Pressure Relief, Positioning, Bed Mobility
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
Appropriate Positioning
promotes muscle tone control
provision of appropriate sensory info
prevents ROM loss, preservation of joint stability
increased spatial awareness
assistance with safer eating
prevents aspiration, contracture, pressure areas, shoulder pain, extremity swelling, reduced QoL, death
promotes comfort and increased position tolerance
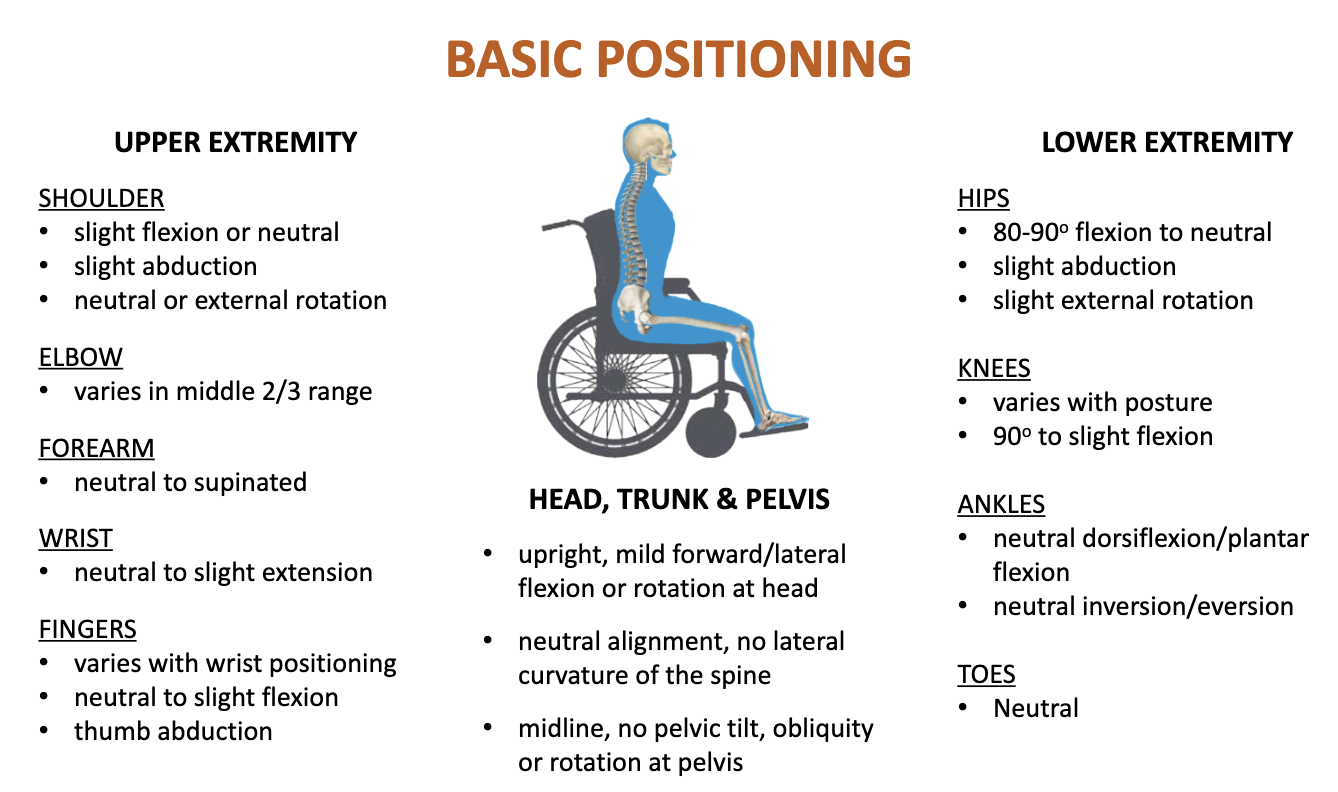
Basic Positioning
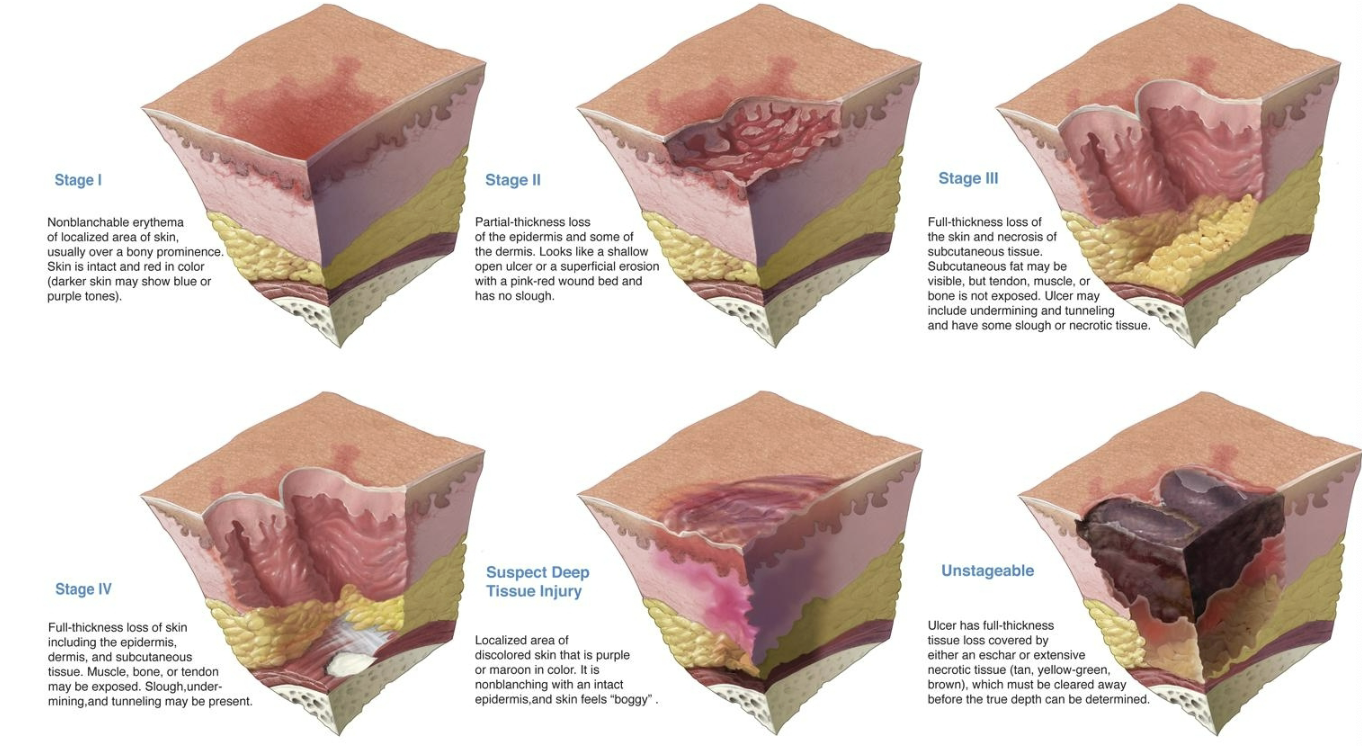
Pressure Ulcers
aka pressure injury, pressure sore, decubitus ulcer, bedsore, skin breakdown
can be life threatening
can be prevented
high risk areas: bony prominences at sacrum, ischium, trochanters, elbows, and heels, iliac crest scapula, knees, toes, occiput, rib cage
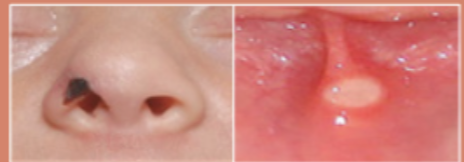
Mucosal membrane pressure ulcer
found on the mucosal membrane, typically caused by a device at injury location
can’t be staged due to the anatomy of mucous membrane
can be caused by supplemental oxygen, CPAP, nasal prongs, endotracheal tube
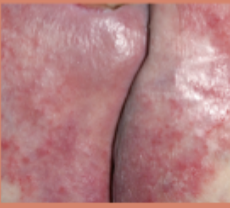
Incontinence/Moisture lesion
caused by moisture not pressure/shear force
skin is damp and not necessarily located on bony prominences
often misclassified as pressure ulcures
there can be a combo of pressure and moisture damage
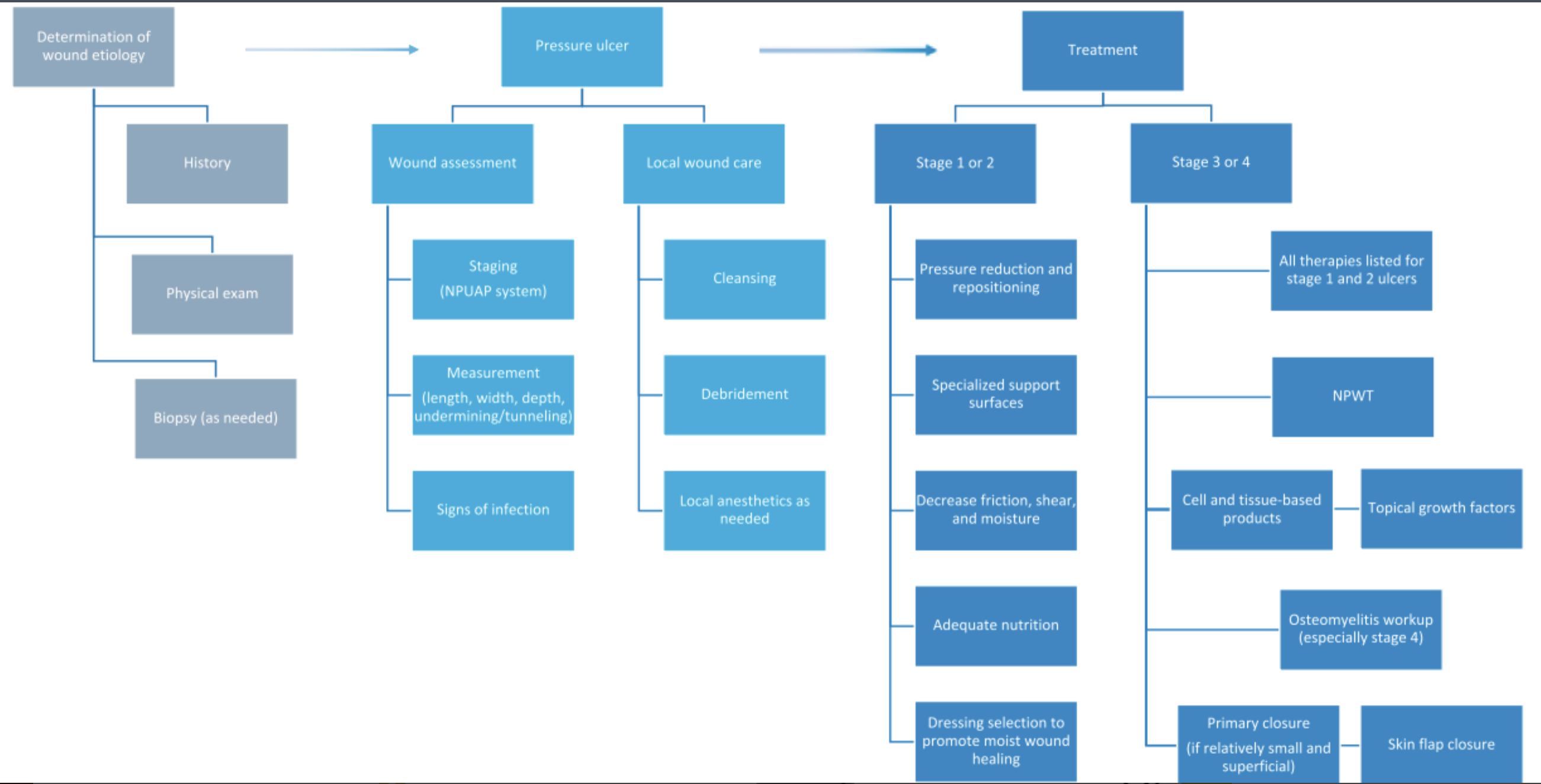
Flow chart for managing pressure ulcers
OT role in pressure ulcers
be aware of signs of developing problems
regular pressure relief and skin inspections
routine turning and repositioning
keep skin clean and dry
maintain adequate nutrition/hydration
wear properly fitting clothing and shoes
specialized bedding and wheelchair cushions
proper transfer techniques
protect bony prominences
SSKIN
surfaces
skin inspection
keep moving
increased moisture
nutrition
greatly assist in prevention
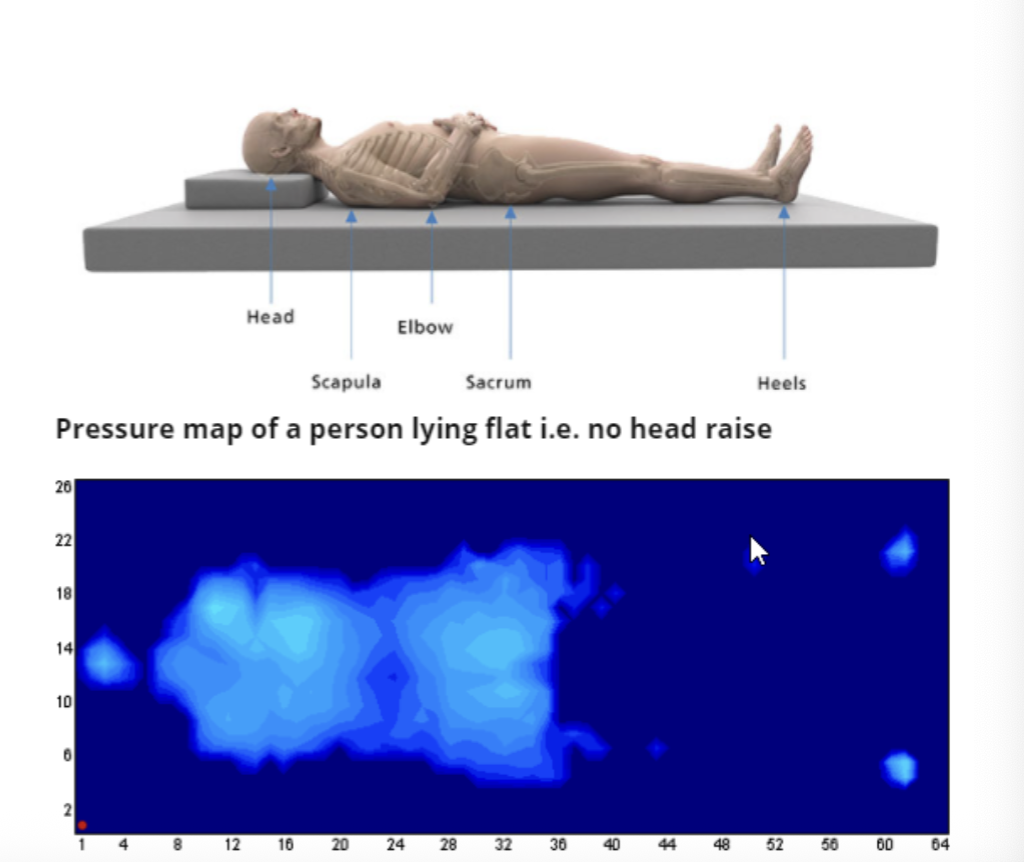
pressure mapping
measurement and visual reporting of pressure between two contacting surfaces
supine positioning
single pillow placed under head
pillow placed under affected shoulder and arm
slight shoulder flexion, abduction, neutral rotation
high tone- place pillows or blanket rolls to assist in positioning the arm away rom the body
LEs neutral- extension, slight hip ER, slight hib abd
use towel rolls to prop heel to reduce heel pressure
use pillows to elevate LE with edema
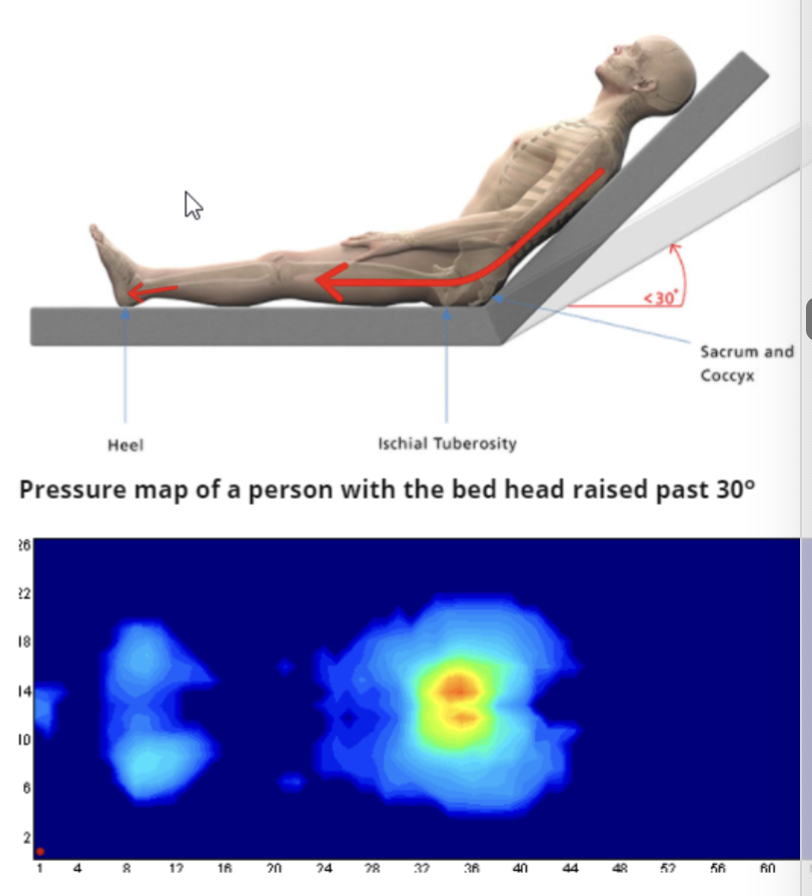
supine positioning: head and bed elevated
head of bed elevated >30 d increases pressure at sacrum
everything else the same as fully supine
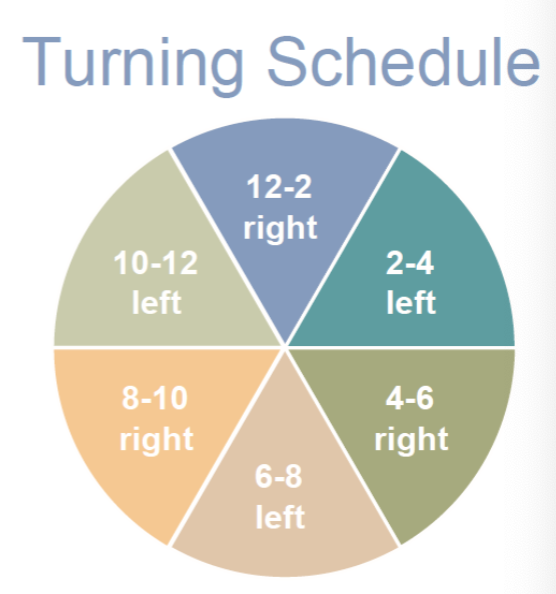
Turning clock schedule: pressure prevention
team effort across nursing and therapy to prevent pressure injury
signs can be posted in all rooms
when returning a patient to bed, check the time an position based upon the schedule
Respiratory Considerations
greater efficacy occurs with respiratory treatments when patients are positioned >30 d due to respiratory mechanics
sitting and standing lead to highest lung volumes where lung and chest wall elastic recoil are greatest
positioning impacts pulmonary function tests
testing SCI patients in supine can provide important info
Tube Feed Considerations
when patients are receiving tube feedings, every effort needs to be made to minimize aspiration
elevate the head of bed to 30-45 d at all times, unless contraindicated
bolus feedings- have patient sit if possible and for 1 hour after the feeding; if they can’t sit, have HOB elevated at least 45 d
there is no benefit from stopping feedings during short periods of HOB lowering, such as during linen changes
if prolonged procedure will require HOB lowering, the gastric feedings should be stopped during the procedure; feeding should be promptly returned and patient return to HOB elevated position
generally small bowel feedings don’t need to be stopped

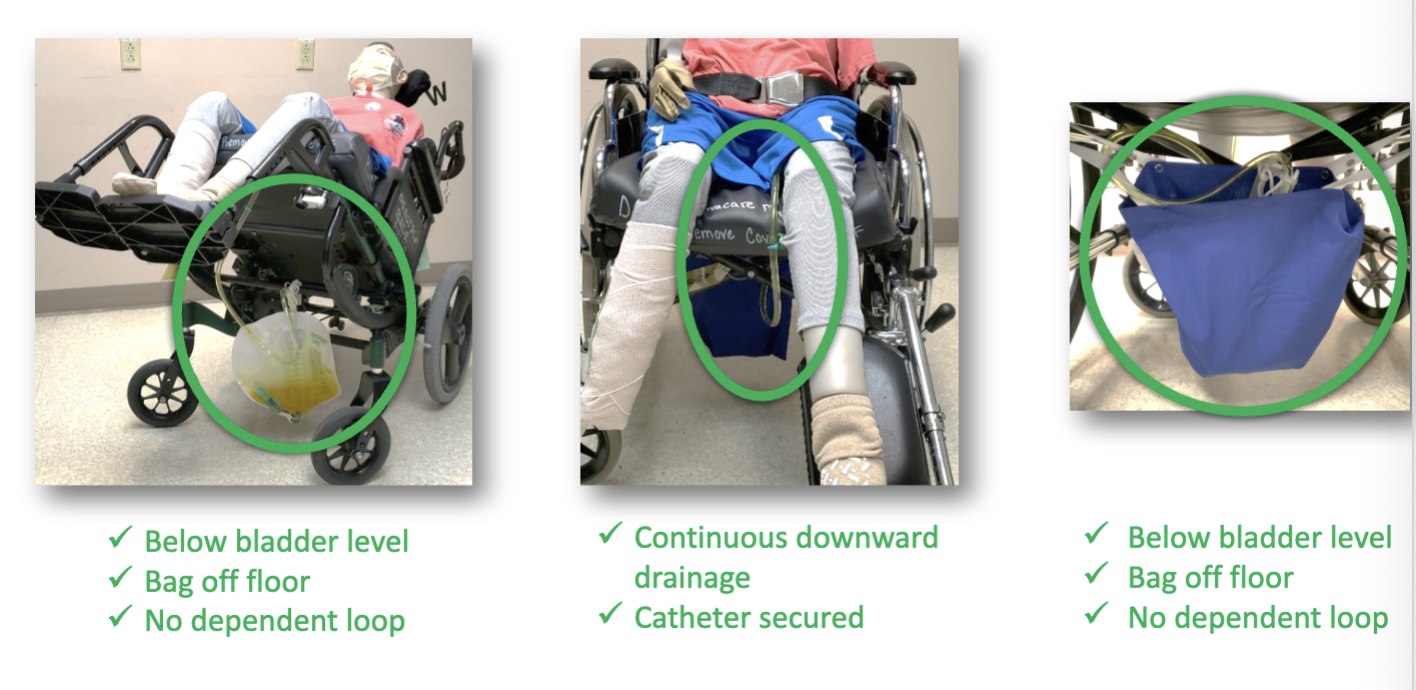
Foley Care Considerations
preventing catheter-associated UTIs requires team approach
ensuring continuous downward drainage
paying attention to foley placement during transfers
placing below bladder level at all times
Fixed vs Flexed Posture Wheelchair
fixed posture (accommodate)- skeleton does not move out of that posture; equipment must provide optimal support and pressure redistribution; prevent further progression
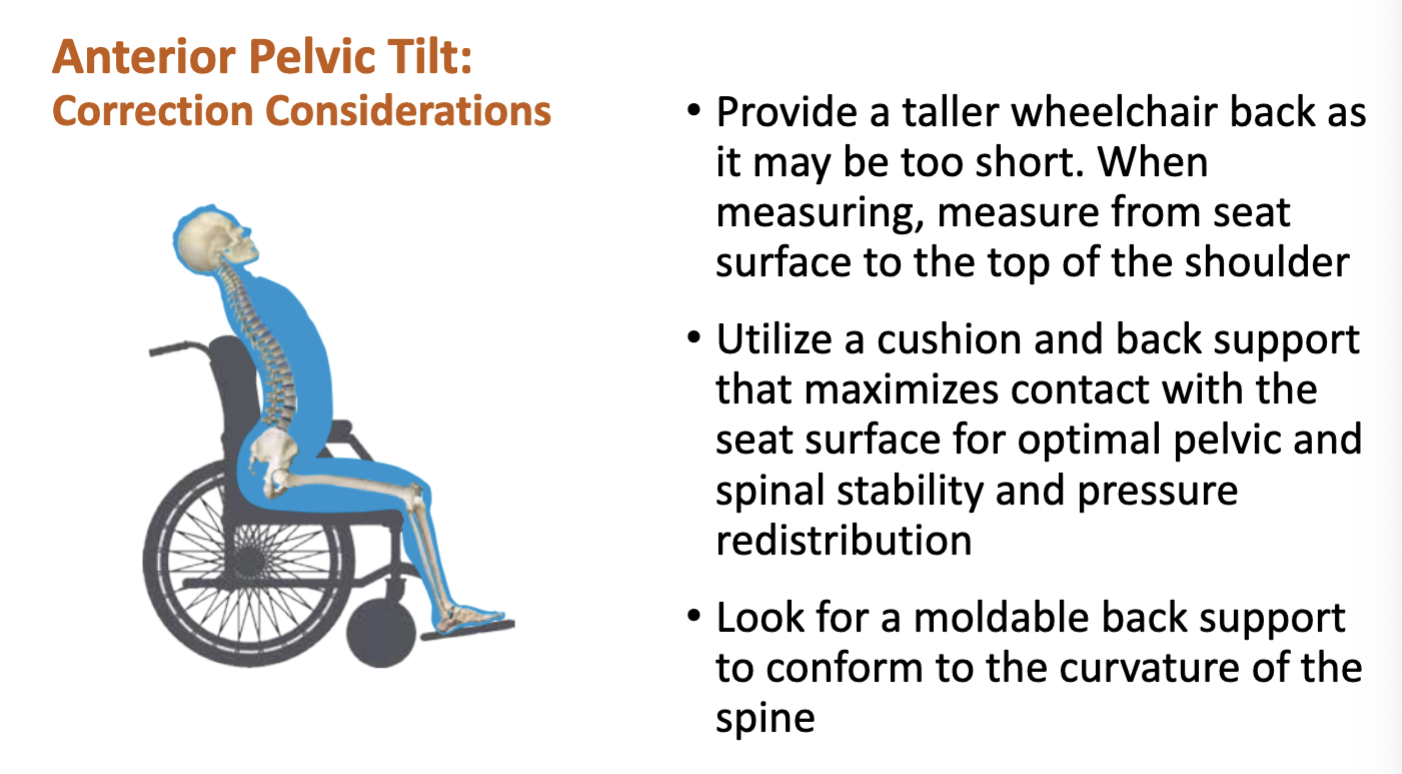
flexed posture (correct)- skeleton still moves; equipment should correct abnormal posture; prevent fixed posture, achieve most neutral posture that can be maintained over time with support
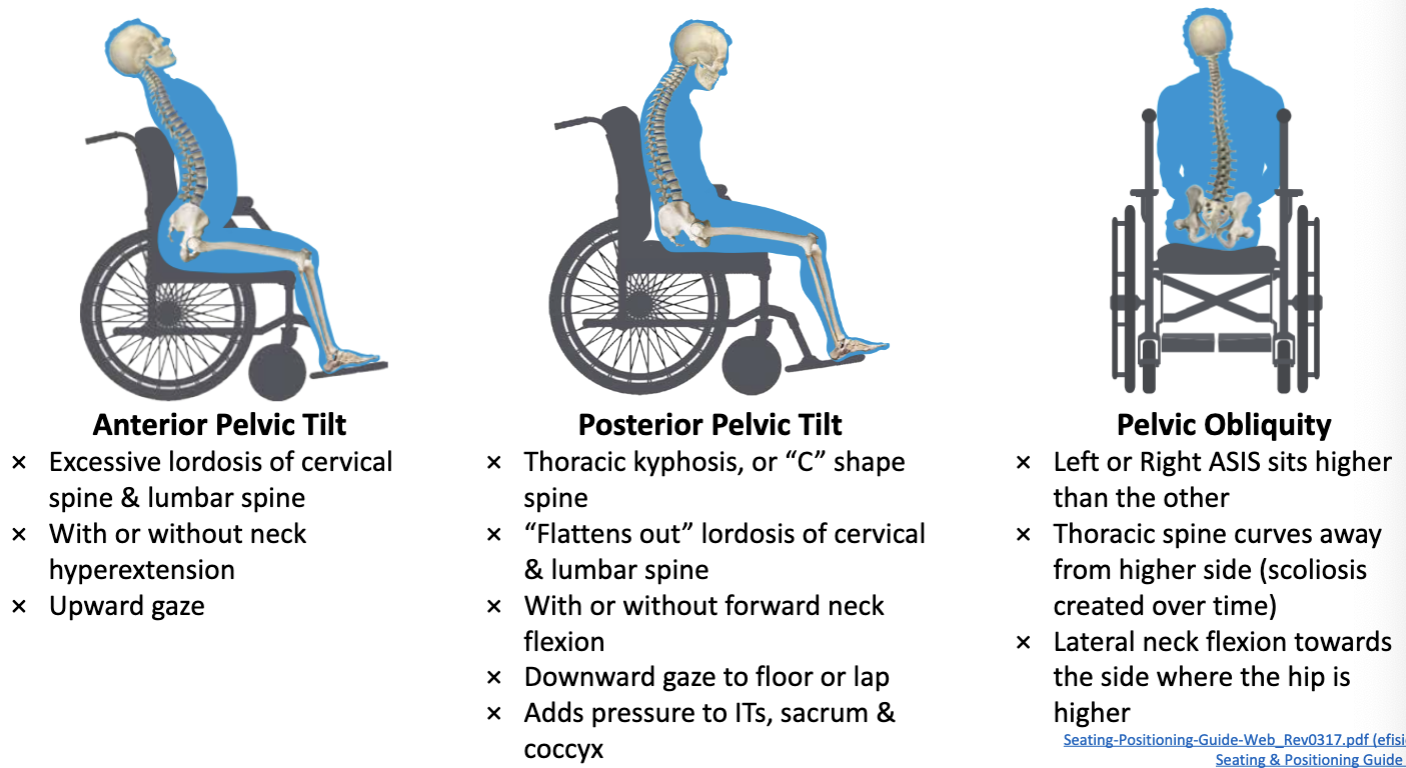
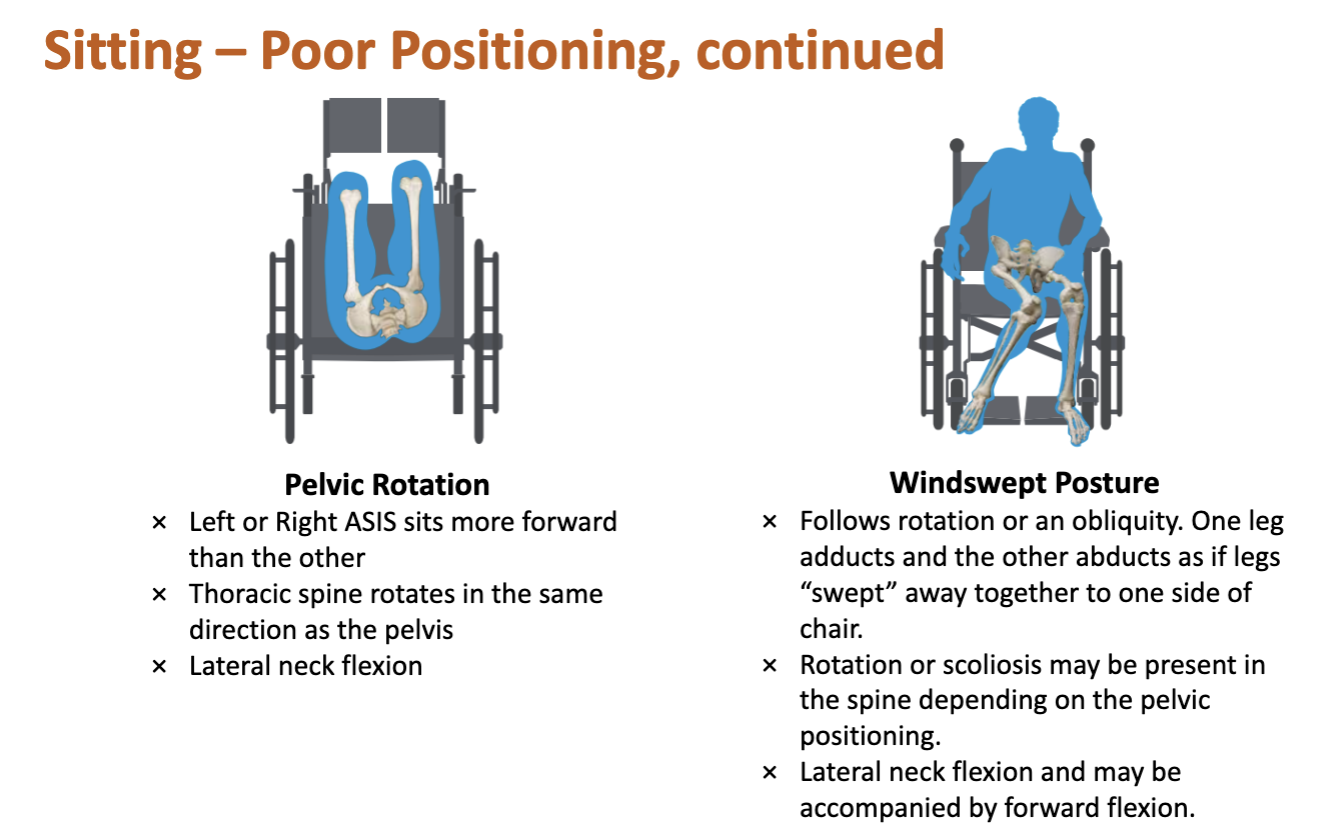
Sitting-Poor Positioning
Sitting Positioning- Pelvic Tilt

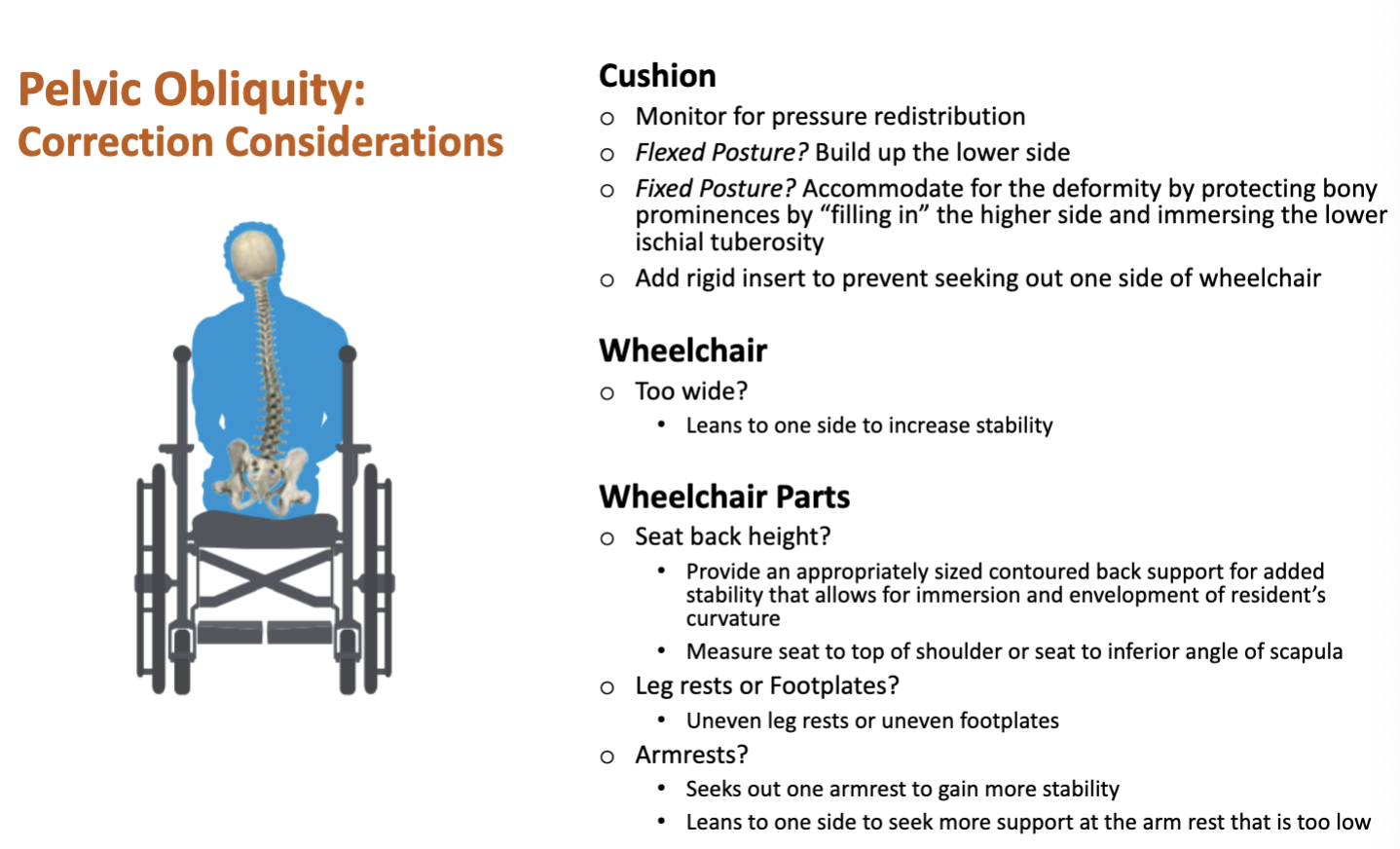
Pelvic Obliquity Sitting Posture
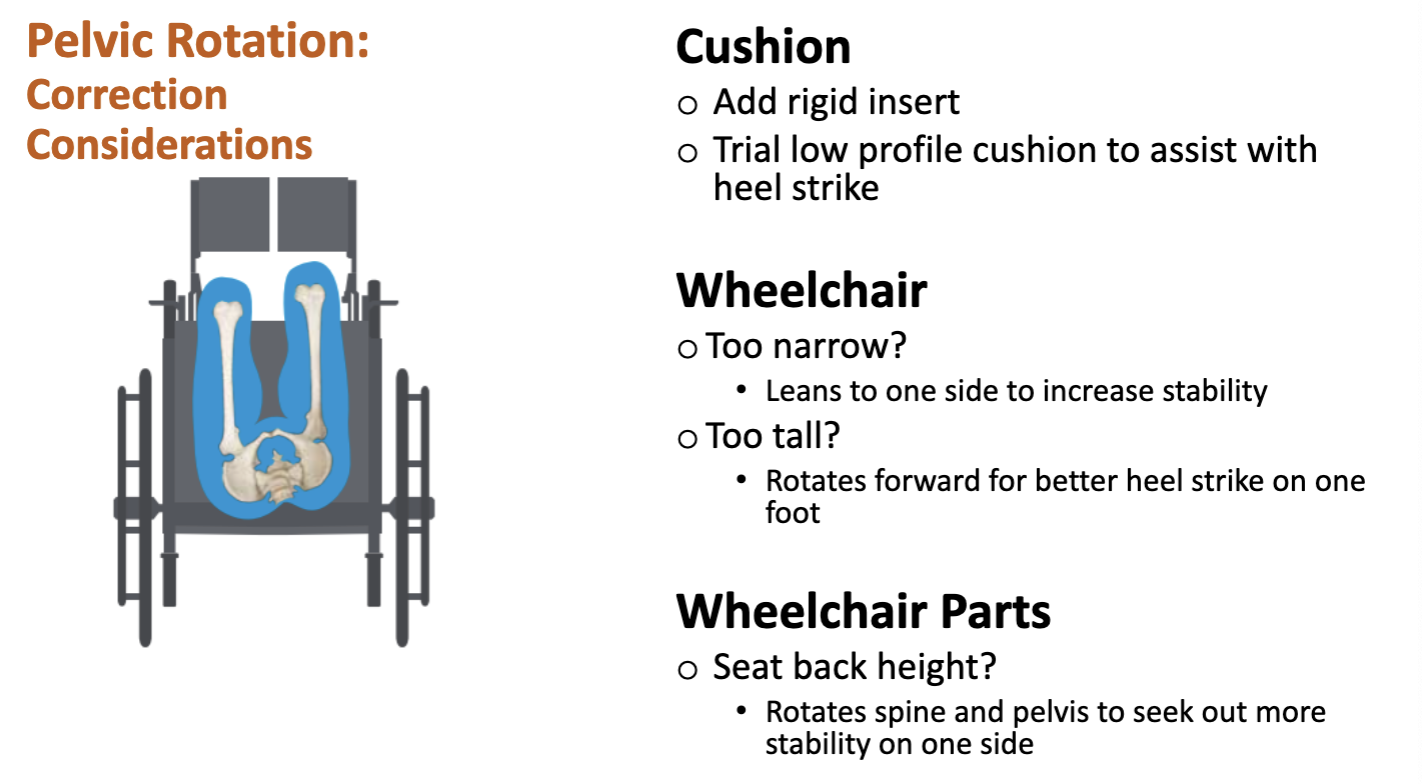
Pelvic Rotation Sitting Posture
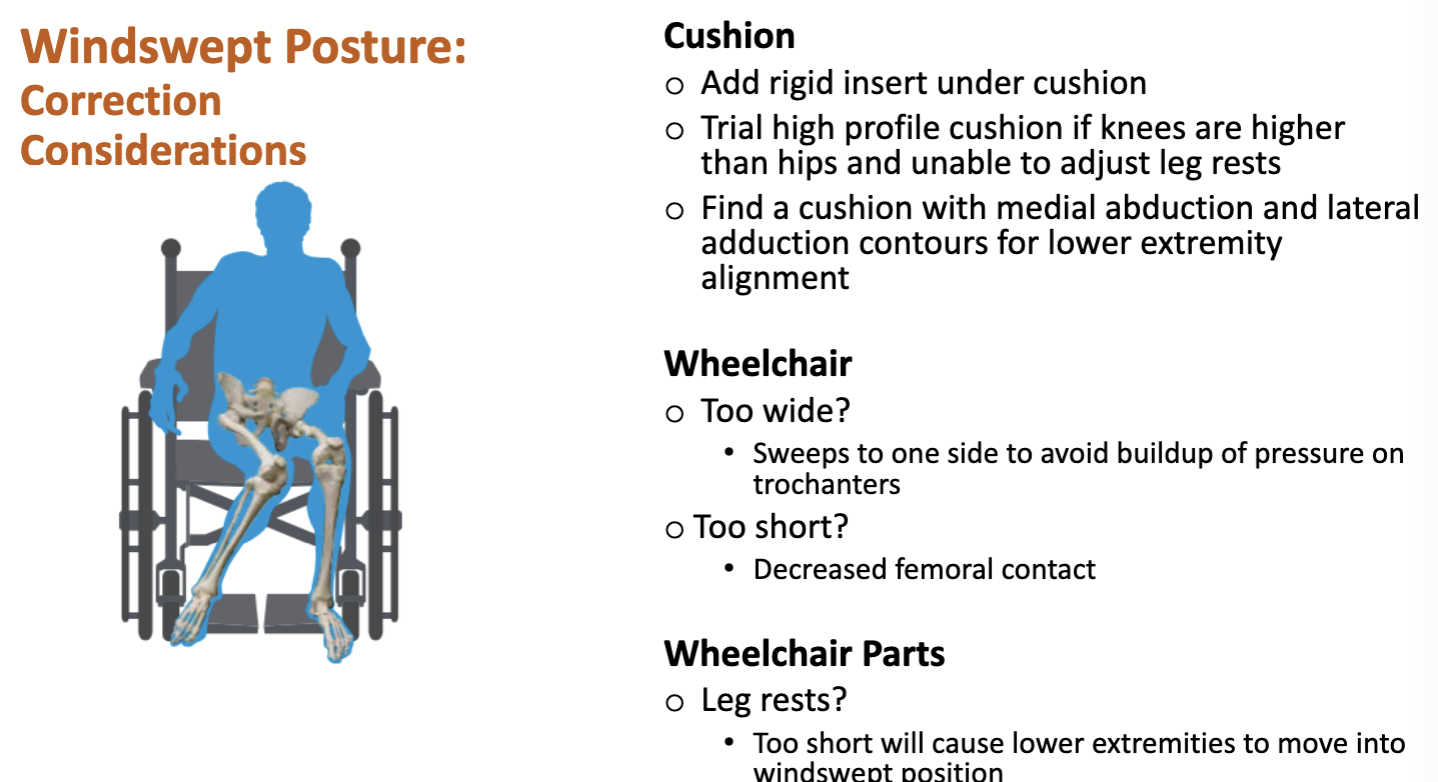
Windswept Posture Sitting Posture
Ortho Positioning
know all precautions before moving
monitor leg rest and footplate positioning, wheelchair height, cushion height for hip precaution compliancy
ensure cushions precent rotation that may impact spinal precautions
SCI Positioning
cushions filled with air can offer reduced support for individuals with limited trunk control
be aware of how the patient is sitting or lying and for how long
impaired sensated reduces skin breakdown awareness
monitor foot plate placement, avoid foot dragging or obstacle collisions
7-33% of injuries in PW are cause by catching a LE on a doorframe
have a pad on the head rest to protect suboccipital region
on or above occipital area causes neck strain
on the cervical spine results in poor posterior support and head extension
Stroke Positioning
protect the affected limb, don’t allow UE to dangle
less common to sit in wheelchair or lay supine for long periods
recommended: sitting in an armchair, side lying on unaffected side, then side lying on affected side
Amputee Positioning
avoid positions that induce risk for hip and knee contractures
below knee: support residual limb and maintain knee extension when seated, use an amputee board at wheelchair level, use a second chair of same height when seated in regular chair
do not allow the residual limb to ever dangle
Brain Injury Positioning
extensor tone is common with individuals post TBI; increases risk for sliding forward out of w/c
tilt-in-space w/c help