages creativity and expands vocabulary and storytelling abilities
Adolescence
(13-18 years)
Identitiy formation: participating in sports, drama, or video games helps teens explore roles and strengths, contributing to self-concept
Stress relief & emotional regulation: engaging in hobbies or recreational play like music or skateboarding povides healthy outlets for stress and emotinal expression
Adulthood
(19-64 years)
Relationship building: playing games with friends, partners, or children builds connection, communication, and intimacy.
Cognitive stimulation: strategy based games (e.g., chess, puzzles) help keep the mind sharp and enhance problem-solving skills
Old-age
(65+)
cognitve maintenance: playing memory games, card games, or doing crosswords helps slow cogntive decline and maintain mental agility
Social engagement: Group play (e.g., bingo, dancing, storytelling) reduces loneliness and supports emotinal well-being
Identify three suggestions by the American Academy of Pediatrics with regards to children and television viewing
Limit screen time. For children under 18 months avoid screen time execept for video chatting. For ages 2-5 limit screen use to 1 hour per day of high-quality programing. For ages 6 and older place consistent limits on screen time to ensure it doesn’t interfere with sleep, physical activity, or socia interaction.
Co-view and discuss content. Parents should watch programs with their children to help them understand what they’re seeing and apply it to the real world. Active engagement like asking questions or connecting the content to everyday life, helps children build critical thinking skills and language skills.
Avoid using screen as emoitonal pacifiers. The AAP adivses not to use TV or devicese to calm or distract children, espeiclaly during tantrums or distress. Instead, parents hsould hlep children develop self-regulation skills and healthy coping strategies.
For each type of deprivation mentioned, identify a minimum of two potential negative consequences on any area of growth and development.
Attachment and bonding
Emotionla insecurity - children may develop anxiety, fear, or trust issues, struggling to form healthy future relationships
Cognitve delays - lack of secure attachment can interfere with brain development, leading to poor attention and learning difficulties
Social interaction and play
Delayed social skills - children may struggle with sharing, empathy, cooperation, and understanding social cues
Language development issues - fewer social exchanges can lead to limited vocabulary and poor communication abilities
Exercise
Poor physical health - can lead to obesity, weak muscles, and underdeveloped motor skills
Mental health struggles - lack of movement is linked ot higher rates of depression, anxiety, and poor emotional regulation
Propery healthy nutrition
Stunted physical growth - malnutrition can result in short stature, weekened immune system, and delayed puberty
Cognitve impairment - poor nutirtion, espeically in the early years, can negatively impact memory, focus, and IQ development
Regular exposure to language and verbal communication
Delayed speech and language skills - children may have limited vocabulary, poor grammar, and trouble expressing needs
Academic challenges - language delays often lead to reading difficulties, poor comprehension, and lower school performance
Unit 4: Adolescence
Puberty and changes in adolescence
Changes include the development of secondary sexual characteristics, growth spurts, and the ability to reporudce. Accompanying the physical changes are cogntive and emotional shifts, sucha s increased abstract thinking, mood swings, and growing awareness of self and others. Puberty begins between the ages of 8 and 13 in girls and 9 and 14 in boys.
Growth spurts: adolescence can expereince rapid changes in height and weight
Secondary sexual characteristics: breast development and menstruation in females, and the grwoth of pubic hair, underarm hair, and facial hair in both sexes
Hormonal changes: trigger puberty and infleunce physical development
Voice changes: larynx grows, causing a change in voice pitch sometimes leading to voice cracking in males
Body odor and acne: increased oil production in the skin can lead to body ordor and acne
The role of brain development in schizophrenia
Schizophrenia involves structual and funcitonal changes in various brain regions, particularly within the coretex and interconnected areas. Key structures include the prefrontal cortex, hippocampus, and temporal lobe, which show reduced gray matter volume and dsiruptions in connectivity.
Cortex:
Structural deficits like reduced gray matter volume and disrupted white matter integrity are observed in the cortex, particularly in regions involved in language processing and higher-level cognitive functions.
Prefrontal Cortex:
This area, crucial for executive functions, decision-making, and working memory, shows reduced activity and volume in individuals with schizophrenia.
Hippocampus:
Involved in memory formation and spatial navigation, the hippocampus shows reduced volume and altered activity, potentially contributing to memory problems in schizophrenia.
Temporal Lobe:
Specifically, the superior temporal gyrus, associated with auditory processing and language, shows structural and functional abnormalities.
Two friends have grown up together since kindergarten. They are both female, the same age, have university degrees, and have the same circle of friends. However, one is an alcoholic and drug abuser and the other is not. Identify all the possible reasons why only one became addicted to drugs and alcohol even though they have markedly similar life experiences and characteristics.
Biological and genetic factors: one may have a family history of addiction, increasing their biological susceptibility. Differences in how their brains respond to subtances (e.g., dopamine levels, reward sensitivity) can make one more prone to dependence.
Psychological and emotional factors: one might struggle with anxiety, depression ,m or trauma, using substances as a form of medication. They may differ in how they cope with stress; one may turn to substance while the other uses healthier outlets
Family and early life experiences: how they were raised (e.g., emotional suport, boundaries, or exposure to substance use) can shape future behaviour. Early exposure to drugs and alcohol earlier or in a more permissive environment
Socail and Environmental factors: peer pressure even within the same friend group and unique interation or experiences at parties or events can lead one to experiment more heavily. One might have experienced a toxic relationship, breakups, or loss, which can trigger substance use.
Personality traits: one may naturally be more impulsive or sensation-seekin. Lower self esteem or a ened for acceptance can make someone more vulnerable to external forces.
Access to help and support: one may have had more access to mental health services or supportive conversatons that prevented dependence. Awareness and education about the consequences of addiction or differenet personal boudnaries regarding substance use.
Why disorders emerge in individuals
Biological factors like genetics, brain chemistry and an overactive amygdala
Psychological factors like trauma, stress, negative thinking patterns, and learned behaviour
Environmental and soical factors like lack of emotional support, neglect, life stransitions and stress, and peer and social influence
Unresolved emotional conflict sucha s suppressed emotions and lack of coping skills
Sociopathy is a unique disorder in that there are consistent patterns of behaviour from an early age. Imagine you were a teacher. What types of behaviours/signs would you look for in order to determine whether your student was a sociopath or not.
Persistent aggression and cruelty
Chronic lying and manipulation
Rule breaking and defiance
Lack of empathy and remorse
Shallow or superficial emotions
Difficulty forming genuine relationships
Early signs of conduct disorder like distruction of property, theft, aggression toward people or animals
Cortisol vs Dopamine
Corisol: stress hormone released during stressful or dangerous situations to help the body respond to stress. Long term high levels of cortisol can cause anxiety, fatigue, and weakened immune system
Dopamine: a feel-goo neurotrasnsmitter linked to pleasure, motivation, and reward. It is released during enjoyable or rewarding experiences. High dopamine can lead to risky behaviour or addiction.
Types of stress and impacts on the body
Positive stress (eustress): short term, mild stress that can be motivating or helpful (e.g., studying for a test, preparing for a performance). Boosts focus, energy, and alertness
Tolerable stress: more intense but with support and coping, the body can recover (e.g., breakup, losing a job). Temporary strainn on mood or body, but not permanent damage.
Toxic stress: prolonged or reepeated strese without support (e.g., abuse, neglect, long-term poverty). Harmful to brain development, weakens immune system, can lead to anxiey, depression, or heart disease.
Socialization
Socialization is the lfielong process by which individuals learn values, norms, behaviours, and social skills necessary to function in society. It helps people understand how to interact with others and what is considered acceptable behaviour. Influences include family, school, peers, media, and culture.
Parenting styles
Authoritative: sets clear rules and expectations but also lsitens to the child’s thoughts and feelings. Uses postive disciplines like time outs and natural consequences instead of harsh punishment. Encourages independence and responsibility while providing guidance and support.
Impacts on children: high self esttem, good social and emotinal skills, strong academic performance, more independent and responsible.
Authoritarian: very strict wiht ltitle flexibility or open discussion. Focuses on obedience, discipline, and often uses punishment. Does not encourage input from the child and may use phrases like because i said so.
Impacts on children: obedient, but may lack social competence, low self-esteem, higher levels of anxiety or resentment, difficulty making decisions or thinking independently.
Permissive parenting: very lovng and accepting but sets few rules or boundaries. Rarely enforces consequences; wants to be more of a friend than a parent. Allow children a high degree of freedom, even when not age appropriate.
Imacts on children: may struggle with self discipline, can become impulsive or demanding, lower academic performance, may have difficulty respecting authority or rules
Neglectful: Emotionally distant, uinvolved in the child’s life. Provides basic needs (food, shelter) but little guidance, attention, or affection. Often overwhelmed by personal issues (e.g., mental health, substance abuse) or lacks parenting knowledge.
Impact on Children: poor self esteem, struggles with emotional regulation, higher risk of academic failure, depression, or substance abuse. May seek attachment or validation from peers in unhealthy ways.
Worst parenting style
Neglectful (uninvolved) parenting style is widely associated with the most negative developmental outcomes because it provides neither emotional support nor structure.
→ Low self esteem and poor emotional regulation due to lack of nurturing
→ Difficulty forming and maintaining healthy relationships; may become socially withdrawn or oerly dependent on peers
→ Poor academic performance due to lack of parental involvement and guidance
→ Limited understanding of right and wrong; may be more likely to engage in risky or antisocial behaviour
Best parenting style
The authoritative parenting style is linked ot the most postive overall outcomes because it balances warmth and structure and high expectations
→ High self confidence and emotional resilience
→ strong social skills and the baility to build healthy, respectful relationships
→ High academic achievement and strong problem-solving skills
→ A strong internal sense of right and wrong and respect for rules
Mean World Syndrome
Mean world syndrom is a term coined by media scholar George Gerbner. It refers to a phenomenon where heavy exposure to violent media causes people, especially children, to believe the world is more dangerous, hostile, or frightenining than it actually is.
→ increased fear and anxiety
→ aggressive behaviour
→ social withdrawal
→ distroted worldview
Media exposure
While it is true that excessive or violent media can be harmful, thoughtfula nd purposeful media expose can support growth and learning. Here are four specific examples of how media can benefit development.
→ promotes cognitve development, literacy, and curiosity through interactive learning
→ helps children identify and manage emotions, build empathy, and solve problems
→ supports language acquisition and verbal development in both first and second languages
→ encourages creative thinking, story telling skilling, and artistic exploration
Unit 5: Adulthood and beyond
Development in adulthood
Adulthood is divided into three stages:
Early adulthood (20-40 years)
Middle adulthood (40-65 years)
Late adulthood (65+ years)
Key areas of development:
Physical: gradual decline in strength, fertility, and sensory abilities over time
Cognitve: processing speed may slow, but knowledge and experience grow
Socioemotional: focus on relationshp, career, family, and self-fulfillment
Sternberg’s Triangular Theory of Love
According to psychologist Robert Sternberg, love is made up of three components
Intimacy - emotional closeness and connection
Passion - physical attraction and romantic/sexual energy
Commitment - decision to stay together long-term
Different types of love:
non love: absense of all three components
liking (friendship): high intimacy, but low passion and commitment
infatuation (passion: high passion, but low intimacy and commitment
empty love: high commitment, but low intimacy and passion
romantic love: high intimacy and and passion, but low commitedment
companionate love: high intimacy and commitment, but low passion
fatuous love: high passion and commitment, but low intimacy
consummate love: high levels of all three components
Family life cycle
Single young adult (independence, career start)
New couple (marriage/patnering)
Families with young children
Families with adolescents
Launching children (kids leave home)
Emty nest/midlife couple
Aging family members