CHAPTER 12: PHASE 4: PERIODONTAL MAINTENANCE
1/38
Earn XP
Description and Tags
+ discussion and ppt
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
periodontal maintenance
aka: supportive periodontal treatment (SPT)
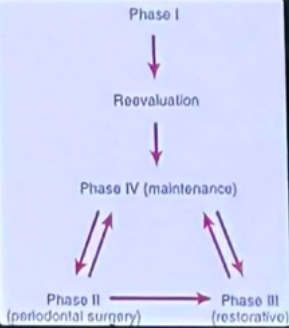
phase IV of periodontal therapy
long-term phase after active periodontal therapy
begins immediately after phase I (initial therapy)
surgical (phase II) and restorative (phase III) treatments occur during this phase
rationale of supportive periodontal treatment (SPT)
high risk of disease recurrence due to:
incomplete bacterial removal
difficult tissue healing
non-compliant patients have higher risk of tooth loss
significance of supportive periodontal treatment (SPT)
essential for long-term tooth preservation
non-compliant patients:
5.6× greater risk of tooth loss
inadequate SPT after regenerative therapy:
50× higher risk of probing attachment loss
classify patients based on:
severity
extent
location of periodontal disease
basis for recurrence and need for maintenance
cross-contamination
motivation and oral hygiene
healing pattern (histologic)
incomplete plaque removal (etiologic)
subgingival plaque regrowth
remaining plaque regrows inside periodontal pockets
regrowth is slow and may not show immediate inflammation
intragingival bacteria
bacteria remain within gingival tissues
not fully removed by:
scaling
root planing
flap surgery
can recolonize and cause recurrence
within 9–11 weeks
pathogens can return to original levels typically __
healing pattern (histologic)
healing usually forms long junctional epithelium
not true new connective tissue attachment
this attachment may be:
weaker
more prone to pocket recurrence
cross-contamination
periodontal bacteria can spread between:
spouses
family members
reinfection risk increases, especially if pockets remain
part I: examination and evaluation (~14 minutes)
goal → identify changes since last visit
clinical assessment:
update medical history, oral pathologic examination
check for:
gingival changes, pocket depth changes
mobility changes, occlusal changes
plaque control check:
evaluate patient’s oral hygiene, reinforce it
patient should perform hygiene routine before appointment
radiographic examination:
individualized based on severity and past findings
compare with previous radiographs to assess:
bone height, healing of osseous defects
trauma from occlusion, presence of caries
part II: treatment (~36 minutes)
hygiene reinforcement
scaling and root planing
perform where needed
avoid instrumenting normal sites (1–3 mm sulci)
prevent loss of attachment from repeated scaling
polishing
chemical irrigation / site-specific antimicrobials
used for patients with remaining pockets
part III: scheduling and administration (~10 minutes)
discuss findings with the patient
documentation
cleaning
schedule next recall visit
schedule additional periodontal/restorative treatment if needed
3 months
initial recall interval
first-year patients
recall not longer than 3 months
purpose:
reinforce hygiene
evaluate surgical outcomes
1-2 months
recall intervals for difficult first year patients
merin classification and recall intervals
class A (excellent / well maintained)
class B (reasonably well maintained)
class C (poor results / multiple negative factors)
class A (excellent / well maintained)
good oral hygiene
no remaining pockets
no teeth with <50% bone support
managed by general dentist
recall intervals for class A patients
6 months – 1 year
class B (reasonably well maintained)
heavy calculus
systemic disease
inconsistent hygiene
some remaining pockets
smoking or some teeth with <50% bone support
alternating care: general dentist + specialist
recall intervals for class B patients
3–4 months
class C (poor results / multiple negative factors)
advanced disease
complicated prostheses
many remaining pockets
smoking or many teeth with <50% bone support
managed by specialist
recall intervals for class C patients
1–3 months
signs of a failing perio case
recurring inflammation
increased bone loss (radiographs)
gradual increase in tooth mobility
increasing sulcus depth (pocket formation)
causes of recurrence
inadequate restorations
failure to return for visits
incomplete calculus removal
poor patient plaque control
poor compliance with SPT schedule
systemic diseases affecting host resistance
1–2 weeks
decision to retreat should be delayed for __ after maintenance visit to allow resolution of edema
factors to consider referral
pocket depth
≥5 mm (from cementoenamel junction)
indicates risk of rapid deterioration
location / extent
extensive osseous surgery
complex regenerative procedures
surgery on distal surfaces of second molars
teeth with furcation involvement (even if >50% bone support)
other factors
systemic health problems
dental implant patients
complex prosthetic cases
general rule
if case is not clearly simple → refer to specialist
peri-implantitis
bone loss around implant
susceptible for px with dental impants
more prone to plaque-induced inflammation than natural teeth
implant microflora link
similar to tooth microflora in partially edentulous patients
healthy tooth microflora is important for implant health
instrumentation when handling implants
special instruments required for titanium surfaces; a key difference
avoid:
metal hand instruments
ultrasonic/sonic tips
(can damage or alter titanium surface)
use:
plastic instruments
gold-plated curettes (specially designed)
for safe calculus removal
chemical / prophylactic agents when handling implants
avoid:
acidic fluoride agents
daily acidic fluoride
use:
nonabrasive prophy pastes
take periapical or vertical bite-wing radiographs at:
6 months
12 months
36 months after prosthesis placement
[ then every 36 months unless problems occur ]
correct sequence of treatment phases
maintenance begins immediately after phase I reevaluation with surgery and resto care performed during the maintenance phase
>6mm
probing depth which scaling is generally ineffective
2 automated risk calculators to predict perio progression
periodontal risk assessment (PRA)
periodontal risk calculator (PRC)
[ no universally accepted objective method exists, risk calculators should complement, not replace good clinical judgement ]
cases to refer a specialist
complex implants
regenerative procedures
extensive osseous surgery
systemic health complication
complex cases (distal surfaces of 2nd molars)
cases requiring co-management
cases general practitioner can handle
minor flap surgery
class A recall maintenance
localized nonsurgical therapy
>5mm pockets from the CEJ or furcation invasions
even with 50% bone support
it carries a questionable prognosis and are usually best treated by a specialist