Cancers + HIV + Glaucoma + RD
1/79
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
80 Terms
Leukocoria - what cases have it?
Literally "white pupil"
A clinical sign where normal red reflex of eye is replaced by a white reflection
Almost always a pediatric emergency until proven otherwise
Toxocariasis (white puppy + streak)
Coat’s Disease (young boys)
Retinoblastoma (cancer)
Coat’s disease?
Progressive disease (worsens over time)
Starts in young boys <10 yrs old
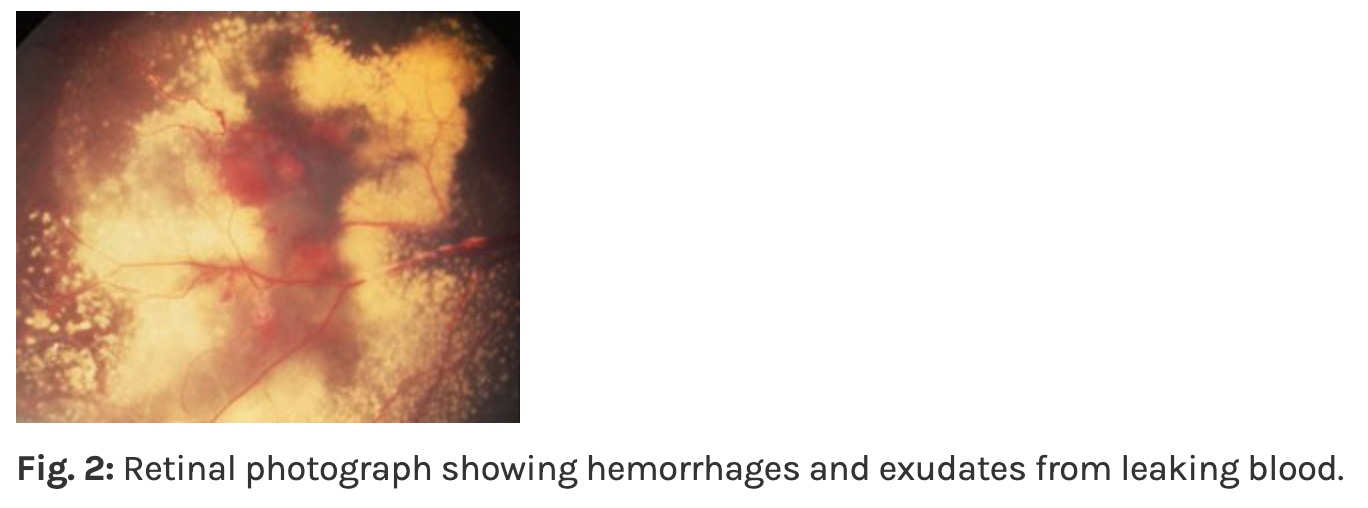
Vascular abnormality → causing leakage of EXUDATES
Exudates become thick + plentiful
Severe enough = cause EXUDATIVE RETINAL DETACHMENT
Exudative RD (aka Serous RD) = type of retinal detachment where fluid collects underneath retina without hole or tear in the tissue
Leaking blood vessels or an inflamed choroid pumps fluid into subretinal space
"Big Three" Causes of Exudative RD:
Inflammatory (Vogt-Koyanagi-Harada)
Patient: Often Hispanic, Asian, or Native American
Signs: Bilateral exudative RDs, "sunset glow" fundus + systemic signs: hearing loss (tinnitus) or vitiligo (white patches of skin/hair)
Neoplastic (Tumors)
Cause: Choroidal Melanoma or Choroidal Hemangioma
Logic: The tumor is highly vascular + "leaky" causing fluid to build up around base of mass
Vascular (Coats' Disease)
Patient: Young boys (as we discussed with Leukocoria)
Logic: The "lightbulb" telangiectatic vessels leak massive amounts of lipid and serous fluid, lifting the retina
Also: optic pits, morning glory syndrome, CSCR
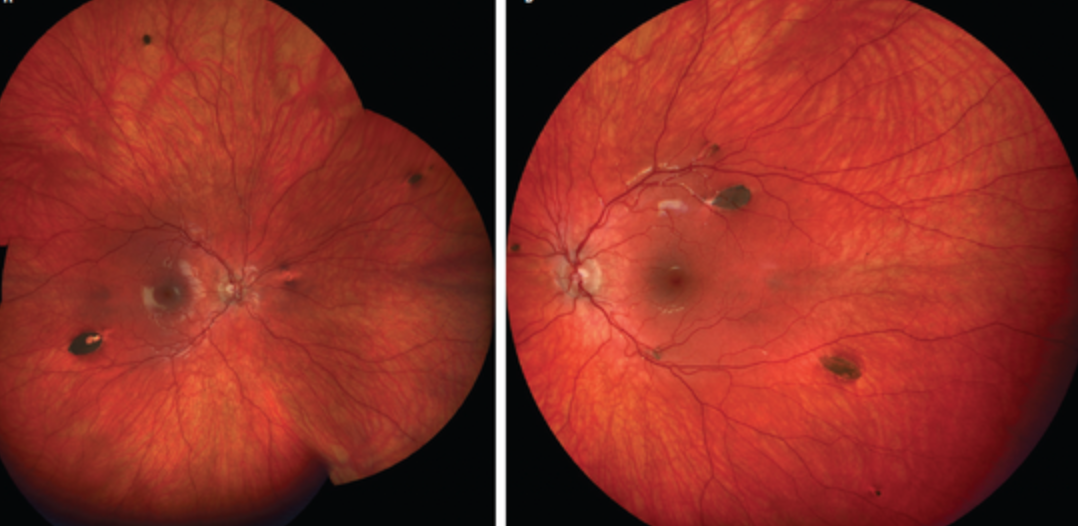
Coat’s disease symptoms?
Poor vision
Coat’s disease signs?
Leukocoria
HUGE sign
If onset early enough → may have strabismus
Telangectasia (abnormal dilated capilaries)
"Lightbulb" telangiectasia
Multiple clumped lipid exudates
Simplest terms: Exudates are "leaky" debris from your blood
Specifically - composed of lipids (fats) and proteins that have escaped from damaged/abnormal blood vessels
Exudative retinal detachments also possible
Advanced cases may have: Glaucoma + blind, painful eye


Coat’s Signs Staging:
Telangectasia only
Exudates
Exudative RD
Glaucoma
End-stage disease
Coat’s disease tx?
***Retinoblastoma MUST BE RULED OUT BEFORE ANY TX
Control leaky blood vessels:
Laser photocoagulation
Cryotherapy (tissue freezing)
Glaucoma:
Tx if present
Retinoblastoma?
MOST common primary intraocular malignancy (cancer that develops inside eye) in kids
Diagnosis: usually before age of 5 yrs
Basophilic cells
Retinoblastoma symptoms?
Parents see Leukocoria!!!! (white pupil)
Possible strabmisus
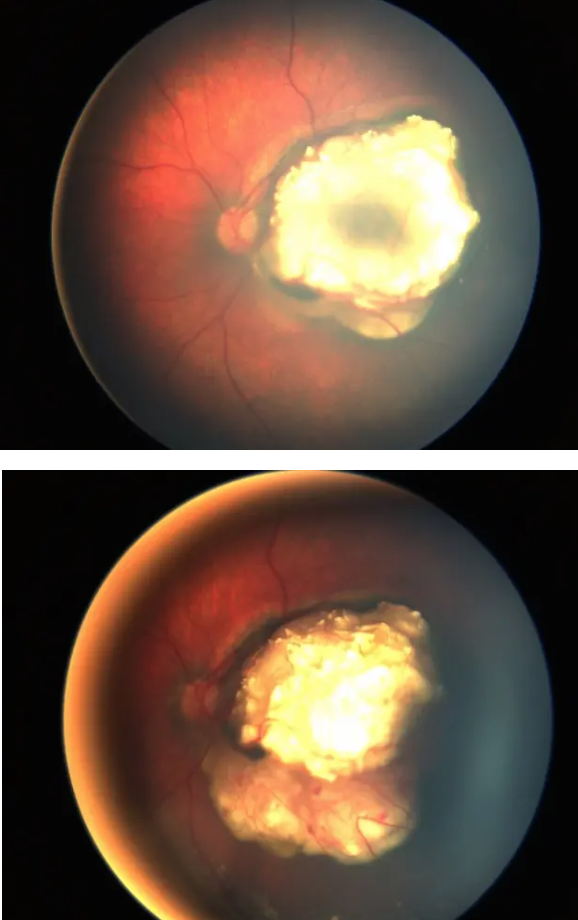
Retinoblastoma signs?
Tumor
Unilateral
Dome-shaped yellow-white globular mass w/calcification
Reduced VA, recurrent uveitis from uvea invaded, psuedo-hypopyon
Looks like hypopyon (white layer in anterior chamber) BUT:
NOT inflammatory WBCs
Malignant cells/tumor cells settling
Secondary glaucoma w/bupthalmos (globe enlargement)
IF left untreated = tumor will spread to invade orbit + adjacent bony structures

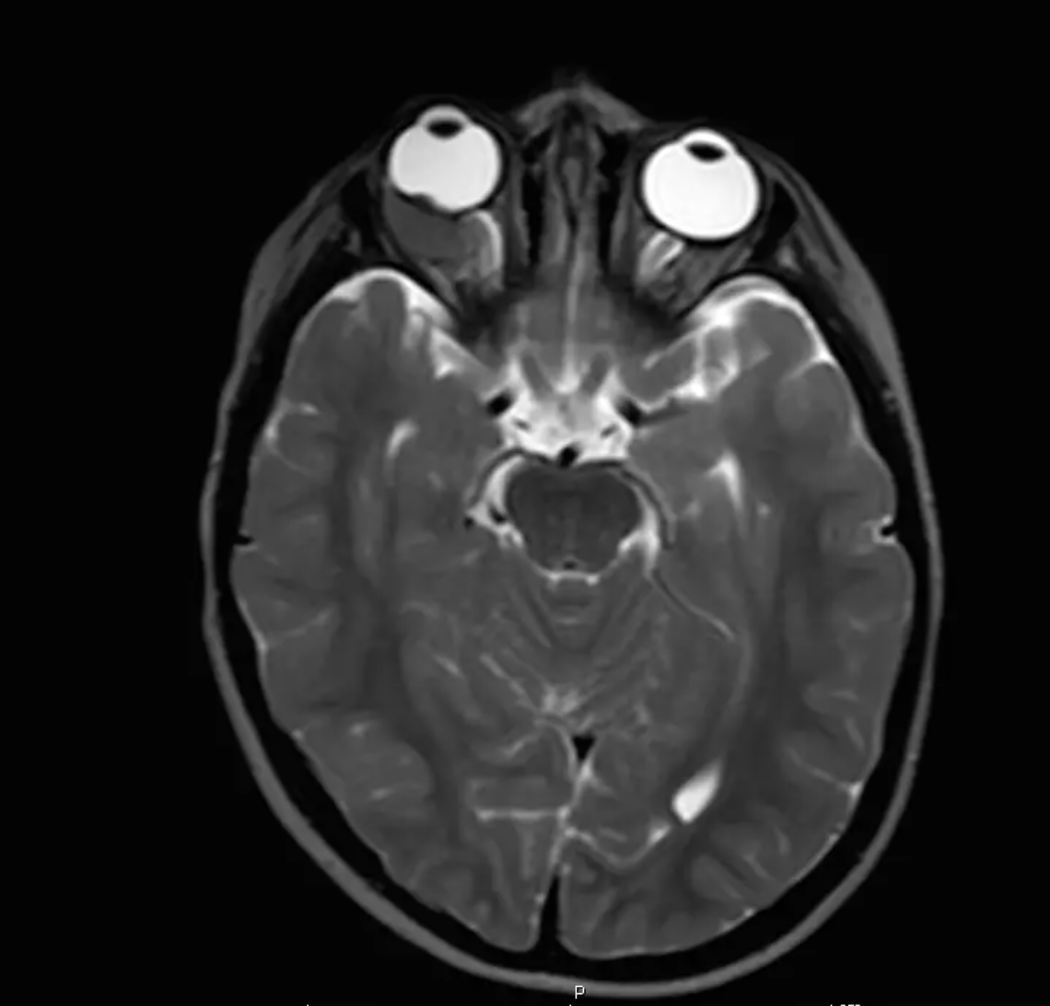
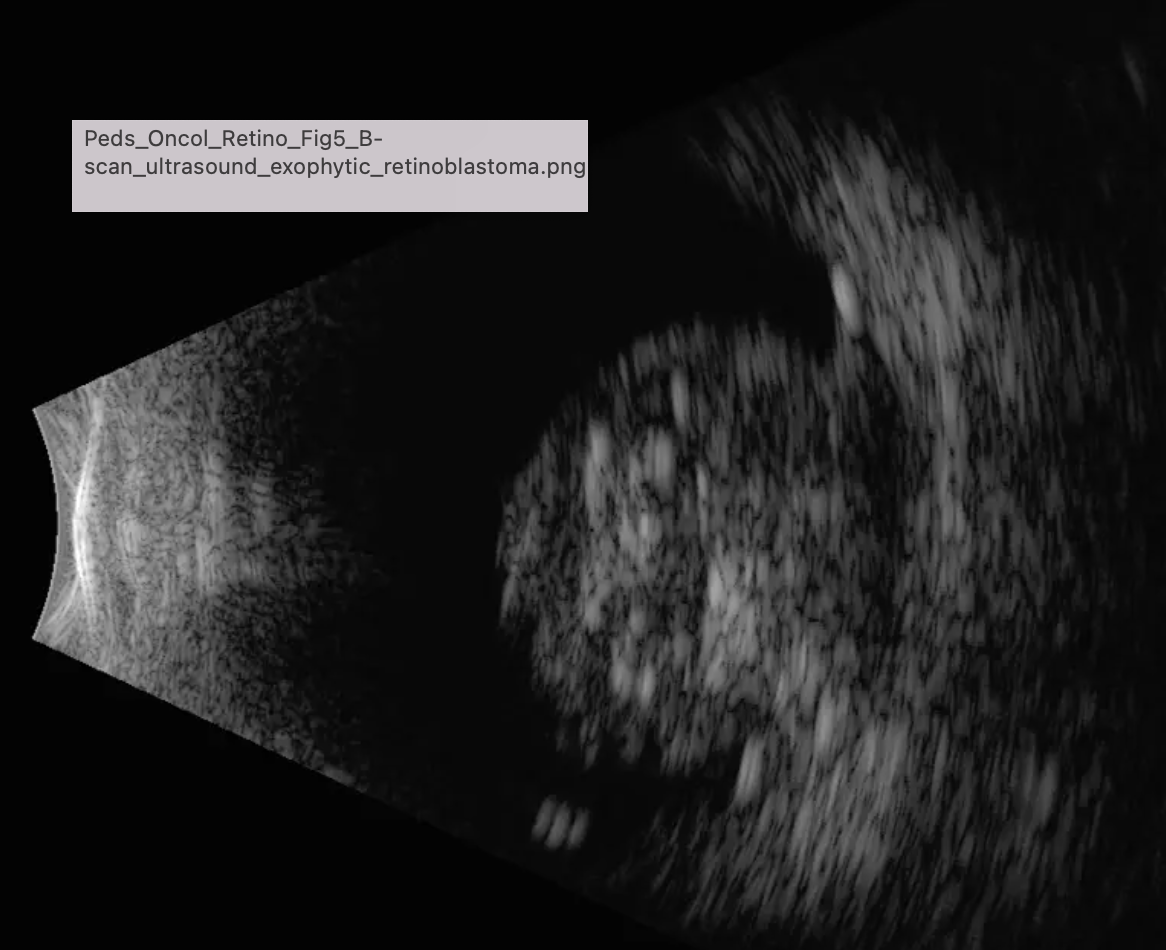
Retinoblastoma tx?
Confirm diagnosis w/exam under anesthesia:
B-scan
MRI
Tx:
Surgical: Enucleation most common (remove eyeball, leave EOMs + other orbital content intact)
VS. Exteneration = complete removal of globe + all eye socket contents
Chemotherapy
Good prognosis; 90% survival rate
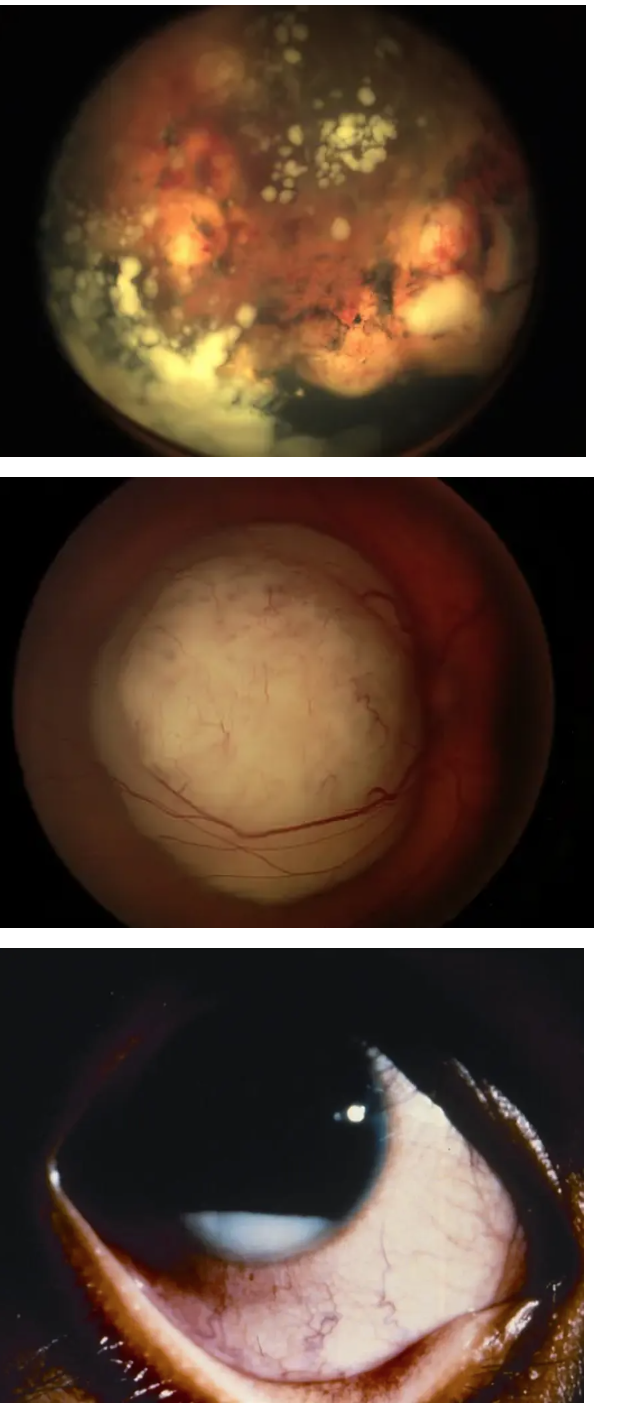
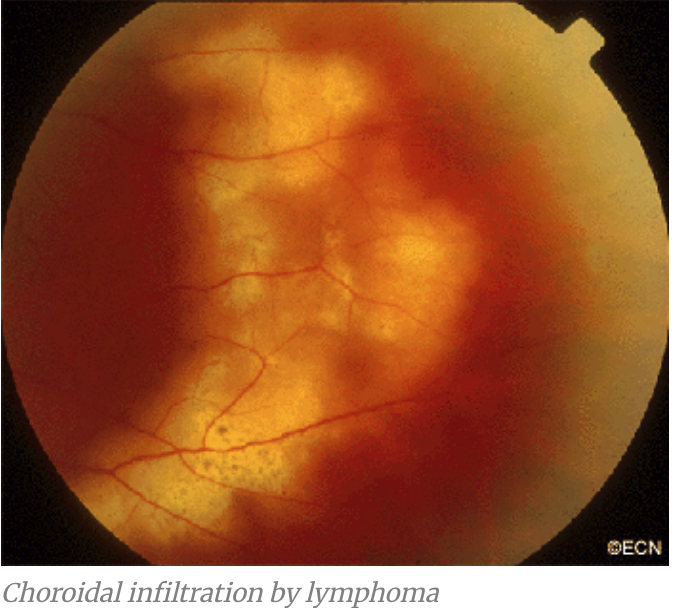
Primary Ocular Lymphoma (Primary CNS Lymphoma)?
Initially begins in brain!
Optic nerve is extension of the brain → so this tumor can manifest in eye also
MOST PATIENTS will DIE wthin 2 yrs diagnosis
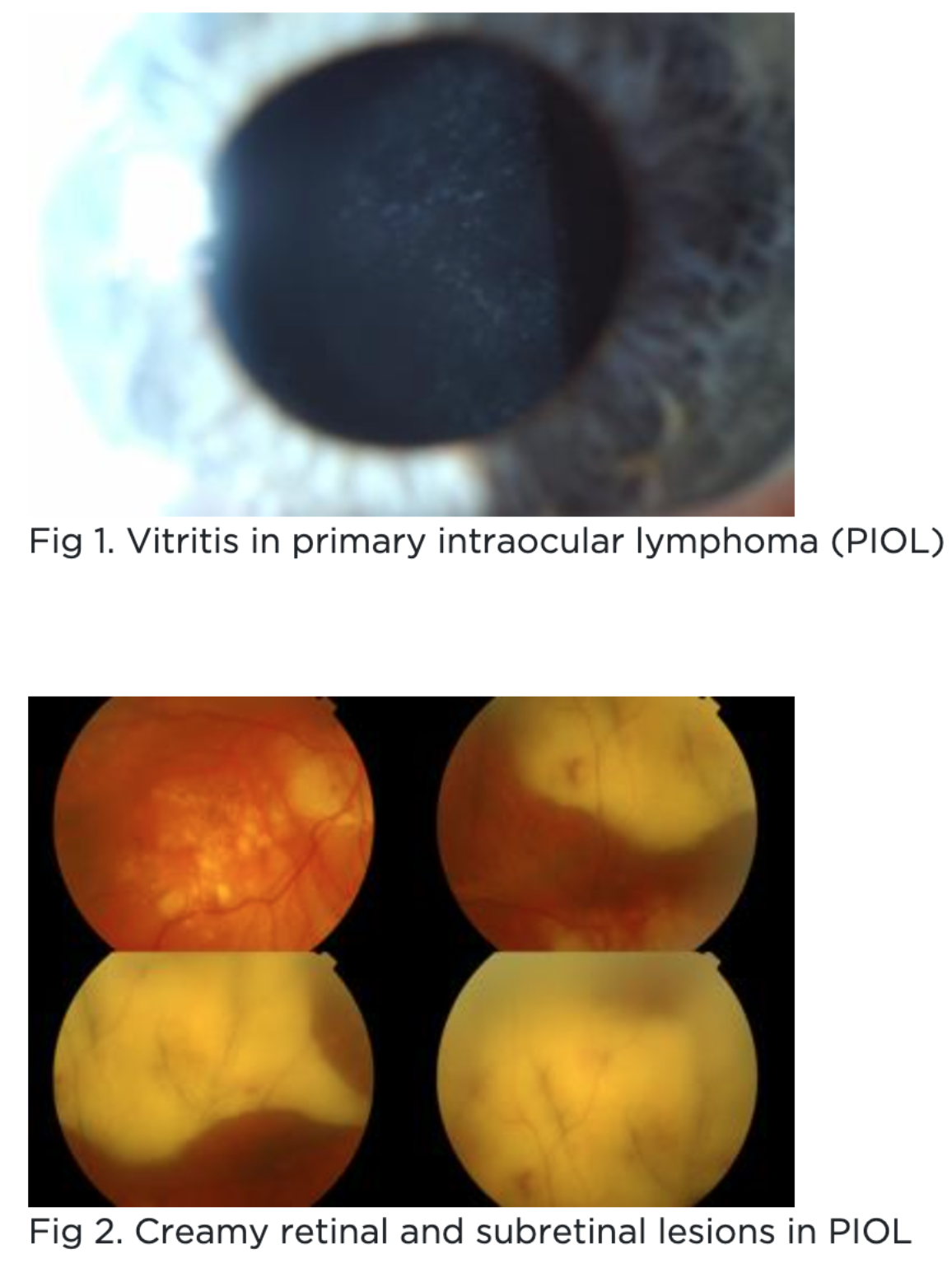
Primary Ocular Lymphoma (Primary CNS Lymphoma) symptoms?
Blurry vision
Floaters
NO inflammatory issues (pain/redness/photophobia)
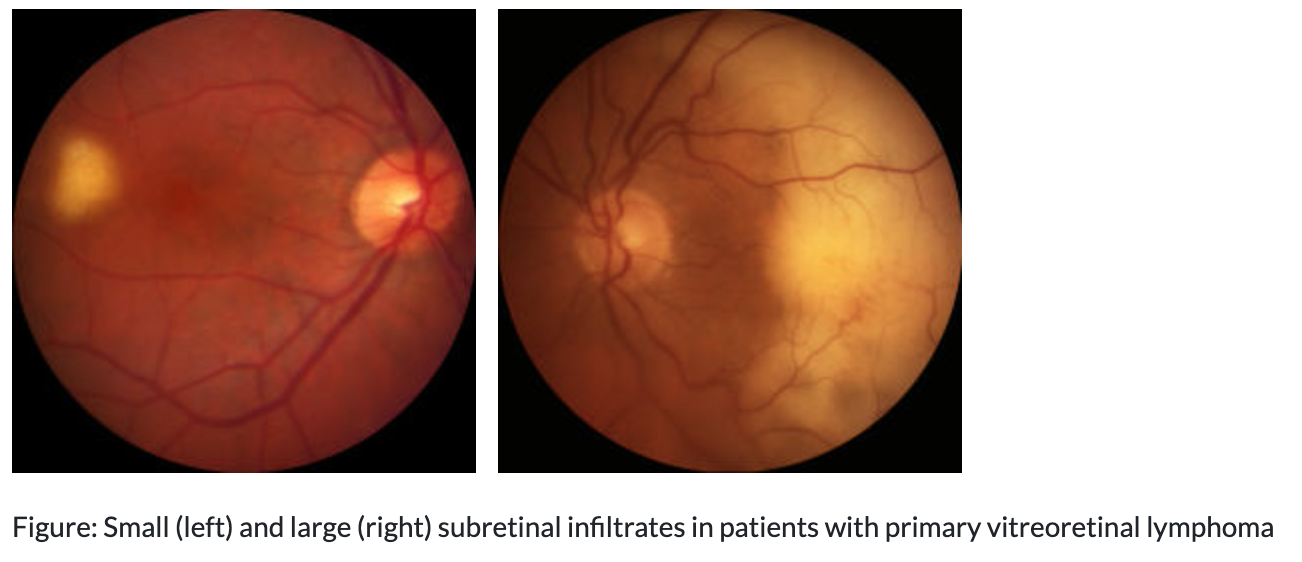
Primary Ocular Lymphoma (Primary CNS Lymphoma) signs?
Vitreous cells
Subretinal + Sub-RPE lesions
Primary Ocular Lymphoma (Primary CNS Lymphoma) tx?
(+) Biopsy of vitreous - to confirm before any start of tx
Systemic workup with oncologist evaluation:
MRI brain
Lumbar puncture
Bone marrow biopsy
Then:
Systemic chemotherapy + radiation
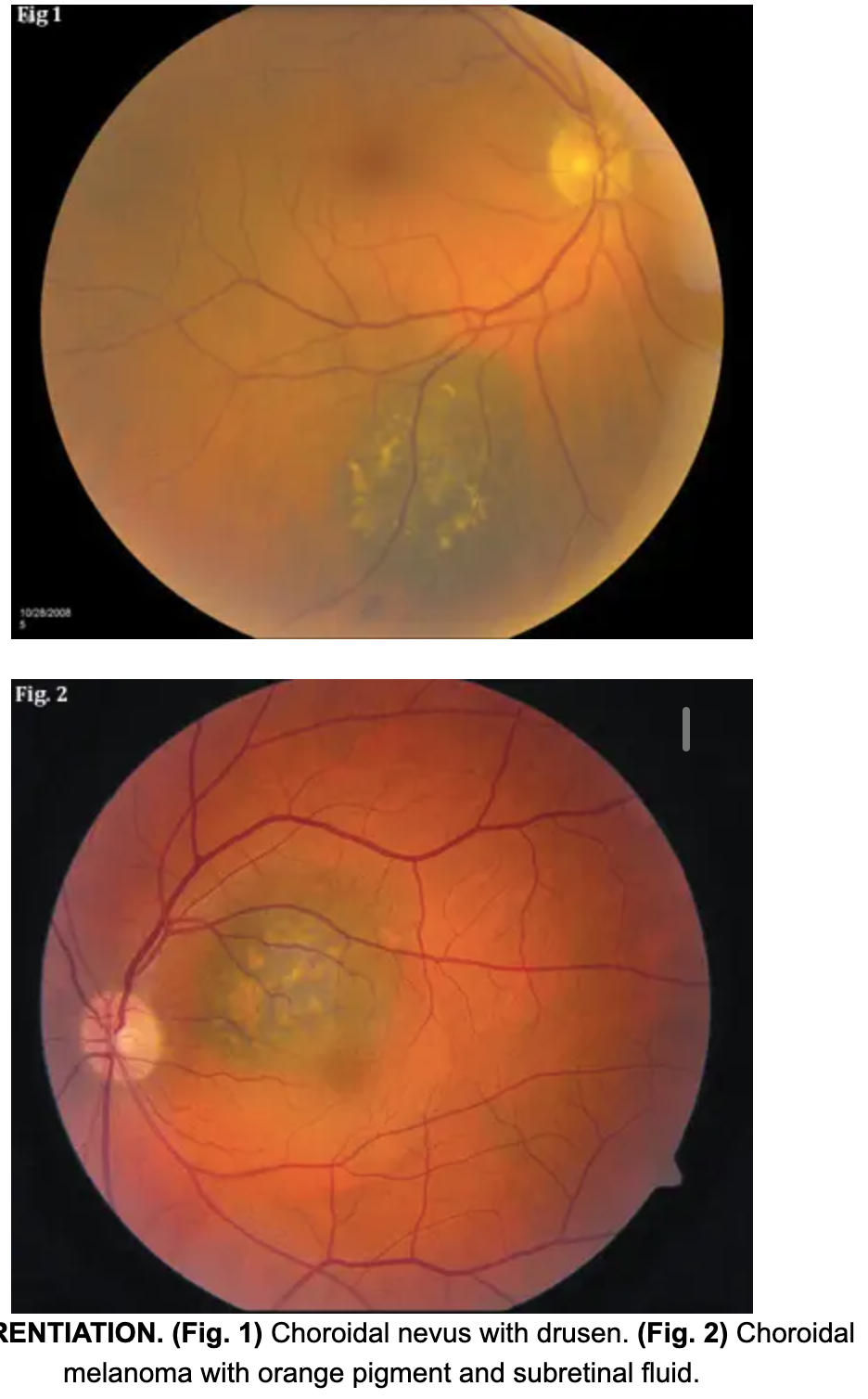
Choroidal melanoma?
MOST common primary intraocular malignancy (cancer that develops inside eye) in ADULTS
Associated with metastasis - most common sites:
FIRST + most common site = LIVER
Then lungs, bone, skin, CNS
Choroidal melanoma symptoms?
Asymptomatic IF located in periphery
Otherwise - blurry vision, metamorphopsia, VF loss, floaters, photopsia (flashes of light)
Choroidal melanoma signs?
Dome shape elevations:
May/may not be pigmented
Overlying yellow/orange lipofuscin
Indistinct borders
Serous/exudative retinal detachment
Tumors most likely to metastasis (spread):
Increased thickness
Involve ciliary body
CLOSE proximaty to nerve
Show growth
Risk Factors: "To Find Small Ocular Melanoma" (TFSOM)
If a lesion has 3 or more of these, there is a 50% chance it is a melanoma.
T - Thickness: Greater than 2 mm.
F - Fluid: Subretinal fluid (serous detachment).
S - Symptoms: Flashes, floaters, or blurred vision.
O - Orange Pigment: Lipofuscin sitting on the surface (this is a huge red flag).
M - Margin: The lesion is touching or within 3 mm of the Optic Disc.

Choroidal melanoma tx?
Oncologist for systemic evaluation
Plaque brachytherapy
Proton beam therapy
Enucleation to prevent metastasis
COMs study
No diff in 5 yr mortality rate for people tx with brachytherapy or enucleation in medium-large sized melanomas
THUS: we usually try to save eye with radiation
Radiation therapy BEFORE enucleation doesn’t improve survival rates
Choroidal metastasis?
Secondary Malignancy!
Most common intraocular malignancy in adults
Cancer started somewhere else (like Breast or Lung) and traveled through the blood to eye
***Most common sites of PRIMARY tumor = women (breast) and men (lung)
Choroidal metastasis prognosis?
Poor ☹
Most people die within 1 yr of diagnosis
Choroidal metastasis signs?
Yellow-white elevated lesions with pigmented clumps + possible overlying serous/exudative RD
Vitreous is usually crystal clear (unlike Primary ocular lymphoma which is 2 yr survival rate)



Choroidal metastasis tx?
Tx underlying cancer with oncologist + chemotherapy
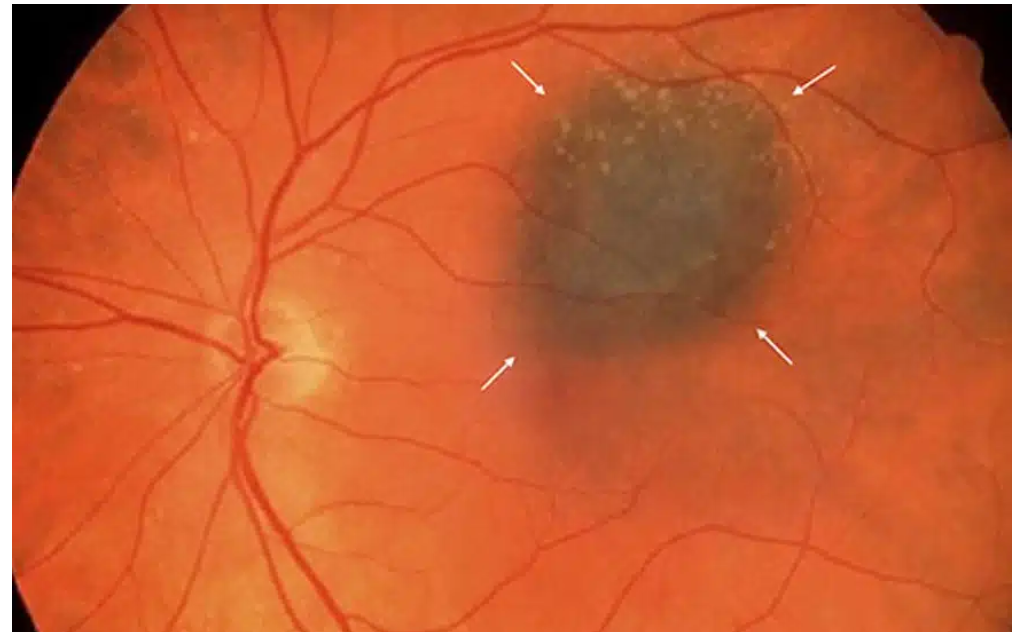
Choroidal nevus?
Typically benign!
Similar to freckles
Disappears with Red-free filter (Green one)
Not visible with Green (Red-free) filter = NOT in RPE but instead in choroid
VS. CHRPE → IS visible with Green (Red-free) filter = in RPE
Choroidal nevus symptoms?
Asymptomatic
Choroidal nevus signs?
Flat, grey-brown spot ANYWHERE in retina
WELL-demarcated borders
***Very small fraction of choroidal nevi CAN grow into choroidal melanomas
Higher risk nevi:
Having symptoms (flashes, floaters, blur, etc.)
Close to optic nerve (recall: within 3mm DD)
Change/growth
Elevation
Overlying orange pigment (lipofuscin)
Subretinal fluid
Choroidal nevus tx?
Document + monitor with FUNDUS photography!
Follow up in 3 months first
Then 1-12 months after depending on risk level
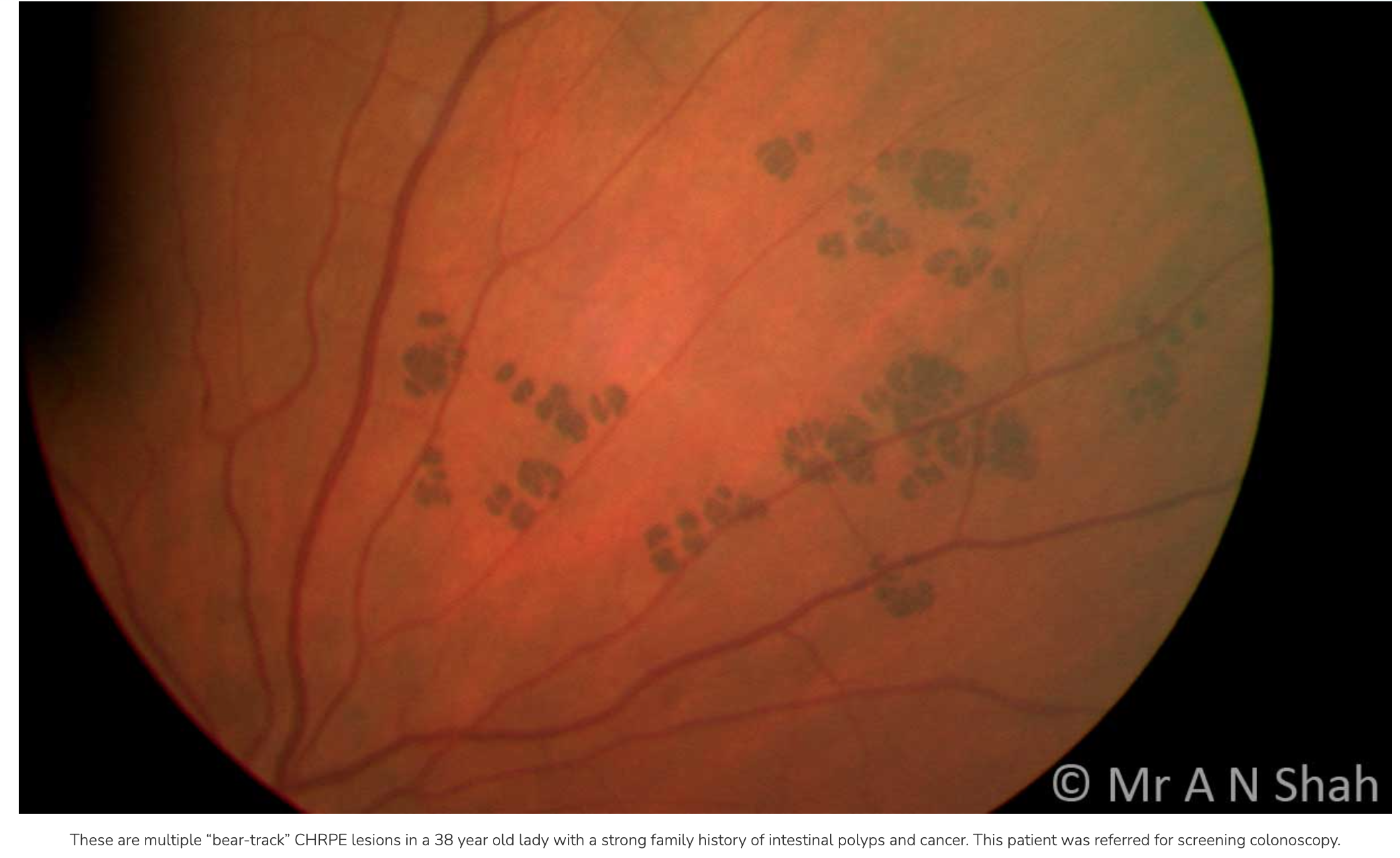
Congenital hypertrophy of retinal pigment epithelium? (CHRPE)
Congenital hypertrophy
THUS: true CHRPE present at birth
WILL NOT disappear with red-free (green) filter - will still be visible!!!
THUS: located in RPE
CHRPE symptoms?
Asymptomatic
CHRPE signs?
Singular, flat brown “freckle”
Not disappearing w/red-free (green) filter

If bilateral, multiple, small CHRPE’s = “bear tracks” (also benign)
VS. FAP lesions (familial adenomatous polyposis aka Gardner’s syndrome) = more ovoid with comet shape (also bilateral + multiple)
CHRPE tx?
1 solitary CHRPE
Monitor + photograph for documentation
Any lesions that look like FAP
Refer for COLONOSCOPY
Gardener’s Syndrome/FAP (genetic) typically diagnosed in 20s → will lead to colon cancer by 50s
Ocular looks like: multiple, bilateral CHRPEs
Systemically: colon polyps, soft tissue tumors (neurofibromas, cysts), skeletal hamartomas
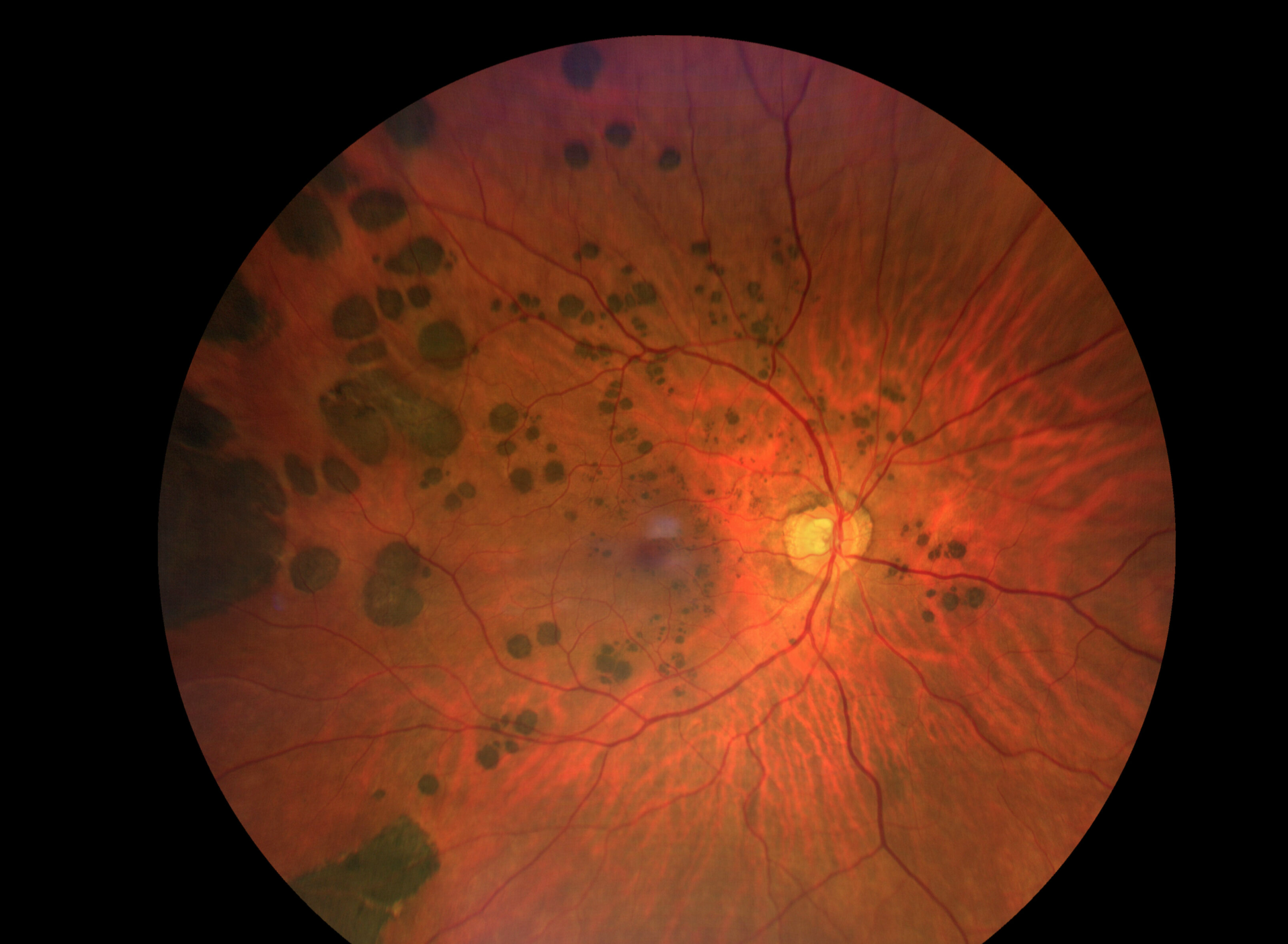
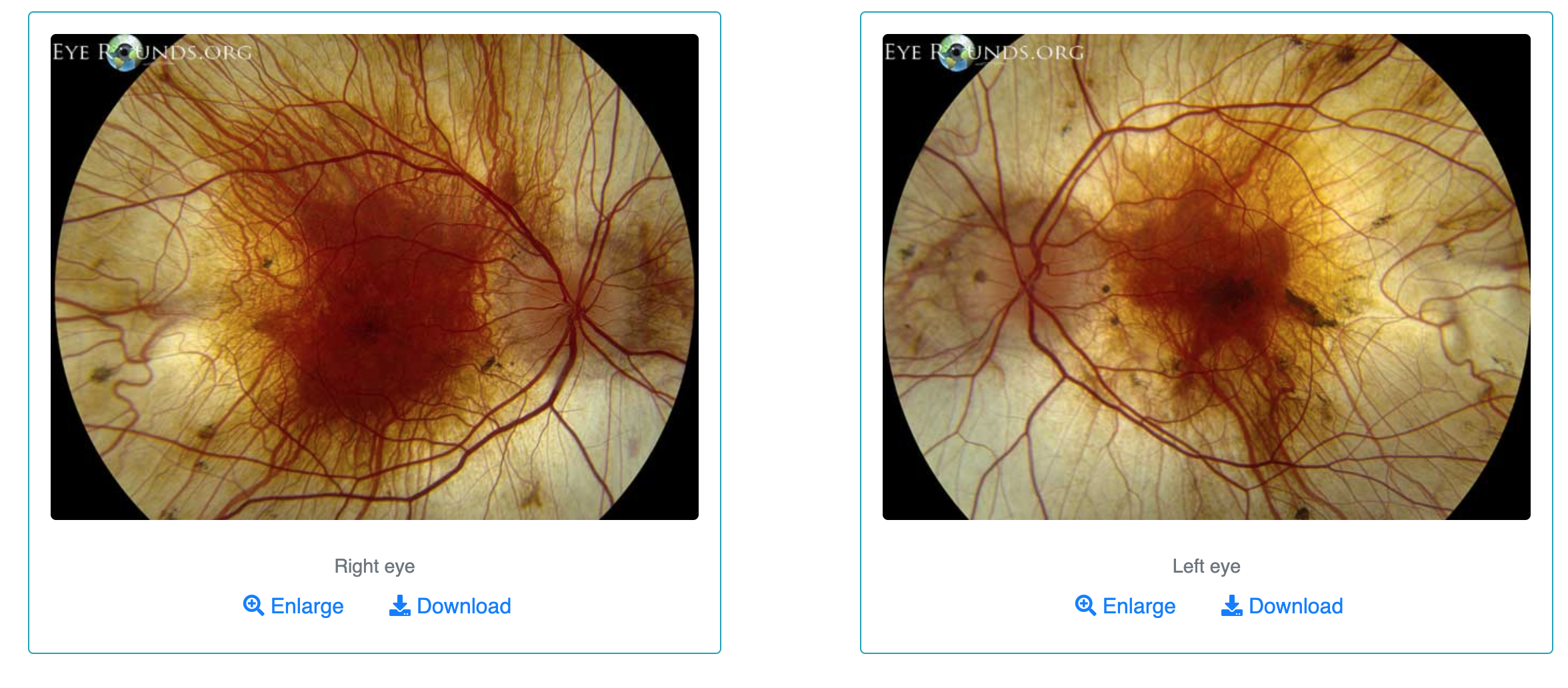
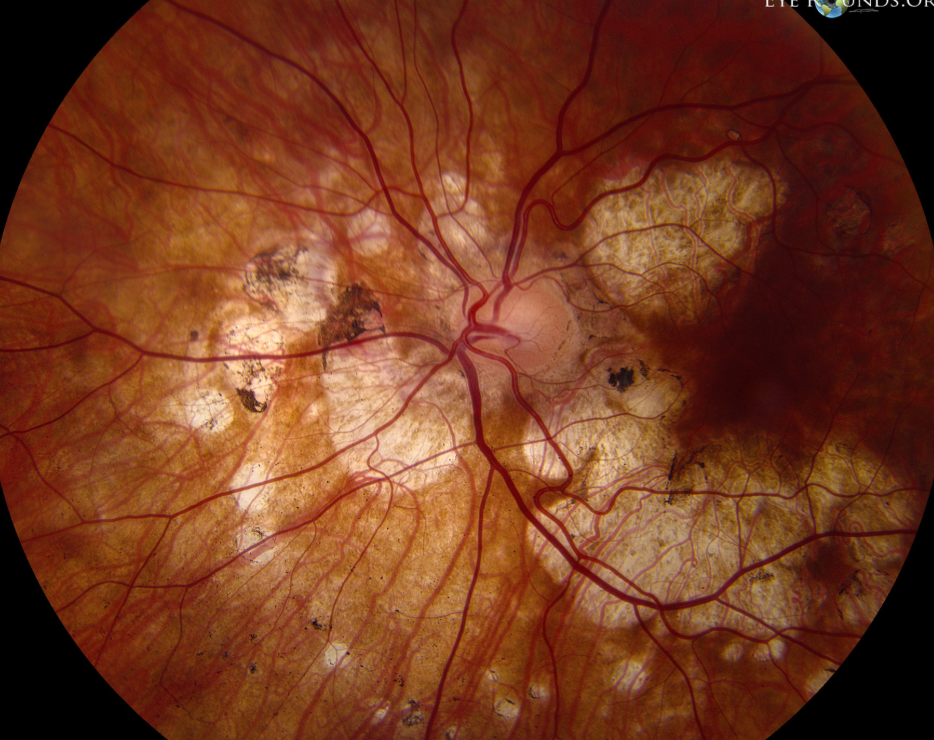
Choroideremia?
X-linked recessive inheritance (genetic)
MEN affected but WOMEN are carriers
Men age 20-30 yrs → progresses to legal blindness by age 50-60 yrs
Choroideremia symptoms?
Night blindness (nyctalopia)
Light sensitivity (photophobia)
Other causes of Night blindness (nyctalopia)?
Choroidemia ✔
Birdshot Chorioretinopathy ✔
Thioridazine Retinopathy
Retinitis Pigmentosa
Gyrate atrophy (progressive myopia) ✔
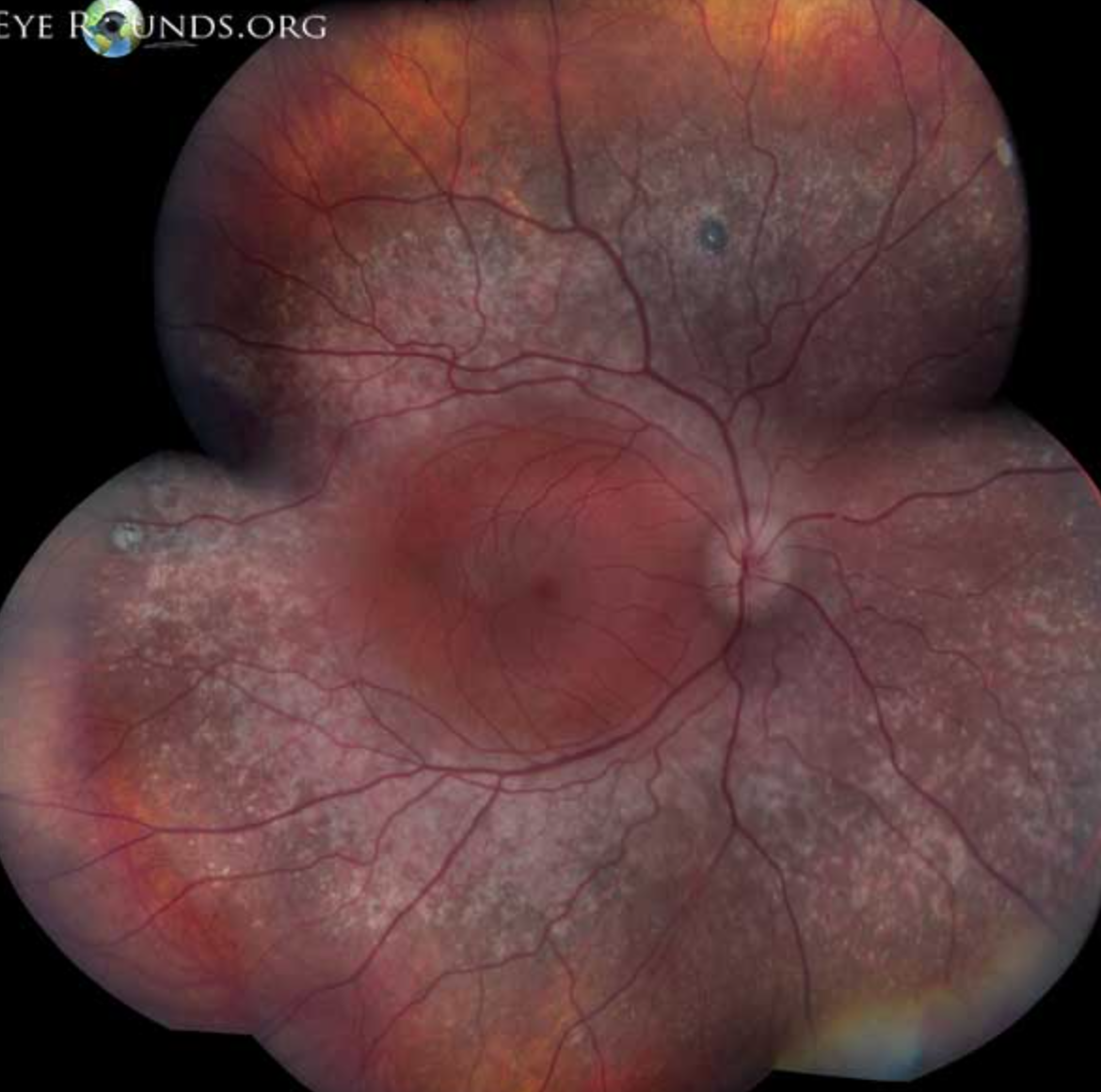
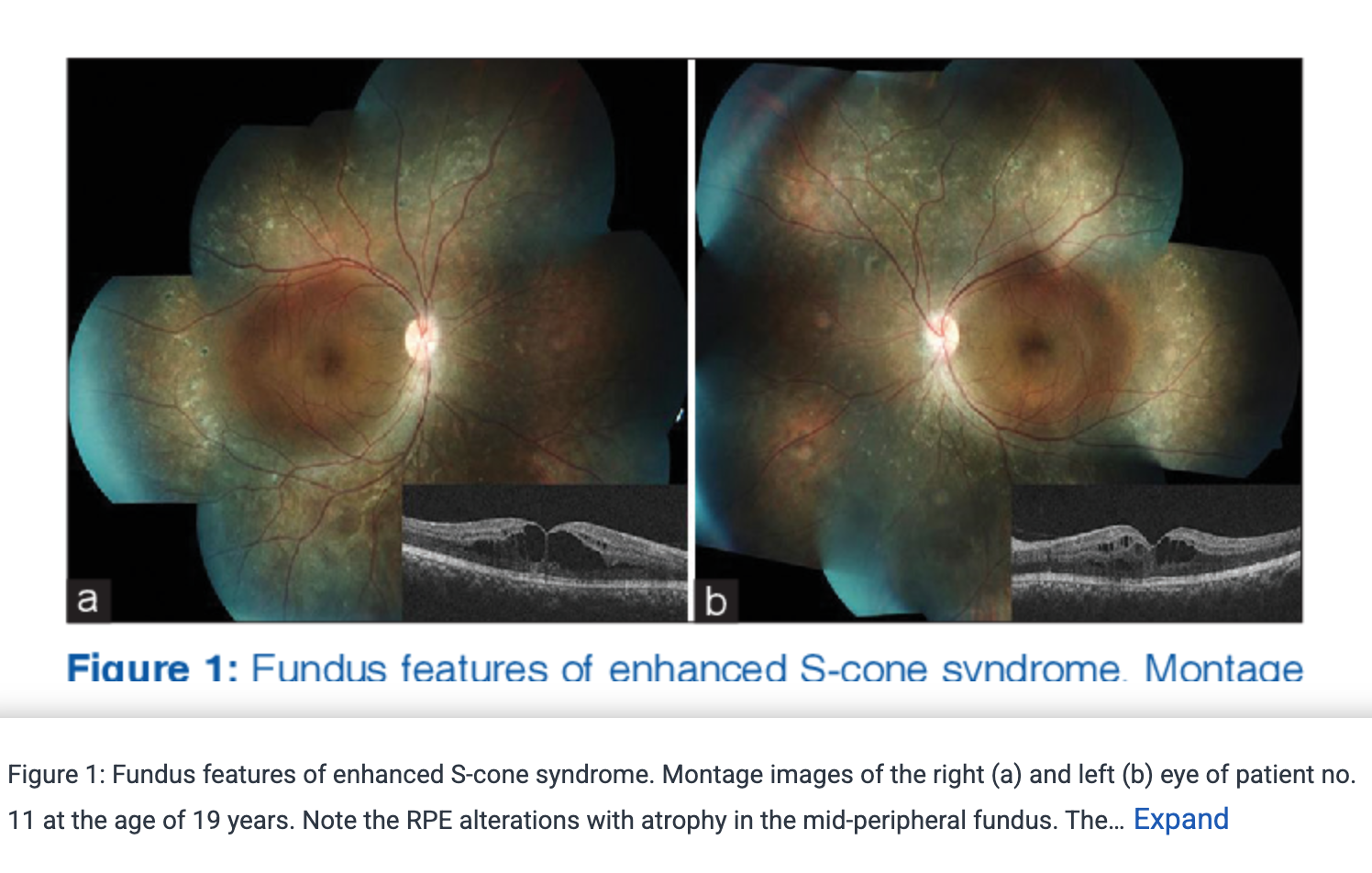
Enhanced S-cone Syndrome/Goldmann-Favre Syndrome
Choroideremia signs?
Peripheral atrophy of choriocapillaries
Revealing underlying choroidal vessels
Progressive
Spares macula till late in disease
Choroideremia tx?
No treatment ☹
Low vision consult + genetic testing
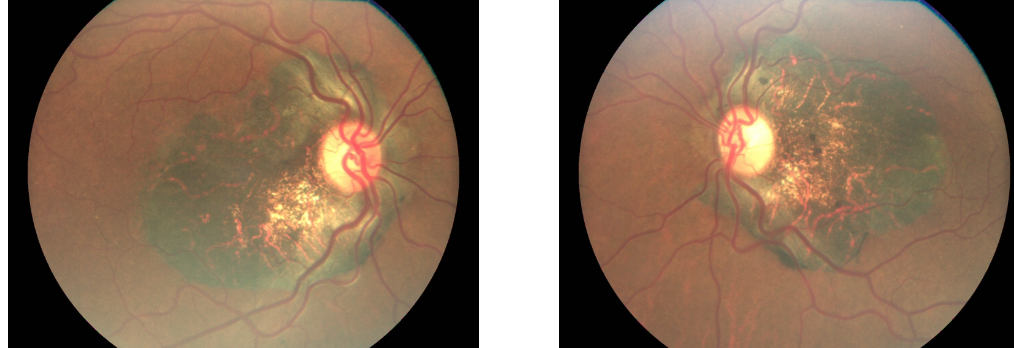
Central Areolar Choroidal Dystrophy?
Autosomal Dominant inheritance (genetic)
Starts 30-40 yrs → progresses to severe vision loss by age 60-70 yrs
Central Areolar Choroidal Dystrophy symptoms?
Blurry vision
Central scotoma
Central Areolar Choroidal Dystrophy signs?
Early stages:
Hypopigmentation of macula → progress to geographic atrophy with well-defined borders, slowly enlarging to reveal underlying choroidal vasculature
Decreasing vision from 20/25 → 20/200
Bilateral + symmetric
Almost looks like choroidermia inverted (now affecting macula first)
Central Areolar Choroidal Dystrophy tx?
No treatment ☹
Low vision consult + genetic testing
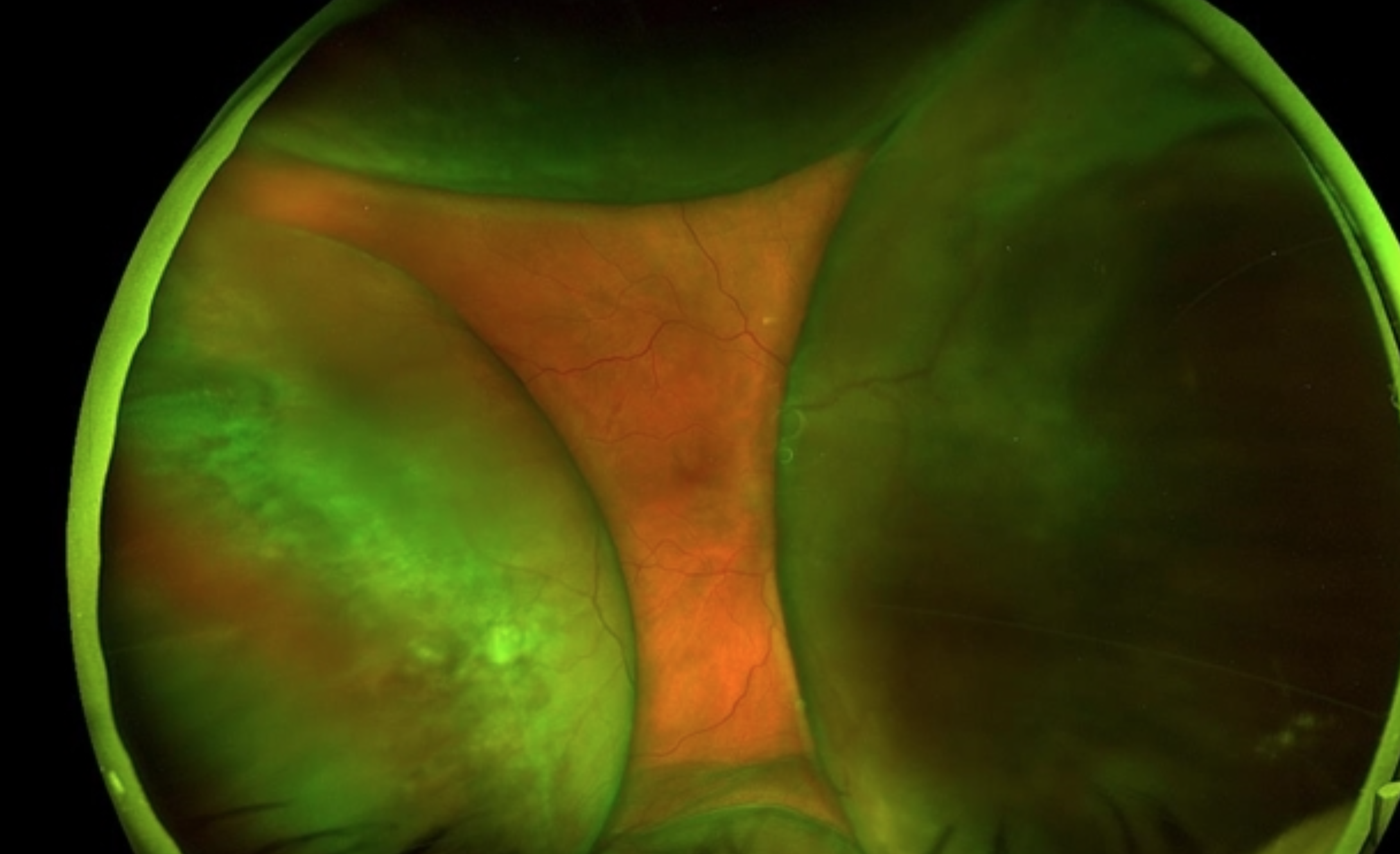
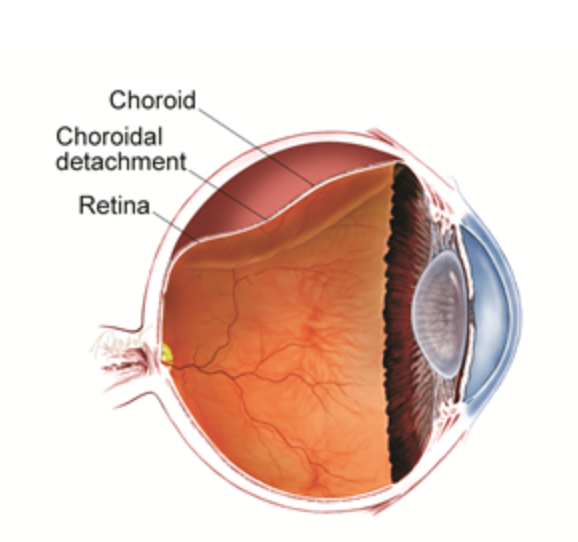
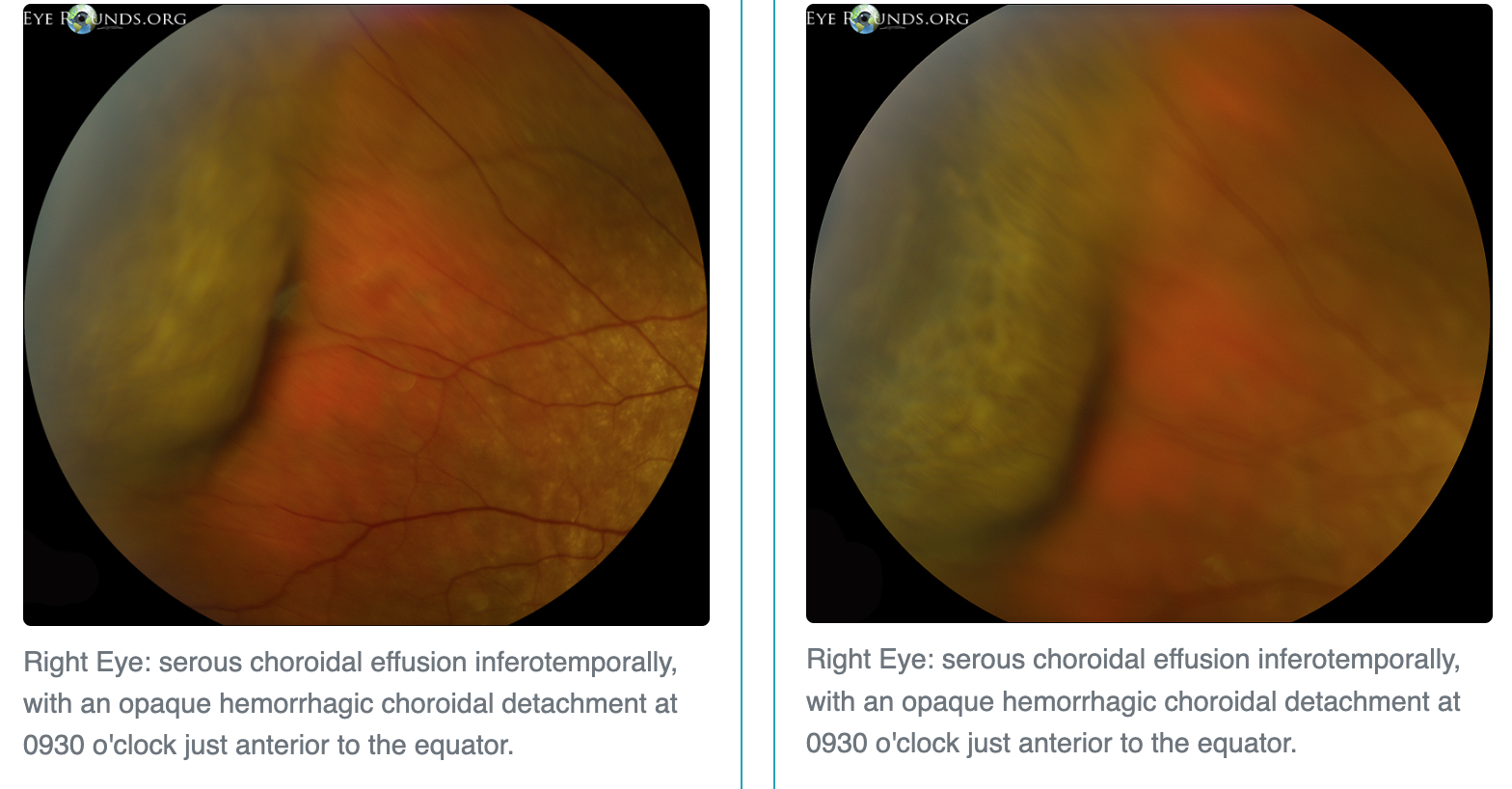
Choroidal Detachment?
Choroid separated from sclera
Looks like a thick, smooth, brown, dome-shaped elevation (VS. RD =
Bullous orange-brown peripheral elevation
2 types! BOTH look same on DFE!!
Serous
Hemorraghic
RD vs CD (detachments)?
Think RD if: "Flashes and floaters," "High myope," "History of lattice degeneration," or "Recent trauma"
Think CD if: "Recent Glaucoma Surgery," "Low IOP (Hypotony)" or "Inflammatory disease"
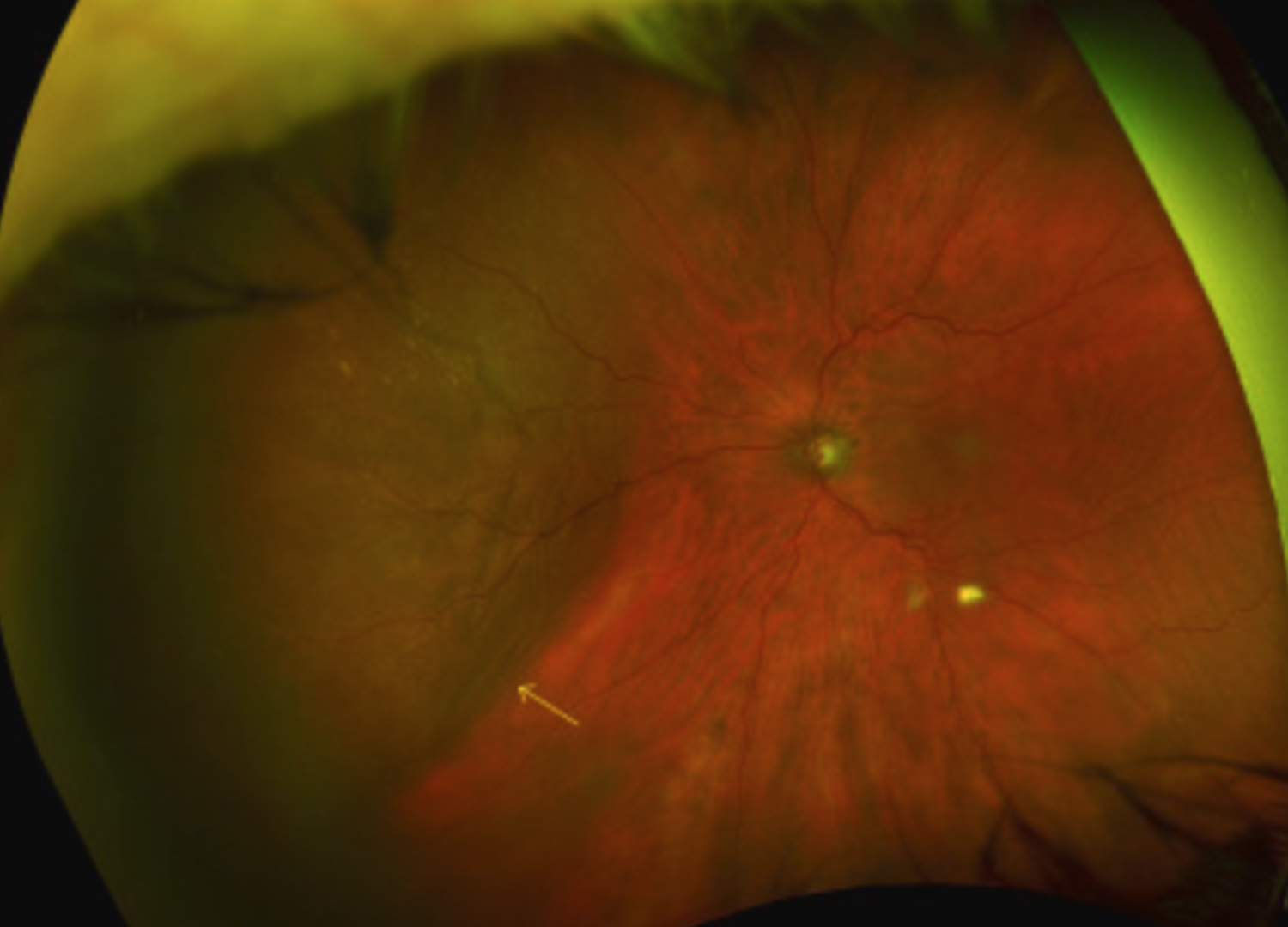
Serous Choroidal Detachment (Choroidal Effusion)?
LOW IOP (hypotony) secondary to puncture wound to globe
Or after glaucoma surgery like a trabeculectomy
WILL transilluminate
Placing bright light (transilluminator) against sclera + looking through pupil to see if light shines through mass

Symptoms?
Asymptomatic if peripheral or mild
Severe vision loss if severe (i.e. kissing)
Kissing Choroids: If detachment is massive, the two sides of choroid can actually touch in middle of vitreous
Tx?
Close wound
Prevent further IOP decrease
Bandage CL, Suture, Cyanoacrylate glue
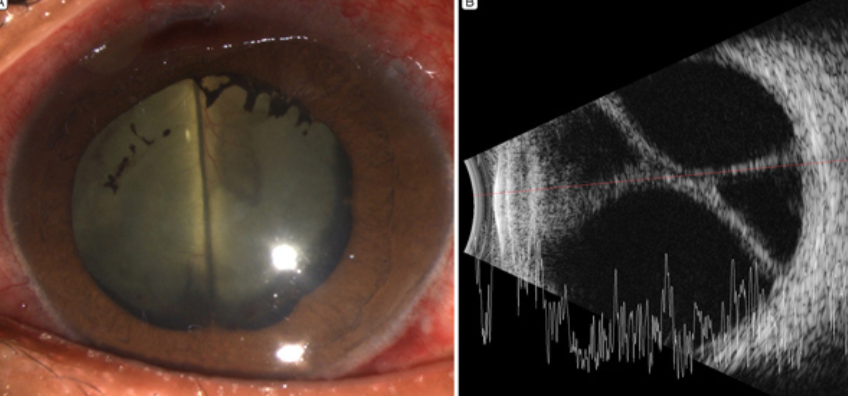
Hemorrhagic Choroidal Detachment?
HIGH IOP secondary to hemorrhaging during ANT SEG surgery
Blood pools between choroid + sclera (limited area in globe) → pressure increases → anterior chamber narrows as iris pushes forward
WILL NOT transilluminate
Symptoms?
SEVERE pain
RAPIDLY decreased vision
Red + inflammed eye
Tx?
Close wound to prevent further hemorrhaging
Cycloplegic to prevent synechiae
Sclerotomy (surgical scalera cutting) possibly - to allow blood drainage
Ocular hypotensives possibly - to reduce IOP
Any remaining choroid issues haven’t gone over yet?
Candidas (other flashcard set - sick/IV patients)
Serpinginous Choroidopathy (similar presentation to TB which is an infection, gran panuveitis, antibiotics, RICE)
Birdshot Chorioretinopathy (Granulomotous, white dot syndrome)
Serpinginous Choroidopathy?
Idiopathic
MEN - 50-60 yrs old
HLA-B7
ALSO think Presumed Ocular Histoplamosis!
***TB can cause similar fundus appearance - RULE OUT***
Serpinginous Choroidopathy symptoms?
Central blurry vision
Scotoma that may be unilateral or bilateral
Serpinginous Choroidopathy signs?
Recurrent disease
Lesions:
Begin at optic nerve
Extend in SERPENTINE manner towards macula
ACTIVE lesions = grey-white color
DORMANT lesions = atrophy + scar
CNVM = develops in 25% of cases

Serpinginous Choroidopathy tx?
Chronic + relapsing course
TX starts with steroids (oral or local) → transition to immunomodulating meds (steroid-sparing)
If CNVM - tx with Anti-VEGF
Birdshot Chorioretinopathy (Vitiliginous Chorioretinitis)?
White dot syndrome!
Bilateral, chronic chorio-retinal inflammatory disease
White females - 40-60 yrs
HLA-A29
Granulomatous Posterior Uveitis (***NO KPs/mutton fat/busacca)
Birdshot Chorioretinopathy symptoms?
Blur
Photopsia (flashes)
Nyctalopia (night blindness)
Birdshot Chorioretinopathy signs?
Multiple, creamy yellow-white spots in fundus periphery
SPARE macula
< or equal to = size of optic disc

May have Vitritis, Retinal vasculitis, Cystoid Macular Edema
Atrophy + choroidal depigmentation → advanced cases
Birdshot Chorioretinopathy tx?
TX starts with systemic steroids → transition to immunomodulating meds (steroid-sparing)
Periocular + IV steroids = for CME especially
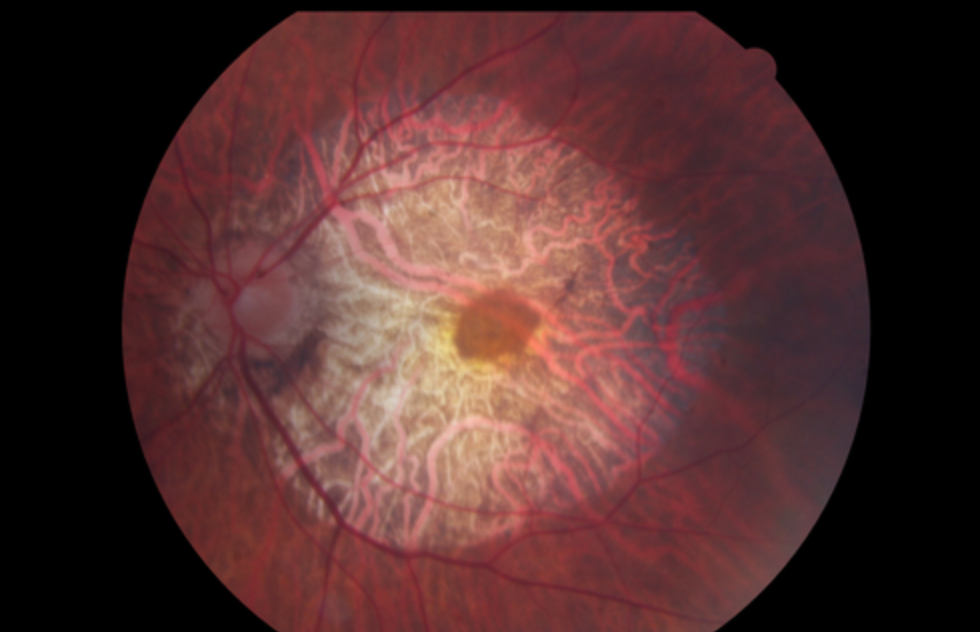
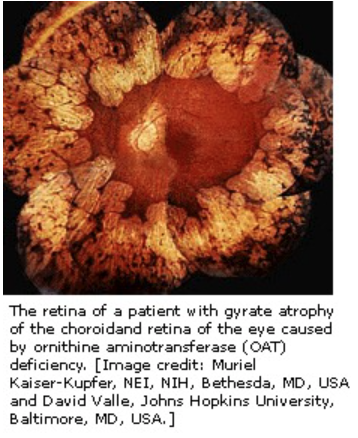
Gyrate Atrophy?
Autosomal Recessive
Genetic mutation of ornithine aminotransferase (OAT)
Causing urine + plasma ornithine levels increased: 10-20x greater than norm = toxic to RPE and Choroid
Onset → first 10 yrs of life
Afflicts entire retina between 40-50 yrs without treatment
Gyrate Atrophy symptoms?
Nyctalopia (night blindness)
Constricted visual field
Gyrate Atrophy signs?
Progressive myopia
Scalloped chorioretinal atrophy peripherally
Enlarge + migrate posteriorly
Effects macula last

Gyrate Atrophy tx?
Argine + Protein = make ornithine
THUS: we restrict these in diet to lower levels of ornithine
Also take Vitamin B6 supplement
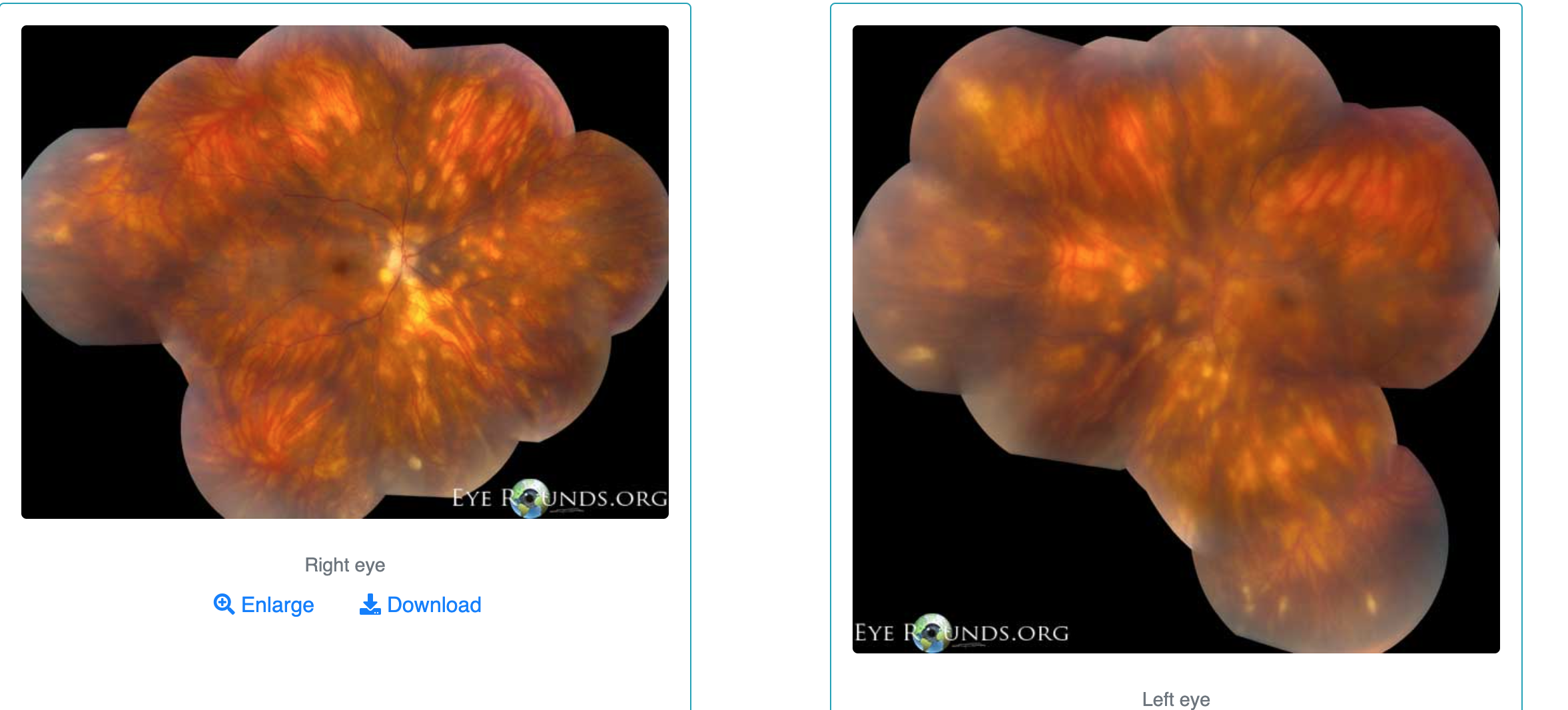
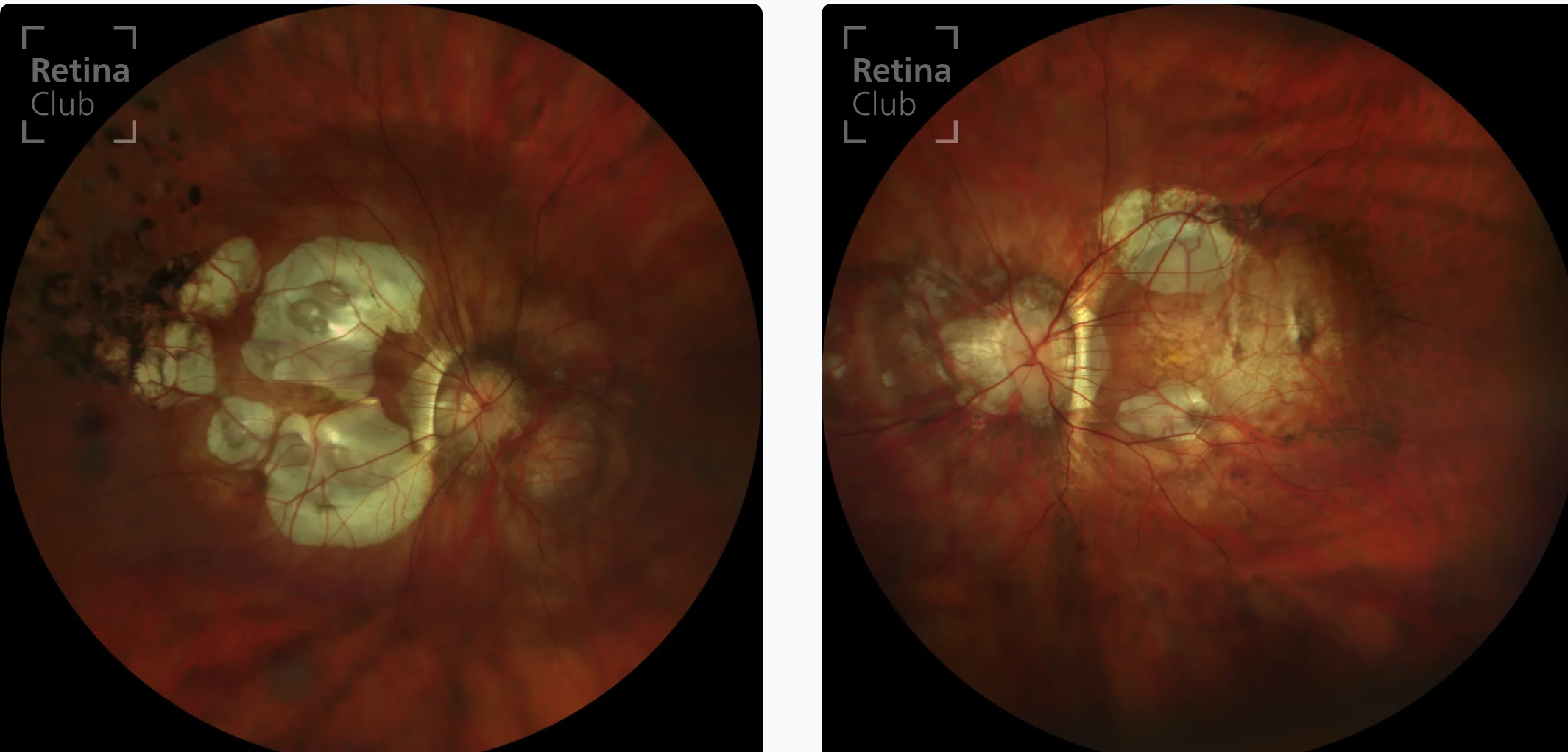
Pathological Myopia/Myopic Degeneration?
High grade + progressive myopia
Hereditary component
Eyeball will not stop elongating
Pts > -6.00D myopia or > 26mm axial length
***NOTE: NOT every high myopia patient has pathological myopia
JUST ones where myopia CONTINUES to progress + present certain signs
Pathological Myopia/Myopic Degeneration symptoms?
May complain decreased vision
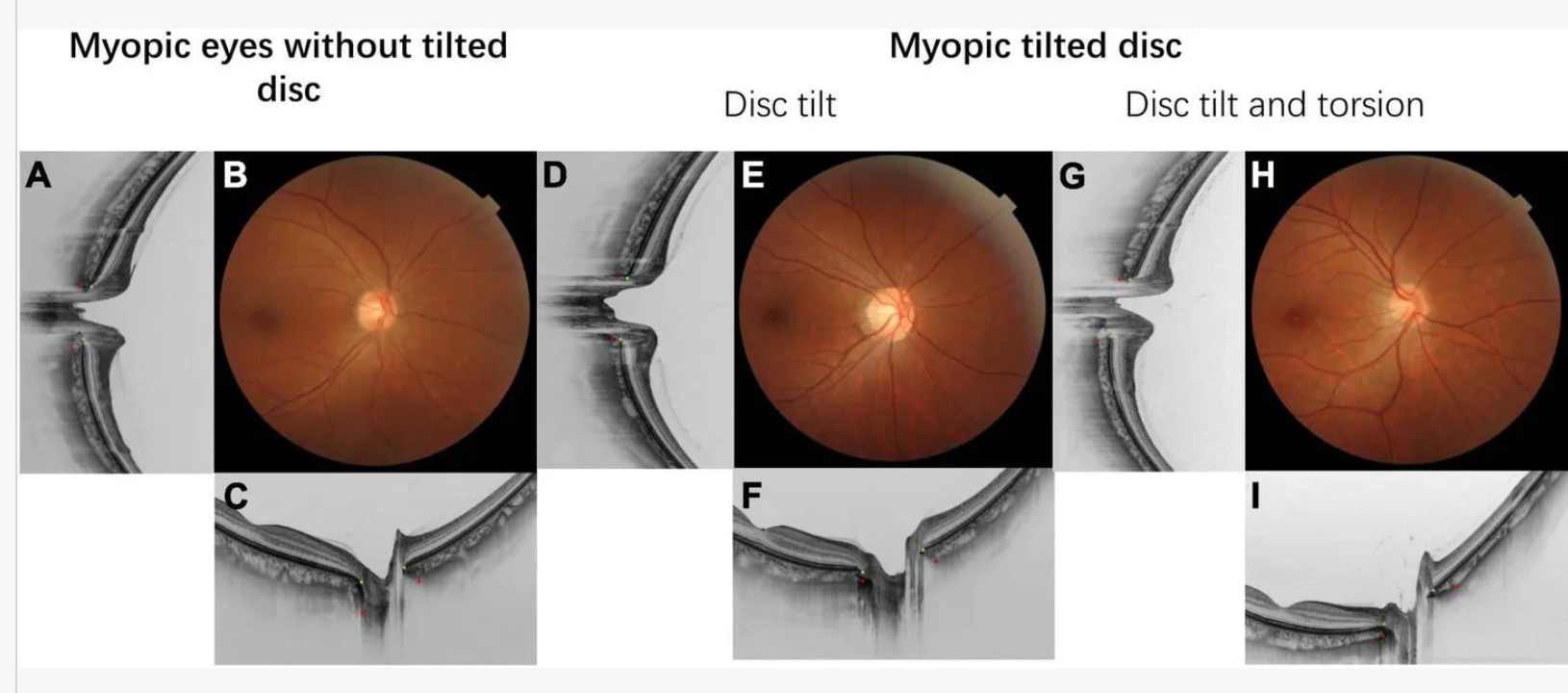
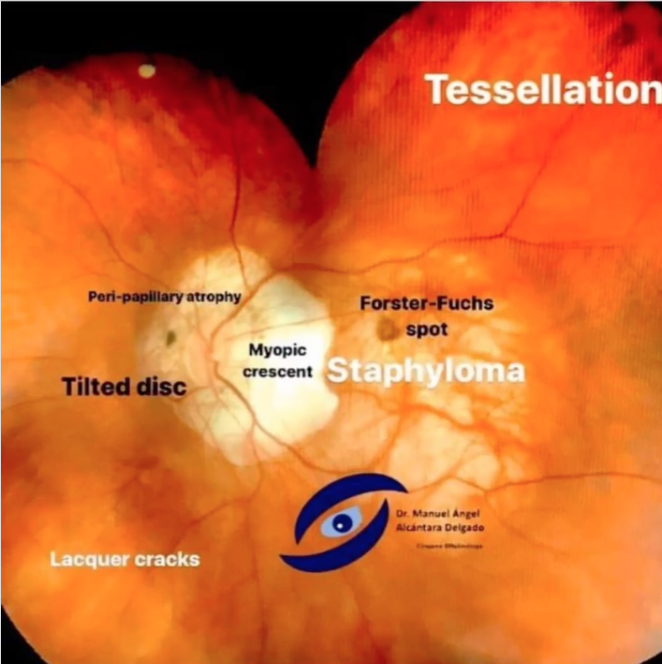
Pathological Myopia/Myopic Degeneration signs?
Tilted disc
Stretching makes optic nerve look "cupped" or pale → can mimic glaucoma even if IOP normal
PPA (RPE pulls away from the nerve)
Lacquer cracks
Mechanical breaks in Bruch's Membrane
Look like yellow-white "lightning bolts" radiating from nerve
Lacquer Cracks = "Mechanical Stretching" (Fine, irregular, yellow-white "lightning bolt" lines. Usually found in Macula or radiating from Optic Nerve) VS. Angioid Streaks = "Chemical Brittleness" (Thicker, darker, "vessel-like" streaks radiating from Optic Nerve)
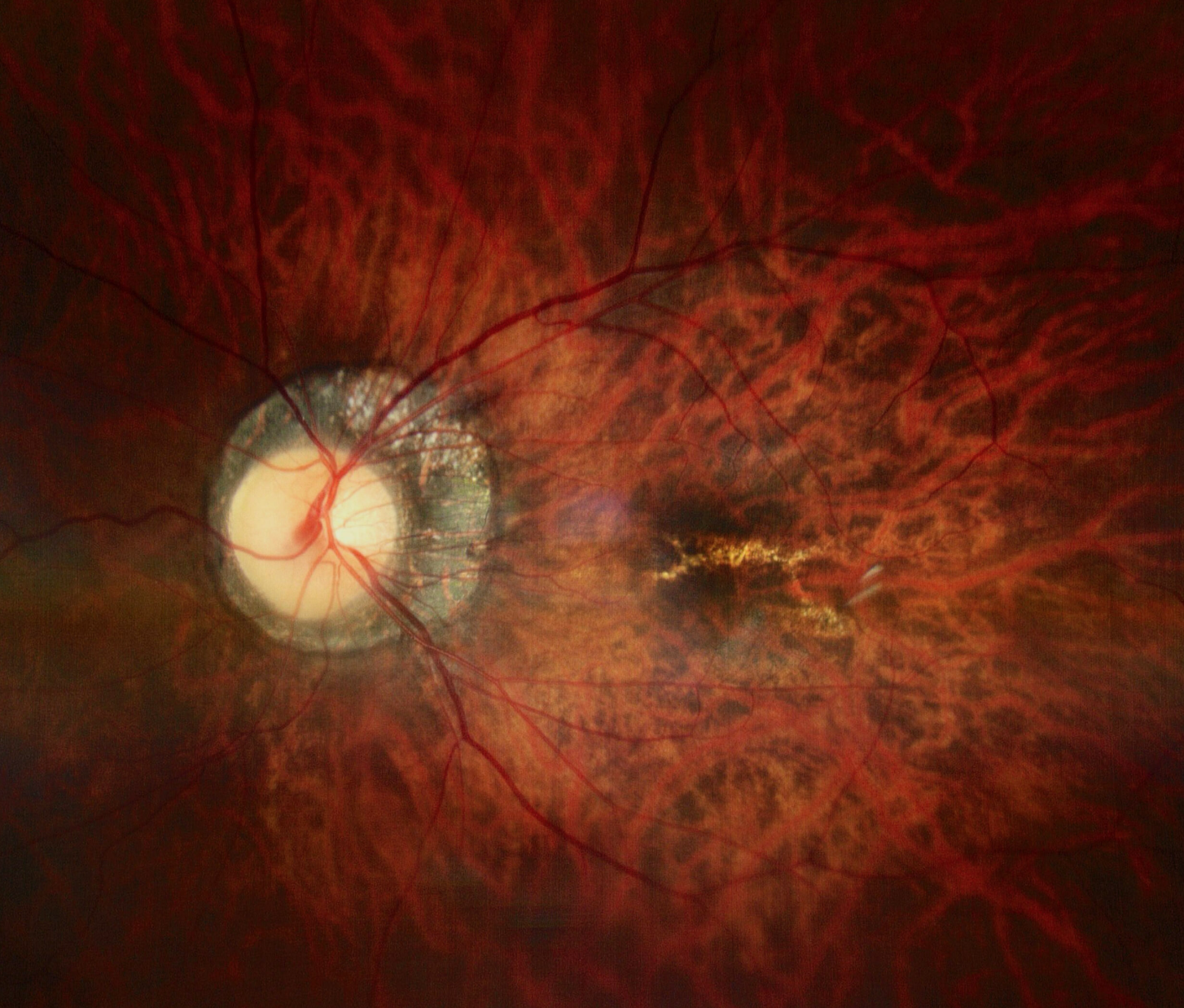
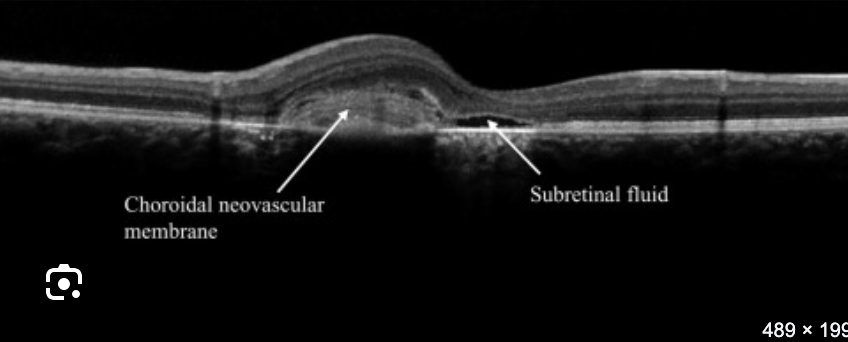
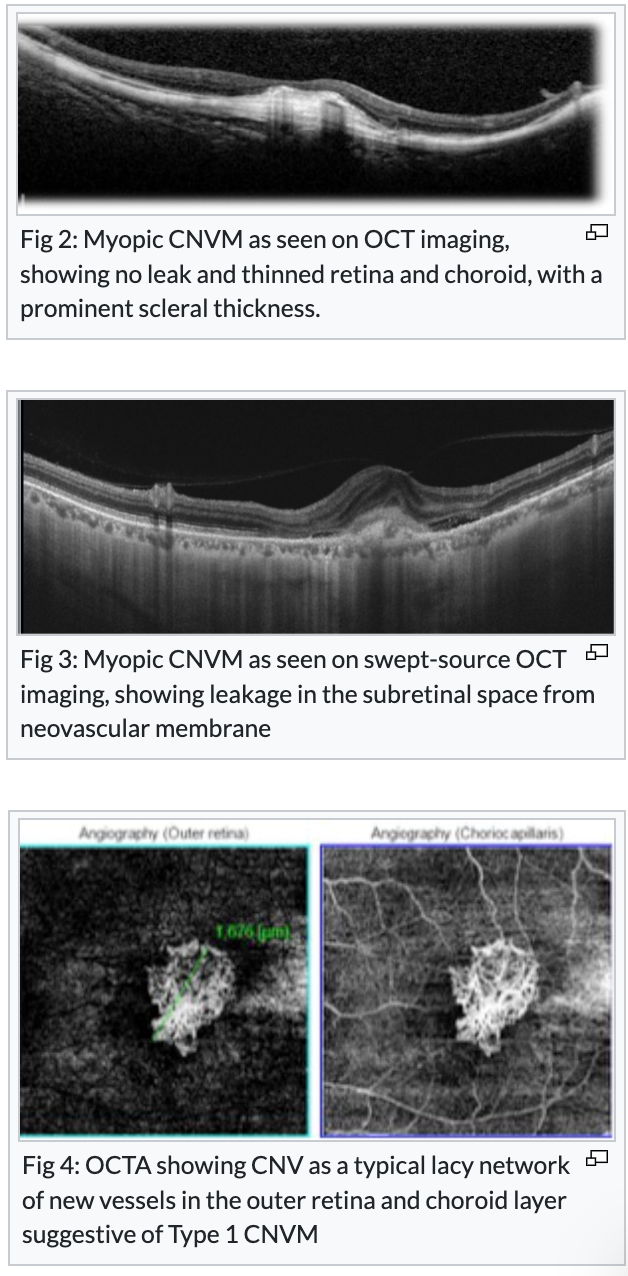
CNVM
While lacquer crack is a physical break in Bruch's Membrane - (think of Bruch's as "fence" keeping choroidal blood vessels out of retina) → once the fence "cracks" from stretching, the vessels can keep growing through gap then leak
New, fragile, "garbage" blood vessels
Start in Choroid (layer under retina) → Break: Grow upward through a break in Bruch’s Membrane (the "fence") → Leak: Because these new vessels are poorly built, they leak fluid (edema), lipids (exudates), and blood (hemorrhage) into subretinal space
Look: Small, grayish-green "tuft" or a small red subretinal hemorrhage
Symptom: Metamorphopsia (wavy lines) or new scotoma (blind spot)
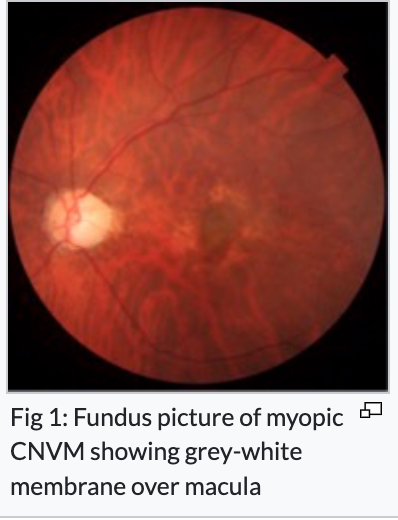
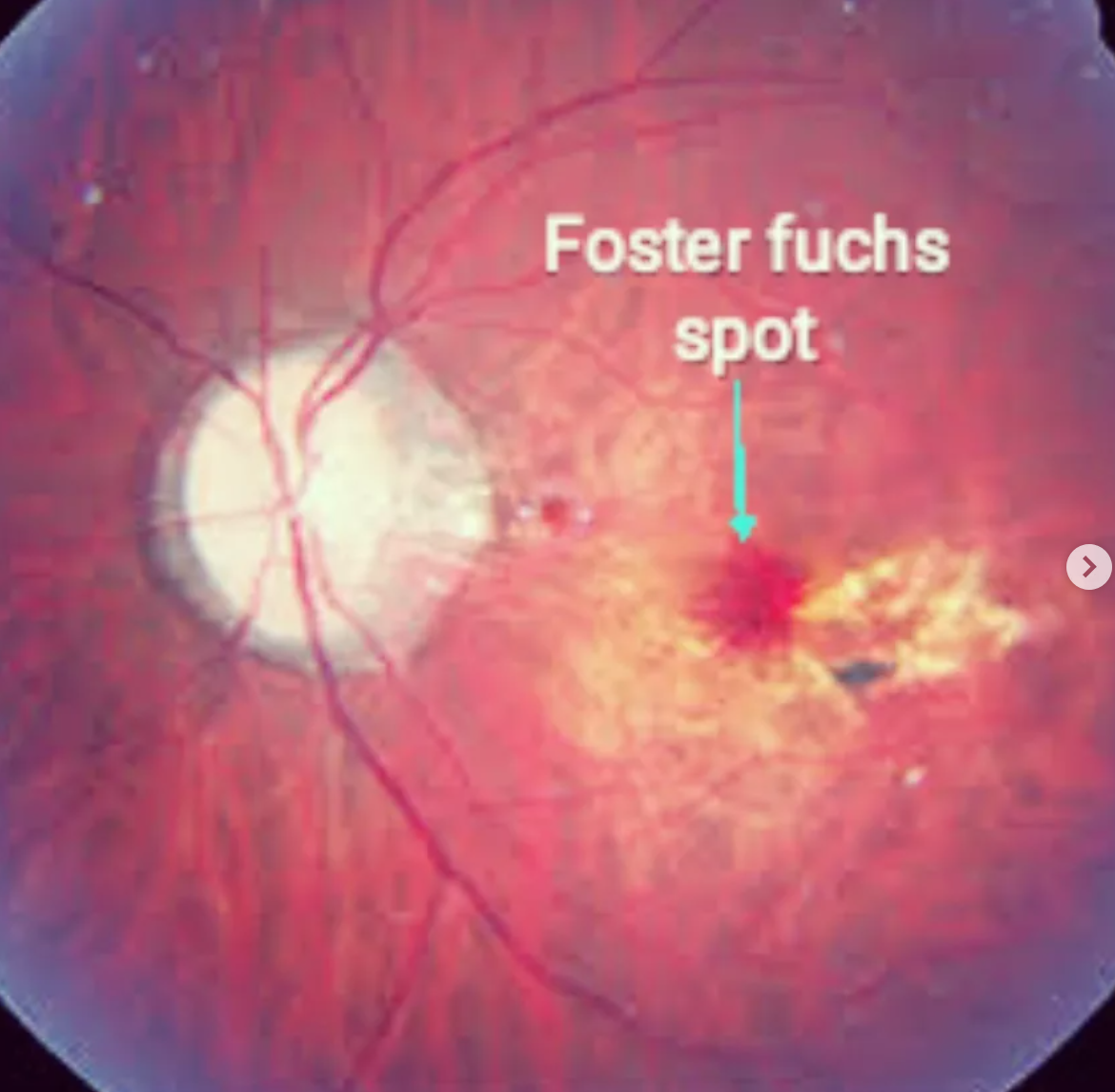
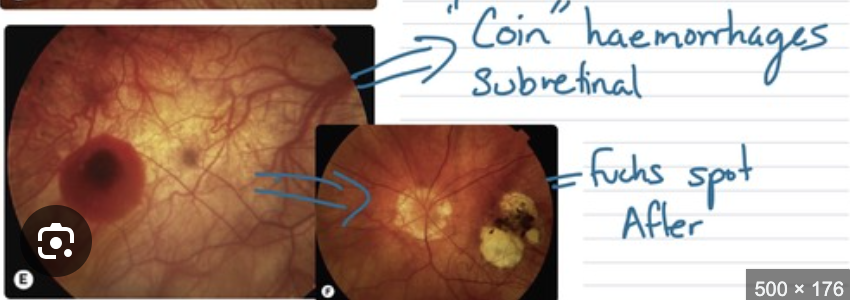
Fuchs’ spots (dark spots from RPE hyperplasia)
If lacquer crack bleeds → leaves a pigmented scar in macula
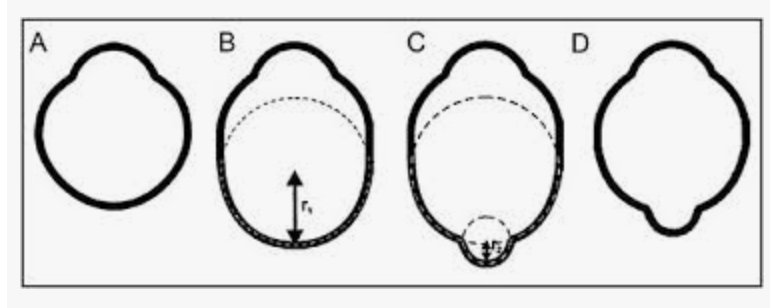
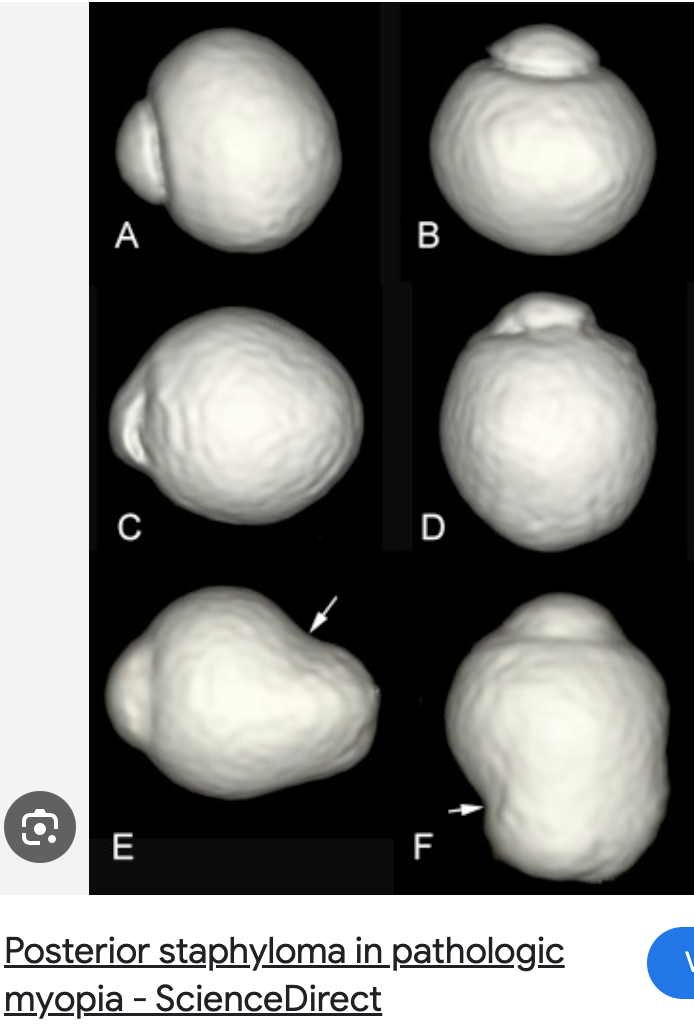
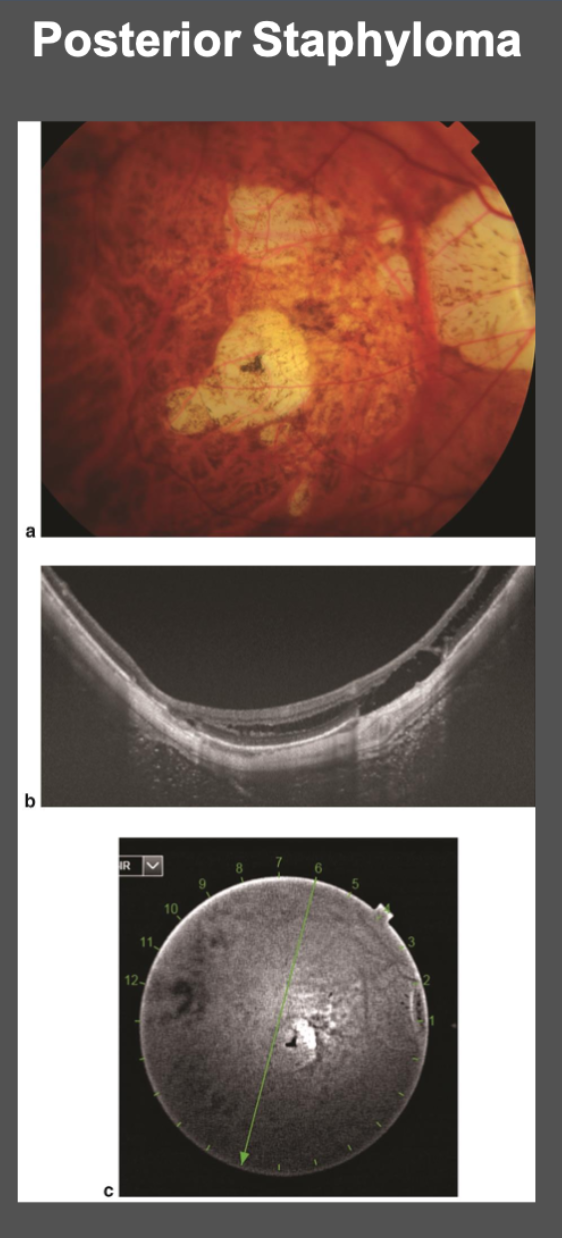
Posterior staphyloma (outpouching of post seg as white circles = visible choroid)
NOT same as gyrate atrophy = this usually has high myopia too, BUT this atrophy isn't caused by the refractive error— it's metabolic toxic buildup

Retinal holes and detachments
PVD
Lattice degeneration
Pathological myopia tx?
Contact lenses preferred over glasses
Less image minification and prismatic effects
Glasses wearers - recommend polycarb
CNVM → Anti-VEGF
Retinal holes + detachments → tx accordingly
Chorioretinal atrophy → no tx
May benefit from Low Vision devices
CNVM VS. NVD/NVI/PDR neo
Who gets CNVM?
If the pathology is Under the retina (Choroid/Bruch's), it's CNVM
If it's In/On retina, it's Neovascularization (NV).
Common CNVM Causes (CHESS):
C: Choroidal Rupture (Trauma).
H: Histoplasmosis (POHS).
E: Exudative AMD (Wet AMD).
S: Serpiginous Choroiditis.
S: Sight-threatening Myopia (Pathologic Myopia/Lacquer Cracks).
Hard exudates are simply lipids and proteins left behind when watery part of blood (serum) leaks out of vessel + gets reabsorbed
"Salt" left behind after "seawater" evaporates
"Basement" Leak (CNVM in AMD/Myopia)
Source: Fragile new vessels growing from Choroid up through Bruch's Membrane
Location: Fluid/exudates sit under retina (subretinal)
Look: Localized, dirty-gray-green "tuft" with exudates/blood gathered right around that specific spot in Macula
"Wall" Leak (Diabetes & HTN)
Source: Pre-existing Retinal Capillaries that have become leaky due to high sugar (Diabetes) or high pressure (HTN)
Location: Fluid/exudates sit inside retina (Intraretinal)
Look:
Diabetes: Exudates often form Circinate Ring (circle of yellow spots) around leaking microaneurysm
Summary: The Diabetic "Leak" Timeline
Sugar damages pericytes → Capillaries get weak.
Weak capillaries → Microaneurysms → CME and Dot/Blot Hemes.
Capillaries close up → Retina loses oxygen (Ischemia).
Ischemia → VEGF is released.
VEGF → Neovascularization → Vitreous Hemorrhage
Vitreous Hemorrhage or Tractional RD
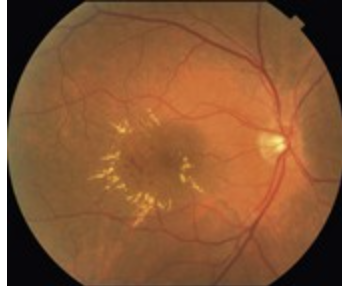
HTN: In severe cases (Grade 4), you see Macular Star
Fan-like spray of exudates radiating from fovea because fluid is being pushed into Henle's layer of retina
Also in HTN, pressure so high it pops superficial capillaries in Nerve Fiber Layer (NFL) = why HTN gives you Flame Hemorrhages, whereas Diabetes gives you Dot and Blots
***Blood-retinal barrier in a diabetic is failing in inner retina (the capillaries)
Oxygen problem (ischemia) is happening in retina itself, so new vessels grow on top of retina (NVD/NVE).
NVD/NVE (Diabetes/CRVO): These vessels grow on top of retina or into vitreous
Visual clue: They look like "frond" of sea anemone or tangled "fan" of fine, red vessels
Follow retinal veins
Vessel color: Bright red
“Top”
***In AMD or Pathologic Myopia, damage is to Bruch's Membrane (the basement floor)
Because floor is cracked, vessels from the basement (Choroid) can grow up into the room.
CNVM (AMD/Myopia): These vessels grow under retina
Visual clue: You usually don't see individual vessels. Instead, you see a dirty-gray, greenish, or yellowish "tuft" or a mound. Looks like something is pushing retina up from basement
Vessel color: Subdued gray/green/dark
“Bottom”
In AMD, you won’t see "cracks" like angioid or lacquer; you’ll see Drusen (yellow pebbles) instead
Localized fluid (subretinal on OCT) and "random" hard exudates clustered right around lesion because it is a leaky "faucet"
CNVM vs Diabetic/HTN neo vs Coats
Coats CNV vs. Diabetics?
CNVM are similar because both involve Retinal vessels (not choroidal; but Intraretinal) becoming leaky. However, the pattern and cause are different:
"How" (Similarity): Both cases, the blood-retinal barrier is broken. Serum leaks out of retinal capillaries, leading to lipid formation = mix of Hard Exudates/Edema (fluid).
"Where" (Difference):
Diabetes: Leaks are usually small, scattered microaneurysms across posterior pole. "Dot + Blot" hemorrhages and circinate rings of exudates.
Coats': Leaks are massive, localized "clusters" of Telangiectatic vessels (often in temporal periphery). Like one giant broken fire hydrant vs. hundred tiny dripping faucets.
The Difference from “CHESS” CNVM: Comes from under the floor (the choroid)
VS. the "lightbulb" vessels in Coats' are part of retina's own plumbing.
"Sea of Yellow": Because these vessels are so high up and leak SOOO massively, hard exudates (lipids) often settle deep into the outer plexiform layer or even subretinal space, which is why you see massive yellow "mountain" pushing retina forward
Feature | Coats' Disease | Diabetic Retinopathy |
Vessel Look | "Lightbulbs" (Telangiectasia) | Microaneurysms / IRMA |
Exudates | Massive / Sheets of Yellow | Small / Circinate Rings |
Laterality | Unilateral (85%+) | Bilateral |
Patient | Young Boys (avg. age 8-10) | Adults with high blood sugar |
Coats' and Serous (Exudative) RD
Serous RD
Think of it this way: In Coats, "leaky lightbulbs" dump so much fluid that RPE (pump that keeps retina dry) can't keep up
Fluid builds up under retina until it literally floats retina off back of eye
No hole or tear = Exudative/Serous RD
Diabetes, RD is usually Tractional (pulled by scars)
Summary: The "Vessel Vocabulary" for your Boards
Telangiectasia ("Lightbulbs"): Think Coats' Disease. (Also Leber's Miliary Aneurysms + Von Hippel-Lindau (Retinal Hemangioblastoma) + MacTel).
Microaneurysms ("Red Dots"): Think Diabetes.
CNVM ("Gray/Green Mound"): Think AMD, Myopia, POHS.
NVE/NVD ("Red Sea Fans"): Think Proliferative Diabetes (PDR) or Vein Occlusion.
Enhanced S-cone Syndrome/Goldmann-Favre Syndrome?
Extremely RARE
Autosomal Recessive degeneration
Begins early childhood
Goldmann-Favre Syndrome is SEVERE form of Enhanced S-cone Syndrome
Enhanced S-cone Syndrome/Goldmann-Favre Syndrome symptoms?
Nyctalopia (night blindness)
Blue light sensitivity
Blurry vision
Enhanced S-cone Syndrome/Goldmann-Favre Syndrome signs?
Goldmann-Favre Syndrome presents as:
→ Bilateral retinal pigmentary + vitreous degeneration with macular retinoschisis (& sometimes peripheral retinoschisis)
sometimes also CME if fluid accumulates within splitting layers (esp for cases like genetics where retina is “sick”)

Enhanced S-cone Syndrome/Goldmann-Favre Syndrome tx?
If CME → topical CAIs (e.g., Dorzolamide or Brinzolamide; these uniquely help with both IOP lowering & CME issues)
Progressive issue → condition likely to get worse despite tx (“prognosis gaurded”)
In Gyrate Atrophy or Retinitis Pigmentosa (RP), the CME isn't a one-time event (like after cataract surgery)
Actual "machinery" of retina is slowly dying
Treatment Limit: CAI drops treat the symptom (the fluid), but don't fix the genetic mutation (broken enzyme)
Progressive Nature: Since RP + photoreceptors keep degenerating over decades, vision will likely keep declining even if you keep macula "dry" for few years
Retinoschesis?
Splitting layers within the retina
VS. Retinal Detachment = retina is detached from RPE/Choroid
Dome-shaped lesions in retinal periphery
May look very similar to RD
Any visual field defects from Retinoschesis?
YES! Intra-retinal visual pathway disrupted:
Absolute VF defect with sharp borders
VS. RD = Relative VF defects
How to distinguish RD from Retinoschesis?
HVF testing
Scleral indentation
OCT
***NOT Fluorescein Angiography
Retinoschesis:
NO Tobacco Dust/Shafer’s sign (may see on RD)
Rarely → can have associated Rhegmatogenous RD + Vitreous hemorrhages
Retinitis Pigmentosa?
What else for this section?
RDs
Breaks/holes
lattice/snail
retinoschesis
myopia - lead to RDs (all myopia stuff)
RP
star
best/vitilli
fam
leber
Maculopathies?
Any pathological change/disease - specifically affecting macula
Central part of retina responsible for detailed, color, "straight-ahead" vision
Look for loss of Visual Acuity (VA) and central distortions (metamorphopsia)
6 maculopathies:
Macular Telangectasia
Macular Hole
Cystoid Macular Edema (CME)
Central serous chorioretinopathy (CSCR)
Age-related Macular degeneration (ARMD)
Epiretinal membrane (ERM)
Macular Telangectasia?
Telangectasia = abnormally dilated capillaries
Usually caused by another retinal disease
Rarely idiopathic
***IF ever rarely idiopathic? Macular Telangectasia
3 types!
Similar to Coat’s disease (progressive, vascular abnormalities are = leaky → hard exudates deposit
Macular Telangectasia symptoms?
Progressive loss of central vision
Macular Telangectasia signs?
Macular findings:
Atrophy
Exudates
Pigmentary changes
Hemorrhage from CNVM
Macular Telangectasia 3 types?
MacTel Type 1 = essentially a localized, adult-onset version of Coats' Disease (vascular issue)
Exudates found in perifovea + periphery
Middle-aged men
“Form frust” (incomplete or “mini version”) of Coat’s disease
Unilateral
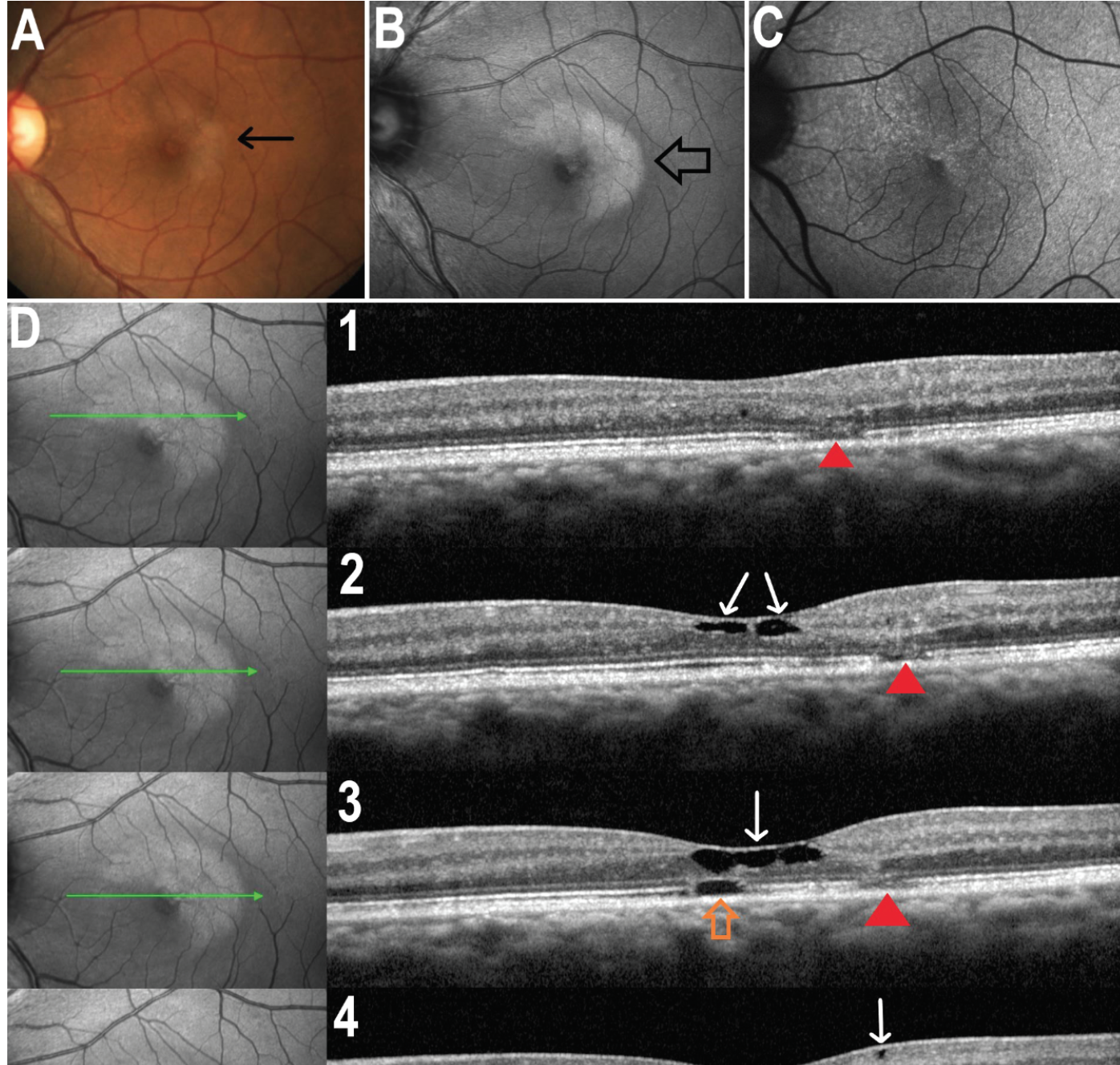
MacTel Type 2 is "dry" and has no exudates - cellular problem
MORE common than Type 1
WORSE visual prognosis than Type 1
Neurodegenerative changes temporal to fovea center w/ILM drape on OCT (on OCT scan, will be large, empty-looking cavities/hyporeflective spaces in middle layers of retina)
Can progress to "Wet" phase where secondary CNVM causes exudates + hemorrhages you’d normally see in Wet AMD (now needs Anti-VEGF)
Atrophy + pigmentary changes → advanced cases
Müller cells die!!! These cells - responsible for holding onto macular pigment (lutein + zeaxanthin)
Hyper-autofluorescence on FAF (due to loss of macular pigment)
Hyporeflective on OCT
Fluorescein Angiography (FA) = Late temporal leakage (diffuse "blush")
Invasive test - injecting dye (Sodium Fluorescein) into patient’s arm
OCT-A = Missing capillary network in deep plexus
MacTel Type 3: Occlusive Telangectasia
RARE
60s age
Capillaries occluded
VERY poor visual prognosis
If you see
question about MacTel mentioning "Systemic association" or "Capillary occlusion," think Type 3
MacTel tx?
Anti-VEGF injections for associated CNVM
The "Dye" (FA) vs. The "Glow" (FAF)
Condition | FA (Dye) Keyword | FAF (Glow) Keyword |
Stargardt's | Silent Choroid (Blackout) | Pisciform Flecks (Bright) |
Best's | Masking (Dark hole) | Egg Yolk (Very Bright) |
Plaquenil | Window Defect (Ring) "Bull’s Eye Maculopathy" | Stressed Ring (Bright) Hyper-FAF Ring |
CME | Petaloid Leak | Usually normal / subtle |
MacTel 2 | Temporal Blush (late leak) | Hyper-fovea (Lost pigment) |
CSCR | Smokestack / Inkblot | Descending Tracts (Gravity) |
Exudates?
Hard Exudates | Soft Exudates (CWS) | |
Material | Lipids / Proteins | Infarct/Collection of Swollen Axons (Debris) |
Problem | Leaky Vessels (Wet) | Clogged Vessels (Dry) |
Looks | Yellow, Shiny, Sharp borders | White, Fluffy, Fuzzy borders |
Location | Deeper (Outer Plexiform Layer) | Superficial (Nerve Fiber Layer) |
Presence of exudates tells you the severity of a disease
Hard:
Condition | Recognition / Board Clue | Treatment | Fluid Name |
Diabetes (CSME) | Circinate rings of yellow dots | Anti-VEGF or Focal Laser | Macular Edema/CSME/DME |
Coats' Disease | Massive "Puddles"; Young boy; Lightbulb vessels | Laser/Cryo to vessels | Exudative RD |
HTN Retinopathy | Bilateral Macular Star + AV Nicking + High BP | BP Control | Macular Edema |
Cat Scratch (CSD) | Unilateral Macular Star + Swollen Nerve + Fever | Antibiotics (Azithromycin) | Serous Fluid |
RAM (Macroaneurysm) | Single localized ring on one artery | Observation or Laser | Localized Edema |
Von Hippel-Lindau | Exudates near a red "orange" tumor | Laser/Cryo to tumor | Exudative RD |
Soft:
Condition | Recognition / Board Clue | Treatment |
Pre-Proliferative DR | >1 CWS (4-2-1 rule); Dot/Blot hemes. | Monitor closely for Neo. |
HIV Retinopathy | CWS in a patient with a low T-cell count. | Manage the HIV (HAART). |
HTN (Grade III) | CWS + Hard Exudates + Hemorrhages. | Urgent BP control |
CRVO / BRVO | CWS + "Blood and Thunder" (Massive hemes) | Anti-VEGF for edema |