Prof Nursing 2 - content before finals
1/152
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
153 Terms
QI in healthcare
systematic approach to making changes that lead to better pt outcomes and stronger health system performance, involves application of QI science
QI
quality improvement
QI science
provides structure, tools and processes to assess and increase efforts for the testing, implementation, and knowledge spread of QI practice
responsible for quality
academic preparation, hc organisations, provincial and federal organisations, professional organisations, professional staff, support staff, pts and families
To Err is Human
US- 1999, pivotal publication bringing pt safety to the forefront of healthcare
almost 98,000 people die from medical errors in hospitals
provides agenda for improving pt safety by designing safer healthcare system
asserts that problem is not with people, but the system
IHI
institute for healthcare improvement (2004), launched campaign to save 100,000 lives by reducing morbidity or mortality in hospitals by using 6 best practice interventions: rapid response teams, improved care for acute MI, medical reconciliation, preventing central line infections, preventing surgical site infections, preventing ventilator associated pneumonia, now aiming for 5 million lives (not just over America)
Canada 2002, building a safer system
outlines a national integrated strategy for improving patient safety in the Canadian health care system, Canada needs collaboration across all sectors, formed CPSI (canadian pt safety institute) (no longer used), using federal funding for improving healthcare errors- annual 2 million given to CMIRPS or Canadian Medication Incident Reporting and Prevention System
CPSI
Canadian patient safety institute- identified gaps in pt care: impact of workload pressure and complexity of care, difficulty in coordinating and sustaining pt safety initiatives, need for stronger safety culture, need to focus on systems focusing on safety, need to support leaders across continuum
nurse’s role in quality
largest group of hc providers and spend that most time with patients, nurses are in ideal situation to observe and address quality gaps, nurses participation in quality improvement process can be critical efforts to improve quality and efficiency of hc system
steps: be aware of quality standards of care, speak up to colleagues when standards aren’t followed, speak up when quality gaps are found, participate in pt care development, include pt and family, become involved in unit based or organisation wide initiative to improve quality
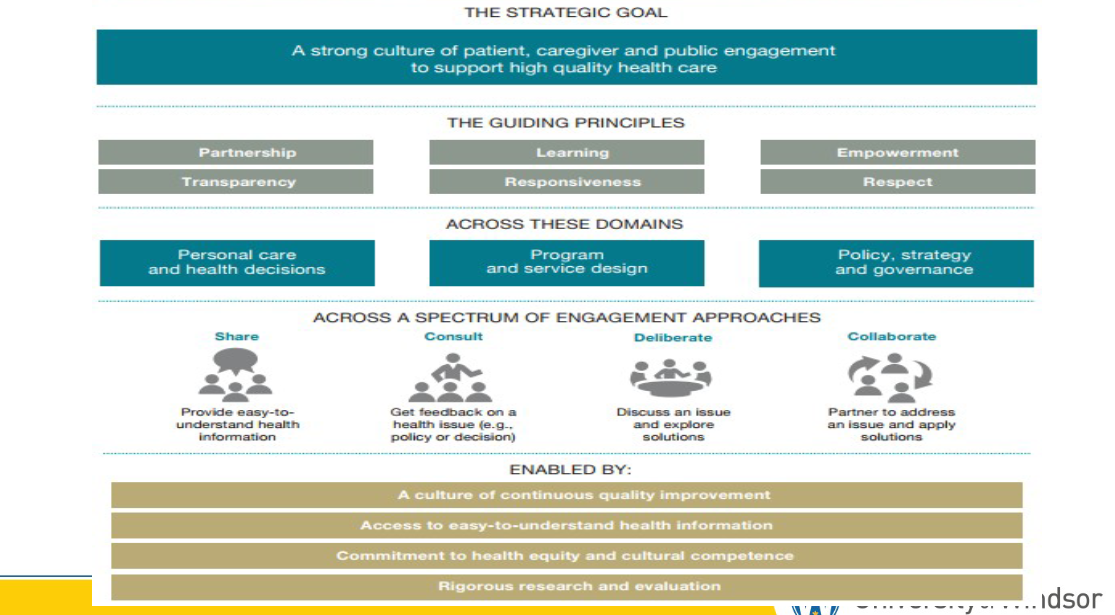
Strategic goal for hc graphic
Safer Healthcare Now
Canadian version of 100,000 lives campaign, using same 6 interventions: rapid response teams, improved MI care, med reconciliation, preventing central line infections, preventing surgical site infections, preventing ventilator associated pneumonia
HQO- health quality Ontario
provincial agency that advises government and providers strategies to support high quality care, received mandate through the ECFAA - excellent care for all act, identified 6 elements of quality care- Safe, Effective, Patient Centred, Efficient, Timely/accessible, Equitable
guiding principles for successful engagement
partnership (btwn hc staff), learning (about other perspectives), empowerment (ppl need to feel empowered to express their own thoughts), transparency (disclose all mistakes, good or bad), responsiveness (respond to needs), respect (for patients and others you work with)
Patient safety linked to?
Quality (they go hand in hand)
systems thinking and quality improvement
SYSTEMS THINKING AND QUALITY IMPROVEMENT - tools for this: health care systems are highly complex (systems thinking, many staff and choices, look in bigger picture), safety analysis or safety improvement techniques such as RCA (root cause analysis) or FMEA (failure mode and effect analysis), RNAO toolkit for best practice implementation, human factors (incompatibility btwn ppl, tools and environment), interdisciplinary teamwork and communication
Lean six sigma in healthcare
LEAN- make overall processes more efficient by eliminating waste (organising stock room so supplies are more easily to find)
QUALITY- manage care processes by standardising and controlling them (standards of care)
SIX SIGMA- make processes more effective by focusing on eliminating defects (why are people falling- recognise deficits)
HQO (quality improvement framework)-
get started, create team and determine goals and timeframe
define problem, analyse info, explore problem from multiple viewpoints
understand system, collect and analyse data gathered, learn abt performance of system and identify barriers and areas of improvement in system
design and test solution, try new things, creative in planning, test using Plan-Do-Act cycles
implement and sustain changes, incorporate into everyday practice, monitor to ensure it is effective
spreading improvement
HQO
health quality ontario- brings transparency into hc so ppl can see flaws
HQO QI themes
team development- work together and cooperate
voice of the costumer- incorporate pt voice
implementing and sustaining change
change management
measurement- methods for gathering info and promote long term sustainability
patient engagement
patient centred, meet their unique needs, individualised and applicable, get to know pt, family goals and context, listening, learning and empowerment important bc- improved pt experience and self management, better health outcomes, decreased cost of care
direct care- what care works for patient?
Program/organisational level- how should care be designed for patients similar?
System level- what services should be available for whom in what way?
model for improvement
PDSA- Plan Do Study Act
What are we trying to accomplish?
How will we know that a change is an improvement?
What change can we make that will result in improvement?
***these allow for trying an improvement idea before fully implementing change, 90-120 days
PDSA Plan
state purpose of pdsa, 5 Ws
PDSA do
90-120 days, conduct test, document results, challenges etc
PDSA study
alanyse data and study results, compare, summarise and predict
PDSA act
refine change and plan for next test
outcome measures
did QI initiative make an improvement, (wait time or infection rates, voice of pt and costumer)
process measures
is the process or steps for QI initiative being followed (did staff comply? voice of staff or workings of the system)
structure measure
changing and fixing equipment in system
balancing measure
dud QI change cause other problems in the system (increased staff satisfaction but not for patients)
Example
research focus, research abstract, findings, evidence informed practice,
choosing wisely canada
recommendations and guidelines to help with decisions
quality and patient safety
Canadian National Steering committee on patient safety: building a safer system (2002)
quality of care- ability of hc services to increase likelihood of desired health outcomes, incorporates accesibility, effectiveness, efficiency, patient safety, patient centred care, equity, efforts to reduce and prevent unsafe acts, use of best practice for best outcomes
adverse events
an event or circumstance that could have or did result in unnecessary harm to a patient (could have been preventable)
most common errors
medications (biggest issue), transfusions, surgeries, restraints, falls, burns, pressure injuries, patient mix ups
adverse event
harmful incident, near miss, no harm incident
stopped at 5 goals of the Canadian quality and patient safety framework
people centred care
safe care
accessible care
appropriate care
integrated care
just culture
in some healthcare cultures- safe care is a core value, increases knowledge and skills, opportunities to improve are embraced, justice, shared commitment, interest of both patients and providers are protected, aims to make system idiot proof and doesnt blame workers
nurse’s responsibility in just culture
patient safety culture, work in teams, communicate effectively, manage safety risks, optimise human and environmental factors, recognise and respond to adverse events, ensure own safety, be aware of common precautions, critical thinking during pt safety hazard, be familiar with patients
healthcare organisation responsibility in just culture
focus on performance improvement programs, act on risk management findings and safety report, provide reliable and current technology, integrate evidence informed practice into procedures and policies, design safe environment and atmosphere, provide continuing education and access to resources
ppl responsible for patient safety
acedemics, professional organisations, provincial government, federal government, healthcare professionals, support staff, patients and families
factors influencing safety
patient and provider factors, task factors, technology factors, environmental factors, organisational factors
systems thinking and quality improvement
core principle: multiple factors involved in failure, errors are caused by systems and are complex, not just caused by one person FINISH, systems can be engineered (bar code scanner) or people dependant (2 patient identifier), policies and procedures depend on individual attention
swiss cheese model
each slice is a barrier put in place to stop an error, holes represent weaknesses in barriers, holes are continuously moving, when holes line up- hazards find their way to patient, termed active failures
safety analysis or safety improvement techniques
RCA- root cause anaylsis
FMEA- failure mode and effective anaylsis
Lean Six sigma
RCA-
RCA- root cause anaylsis, go into past to determine issue
FMEA
FMEA- failure mode and effective anaylsis, anticipate future issues and engineer solutions and safeguards
Lean 6 Sigma
eliminate waste, eliminate defects
human factors
address incompatibility btwn ppl, tools, environment, improves human performance
interdisciplinary teamwork, communication and feedback
teamSTEPPS used to improve communication and teamwork, program developed to provide team with teechniques and trategies to support teamwork FINISH
nursing knowledge base
experience with care, nursing and scientific knowledge, practice standards, critical thinking
Patient safety organisations
CPSI, HQO, Accreditation canada, canada’s hand hygeine challenge, CIHI, institute for health improvement
patient safety reporting
when actual or potential adverse event occurs, confidential report, organisation can identify pattern or trends, focuses on root cause, undergrad students will complete incident report for hospital and academic institution
staff safety
environmental risks, ipac, violence
patient safety top risks
falls, procedure related accidents (wrong person (med, surgery etc), equipment related accidents (malfunction, misuse or electrical hazards)
fall risks
age, history, mobility risks, patients attempt to get out of bed, hip fracture is serious injury, extend length of stay and increase risk of other complications
nursing interventions for patient safety
assessent and patient communication, staff assignmnets, signage, improved patient hand offs, nursing comfort and toilet rounds, involves patient and family
potter and perry 877-878
risks per developmental stage activity
individual risk factors
lifestyle, impaired mobility, sensory or communication impairment, lack of safety awareness
safety during assessment
health history, pt home environment, health care environment, risk for falls, risk for medical errors, patient expectations
health promotion passive vs active strategies
passive- implemented through public health or government legislative interventions
active- individual is actively involved through changes in lifestyle and participation in wellness programs
fall prevention interventions
safety bars near toilets, non slip footwear, educate on assistive devices, use of restraints, side rails or bed alarms, frequent nursing rounds
restraints
physical, chemical or environmental means of controlling individuals behavior, controversial, understand legal factors, require psychological adjustment for pt and family, could lead to patient injury
side rails
may increase pt mobility and stability in bed or during transfer, keeps pt from falling, are considered restrain if pt can’t operate them, could cause injury
precautions
electrical hazards, seizure precautions, radiation safety
what is a theory
purposeful set of assumptions or propositions that identify relationships btwn concepts, provides systematic view for explaining predicting and prescribing phenomena
what is a nursing theory
knowledge abt nursing organised for nurses to use in a professional and accountable manner, perspective for viewing clients situations, a way to organise data, and a method of analysing and interpreting information, theories are one aspect of disciplinary knowledge and create visual linkages to how inquiry is approached- view client situations, organise data, analyse and interpret information, bring about coherent and informed nursing practice
Table 5.1 terminology
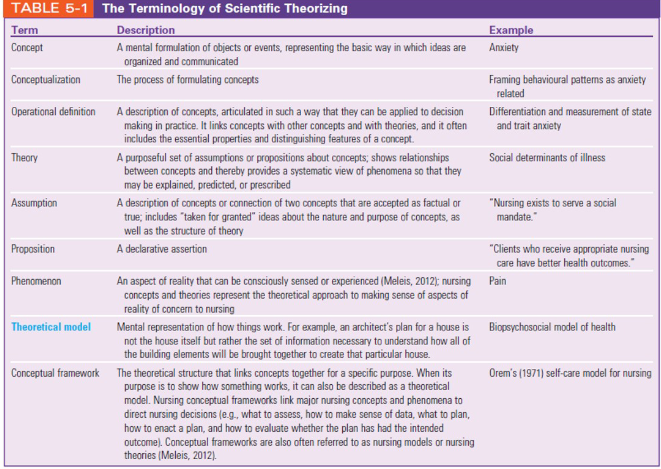
theoretical model vs conceptual framework
theoretical- someone tells u steps to make a basic cake, basic steps
conceptual framework- being able to make a variety of different cakes, specific variations
emergence of nursing theory
Nightingale created early theoretical and conceptual model for nursing
nursing science- unique body of knowledge abt the practice of nursing
Florence Nightingale
modern nursing practice, formalised what nursing looks like as a profession and discipline, descriptive theory- provided nurses witha way to think abt nursing practice in a frame of reference that focuses on patients and environment, created systems for nursing education and practice,
since Nightingale- nursing practice has paralleled that of authority of women in society, after ww2- major developments in science and technology influenced healthcare including nursing, from then- nursing science came into its own and became a unique body of knowledge
nursing theory class inn 1960
led by nurse educators, (used to be led by physicians until 1960),
change → answering theoretical and philosophical questions
what is focus and scope of nursing? how is nursing different from other hc? what is appropriate disciplinary knowlege for nursing? conceptual frameworks, scientific language in dissemination
Ida Jean Orlando
developed problem solving approach known as nursing process (ADPIE)
the conceptual frameworks
goal is to understand how effective nurses systematically organise knowledge about nursing to understand individual pt’s situation, frameworks and models depict theoretical structures to help nurses grasp clinical situation within larger context, often referred to as nursing theory
nursing metaparagigm
called the worldview in context of nursing theory, metaparadigms are the most general statement of discipline and functions as a framework in which the more restricted structures of conceptual models develop. 4 concepts used frequently in relation to others, each nurse theorist’s definition varies by their orientation, nursing experience and different factors, person is main focus, by each theorist defines nursing metaparadigm uniquely
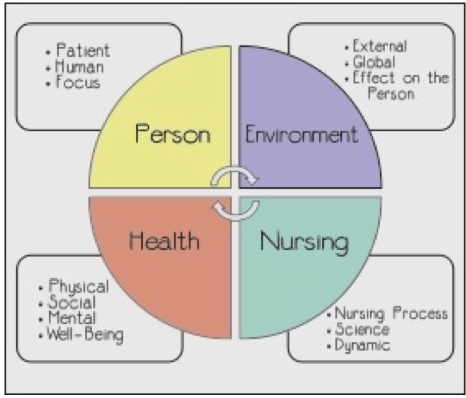
metaparadigm- person
public health/community health nurses, intervene with communities, families, individuals and populations, each have physical, psycological, social, spiritual and cultural characteristics, recognise empowerment as active process
metaparadigm- health
basic resource for everyday living, pblic health/community health nurses participate as active parteners with communities, families and individuals, everyone has the right to information to base decisions and essential healthcare
metaparadigm- environment
nurses are proactive, leaders in promoting public health policy, vulnerable to nature of environment, aware that many variables affect health
metaparadigm- nursing
nurse attributes, characteristics and actions provide care on behalf of or in conjugation with the client, goal of nursing theories is to improve patient care
Imogene King’s theory of nursing (go through summaries instead)
theory of goal attainment - maintain health so ppl can function in their roles, focuses on aiding nurses in pt nurse relationships and helping pt meet goals for their health
person- patient is a social being with 3 needs (need for health info, need for care that seeks to prevent illness, need for care when pt is unable to help themselves)
health- involving life experiences of patient and also takes into consideration the internal and external environment
environment- background for human interactions involves internal environment which transforms energy to enable people to adjust to external environmental changes, which is formal and informal organisations
nursing- considered part of patient of environment
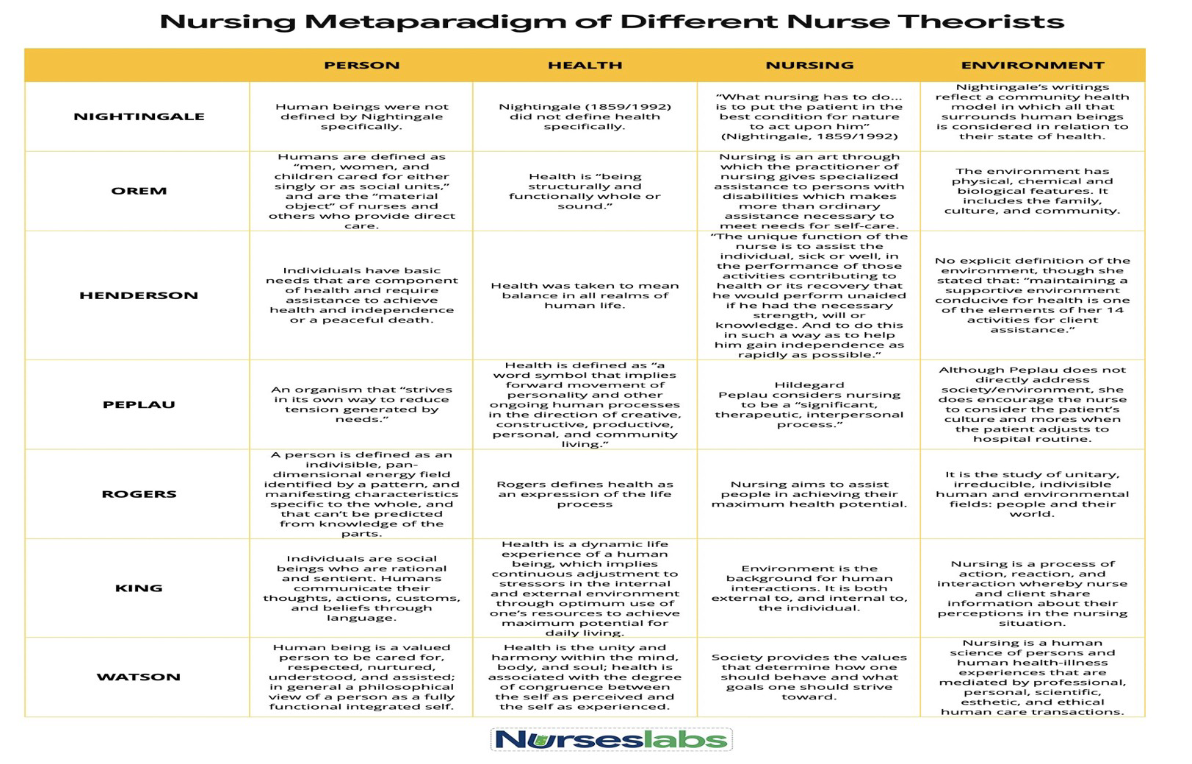
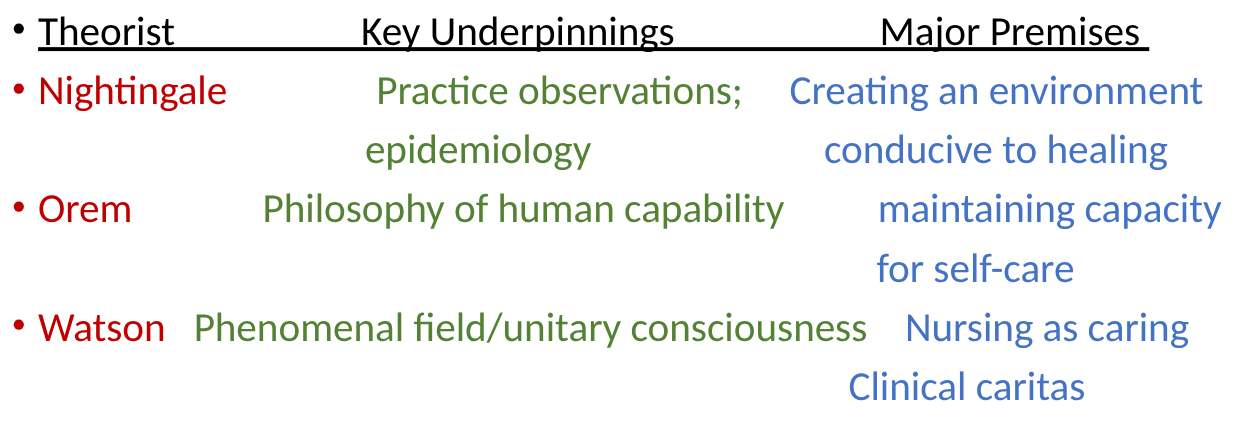
different nursing theory charts- Nightingale, Orem, Henderson, Peplau, Rogers, King, Watson
theory evolution types
grand theory
middle range theory
descriptive theory
prescriptive theory
***some theories work together
nursing theory evolutions
when nurses first began developing frameworks and models, nurses understood the process of building a knowledge base as a matter of science and discovery
grand theory
abstract phenomena, bunch of aspects, broad, conceptual framework, provide structural framework and sometimes called paradigms
martha rogers- theory of unitary human beings- views nursing as both science and art, purpose of nursing is to provide health and well being, believed that patient cannot be separated from the environment
middle range theory
looking at one specific phenomena or concept, limited scope, less abstract,
orems theory - adaptation model of nursing- viewed person as a biopsychosocial being in constant interaction with a changing environment- depicted 4 models of adaptation
descriptive theory
describes why phenomena occurs and describes consequences of it, can be interrelated with the concepts of grand or middle range theories, often considered first level in theory development with aim of detailing components of a nursing phenomenon
ex- nightingale said that ppl were getting more sick bc of the dirty environment
prescriptive theory
stupilates what people must do to attain a goal, uses actions
wiedenbach’s prescriptive theory- multiple realities in which a person exists, depending on the reality of the pt you see- your nursing interventions are different
ways of knowing- barbara carper 1978
nursing is not only science (empiric) byut also art- ethical, personal and aesthetic knowing,
later, theorists added- sociopolitical knowledge, emancipatory knowledge and critical thinking
model bashing
frustration resulting for overly formal and rigid approaches- How does a nurse organise and make sense of all available knowledge and apply it intelligently to the challenges that arise in an individual clinical case?
begin to recognise that older theories are philosophical statements- started to categorise theories as 2 different paradigms
paradigms debated
nursing as art and science, practical and applied, totality paradigm frameworks, simultaneity paradigm frameworks
how was the nursing diagnosis formed
bc conceptual framekworks were less explicit abt how to plan, implement and evaluate nursing care- clinical judgement relating to actual or potential health processes- discrete focus of theorising about nursing care
major theoretical models (+ example)
practice based theory, needs theories, interactionist theories, systems theories, simultaneity theories
practice based theories
theory to improve nursing practice, (prescriptive theory), can draw inspiration from theory,
ex- florence nightingale, dr moyra allen, mcgill modell
needs theories
conceptualising patients as collection of needs, common thinking in 1960s
ex- maslows hierarchy of needs, henderson (14 basic needs, self care theory), orems theory (ways ppl are responsible for meeting the following universal self care requisites)
interactionist theories
look at relationships btwn nurse and client
ex- peplau (described relationship as interactive and therapeutic), joyce travelbee’s human to human relationship model (nurse must provide hope to pt, communication), evelyne adam (nurse respects pt, nurse supports pt strength, knowledge and will)
systems theories
identify subsytems and systems that work together to create a whole, (grand theories)
ex- dorothy johnson (individual is behavioral system with seven subsystems, if one system doesn’t work- dont neglect other systems), UBC model for nursing (individuals made of 9 subsystems), neumans model (looks at stresses and how u react to them),
simultaneity theory (martha rogers)
presents client not just as a person, but in constant interaction with the environment,
ex- Parse theory (person not seen as individual), Jean watson (caring- caritas- how a nurse provides care)
simultaneity vs totality
both are paradigms
totality- views human-universe relationship as cause and effect, considers mind body and spirit as separate entities
simultaneity- human-universe relationship is a mutual process, as entities recognised through patterns
theorising in the future
nursing theories advance over time and build on each other, brings old and new concepts together, shapes concepts into new configurations- adds meaning to human experience
what is community health nursing
a model of care, occurs outside of traditional healthcare facilities, challenges include: social lifestyles, political policy, economic initiatives (not as well funded as acute care)