Behavior Guidance
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
25 Terms
basic behavior guidance- communication and communicative guidance
-appropriate use of commands
-cooperative and uncooperative
-establishes relationship with the child
-allows for successful completion
-supports positive attitude towards health
classifying children’s behavior- Frankl behavioral rating scale
-F4: definitely positive- good rapport, laughter, enjoyment
-F3: positive- acceptance of treatment, cautious behavior, willingness to comply with reservation
-F2: negative- reluctance to accept treatments, uncooperativeness, evidence of negative attitude
-F1: definitely negative- refusal of treatment, forceful crying, fearfulness
-describe objective behaviors in documentation
-”pre-cooperative” if very young and cooperates well
predictors of behavior
-developmental level
-dental attitude
-temperament- can guide behavior
-parental influences- other familial influences
-can assist in anticipating the child’s reaction to care
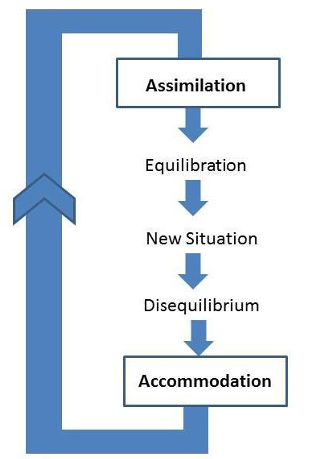
Piaget’s stages of cognitive development
-schema: a cohesive, repeatable action sequence possessing component actions that are tightly interconnected and governed by a core meaning
-building blocks of behavior, organized knowledge
-as the child develops, the schemata become more complex
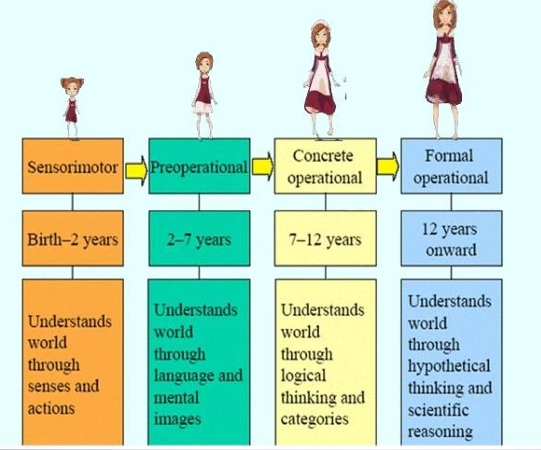
Piage’s stages of cognitive development over time
dental attitude
-past experiences
-familial experiences
-previous exposure: positive- video/cartoon (first dental visit), website; negative- anecdotes, negative imagery
parental influence
-positive attitudes toward oral health care may lead to the early establishment of a dental home
-previous experience can inform the parent’s anxiety- children pick up on parental anxiety
-parenting style can influence a child’s ability to cope with a new or challenging circumstance
-frequently, parental expectations for the child’s response to care (no tears, no crying) are unrealistic- expectations for the dentist guiding the child are great
-may want parent to stand where child cannot see them, but still in the room
pediatric dentistry and parents- positives and negatives
-positives: 2-for-1, can improve dental IQ, can help parents with their homecare, teaching opportunity, can reach other children in family (prevent same outcomes)
-negative: helicopter parents, Wiki-parents, jargon (i.e. oil pulling), parental experience (parents feelings influence behavior)
parenting styles
-health history asks how child is guided at home
-determining style may help with ability to communicate well with parents and children
authoritarian parenting style- characteristics and outcomes
-characteristics: demanding/scheduled, high expectations, not responsive, “snowplow parenting” (removing all obstacles), rules and punishment, reserved warmth
-may lead to: low self-esteem, fearfulness, shyness, may misbehave when parent is absent, obedience = love
authoritative parenting style
-characteristics: high expectations, understanding/support, limits and controls, willing to listen and evolve
-may lead to: child understanding opinions are valued, autonomy, engaging in discussion/negotiations
permissive parenting style
-characteristics: aka “indulgent”, not demanding, lenient, avoid confrontation, nurturing and loving, inconsistent rules, lack of structure
-may lead to: lack of self-discipline, egotistic tendencies, insecurity, lack of motivation, clashing with authority
uninvolved parenting style
-characteristics: no knowledge of child’s life, not present, no requirements, not warm
-may lead to: lack of trust, harder to form relationships with others, low self-esteem, lack of self control
snowplow/helicopter parents
-snowplow: allows/encourages child to have new experiences, removes all obstacles, does not want child to experience discomfort
-helicopter: hover nearby, demonstrate protectiveness, watch over every activity
gentle parenting
-effort to turn away from authoritative style (“mindful”, “intentional”)
-affirms emotions and reactions of child are real and important- validates feelings and reactions
-works against orders
-trend on the rise
-trend away from: positive reinforcers, negative reinforcers
dental fear
-not all children demonstrate identifiable “fear behavior”
-much anxiety wanes as individual matures
-positive early experiences can diminish fear
-fear may stem from perception of appointment
-predictor of disruptive behavior- fear incongruent with circumstance
basic management techniques
-TSD: tell show do
-distraction
-non-verbal communication
-positive reinforcement/descriptive praise
-memory restructuring
-enhancing control
-voice control- falling out of favor, try just lowering volume of voice
-parental presence/abseence
-nitrous oxide (permit necessary in some states)
nitrous oxide
-quick and safe
-child does not necessarily sleep- may fall asleep (not always good)
-relieves anxiety
-STILL NEED TO USE BEHAVIOR GUIDANCE
advanced techniques
-protective stabilization
-”hold and go”
-brevity
-”papoose” board

advanced techniques- protective stabilization
-course
-new consent (separate from other consents), signed and dated by parent
-up to date
-periodicity varies by state
-document, have parents help you put child in papoose
advanced techniques- sedation
-minimal, moderate, deep
-enteral sedation (conscious, oral)
-parenteral sedation (IV)
-permits necessary
-advanced training- residency, sedation courses in some states
-many states are adjusting requirements
advanced techniques- general anesthesia
-hospital OR setting
-ambulatory surgery centers
-private practice- dental/physician anesthetist
-hospital privileges
-pediatric specialists
-understand the referral system in place
-case selection
communication
-smile- when you see parents, at child, eye contact
-learn their names
-listen
-be very specific
-avoid accusation
-include parent in decision making, do not decide treatment for them - address fears
-consistency of message
cultural awareness
-find a translator (not family, not child)
-assure translator conveys tone
-don’t assume someone who speaks the language is a good interpreter
-look at person and talk, then pause for interpreter → don’t just simply talk to interpreter
-do not need to know everything- some knowledge of larger groups within a society may convey more sensitivity
-putting concern on child is most important
-give time to ask questions that may not be common
additional tips for pediatric appointments
-organization
-no lag time
-recognize individual tolerance levels
-some patients are better in the morning
-pivot/adjust based on behavior