Psychotherapy
1/55
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
56 Terms
Introduction in first lesson - basic info
It’s basic and necessary for the therapeutic process. It is complicated, as it may set the tone for the client’s motivation to continue therapy.
it can be done as an interview or by filling out a printed form.
You should avoid words like “problem” and “why”.
Goal of intake/ initial psychotherapy interview:
These goals might also happen later on
Deciding if treatment is needed and what type
Building relationship
Gathering data to understand the patients’ problems
Formulating a treatment plan
Motivate the patient to cooperate and come to the next sessions
Gathering the patients history information?
Setting for intake/ initial psychotherapy interview:
You need to prepare the room/yoursel
The placement of the chairs (not exactly across from each other). It’s also best if they are comfortable.
noise should be avoided
avoid hierarchical elements in the room
placement of the clock
Examine any available information regarding the patient
How to behave in intake/ initial psychotherapy interview:
In a pleasant, personal way
Shake the client’s hand
Don’t keep the client waiting, be ready on time
Observe the client’s behavior from the first moment
Your body language should be open and inviting
Avoid scientific jargon
You should start with small talk.
How should first interview/intake start
The patient might start with important information right off the bat- you should be prepared
You should:
listen carefully
observe
guide the patient through storytelling. Don’t ask specific questions as it can interfere with his thinking process.
Sentences to start first interview/intake with:
„What brings you here at this time?“, Can you tell me about that?“
What brings you to see me today?
Can you tell me what has been troubling you?
How it is it that you decided to make this appointment?
„I just want to hear about what´s happened, so that I can best help you to feel better and understand your situation“
„Let´s start from the beginning“
For anxious patients, a subtle comment about anxiety could help them talk about worry. You should start with simple facts about their lives to ease them into therapy.
What are the steps of first interview/intake
preparing the setting
First contact with the client
Starting the interview
Introduce yourself and your therapeutic orientation (cost, length, frequency, rules, goals)
Data gathering process - the patient’s subjective perception of the problem, the current illness, the history of the illness (times with/without), past history of symptoms, and personal history.
Finish session-
10-15 minutes prior to the end, inform the client.
Also, summarize important info from the session.
Give the client an option to comment on the session and ask anything.
Determine the number of sessions and the date for the next one
Decide whether to refer to a psychiatrist/another therapist
Three fundamental components of interview
Building the relationship and responding appropriately to the patient’s emotions (relational skills) - building RAPORT
Collecting all relevant data to understand the patient’s problem (data-gathering skills);
Educating the patient about her illness and motivating him to adhere to treatment
(information-giving skills, negotiating and motivating strategies).
Examples of useful question in sessions
Self-Reflection questions-
“How would you describe yourself to others?”
“How do you think your partner would describe you?”
“What’s the easiest/hardest for you in relationships with others?”Questions about resources -
“Have you experienced something similar in the past? How did you cope with it?”Questions about the solution -
“What will it look like when the problem is resolved?”
“Describe signs indicating the problem has resolved.”
“What part of that have you already accomplished?”
“Is there someone who can help you?”Exceptions from the problem-
When do you feel better?
What is different then?
How many percentages of your life is the problem?
In Session Techniques
Summarizing - Verbal summary of the info gathered so far. We should get feedback from the client, whether we understood it well. It helps structure the interview, build rapport, and put thoughts into order.
Paraphrasing - Helps simplify and bring us into focus. It can also encourage the client to elaborate. We choose the most important detail and communicate it back in his wording.
Clarification - “What do you mean by?…”
Facilitation- “Hmmmm” “I see, Yes..” “Please go on”, nodding. Makes the patient feel understood and encourages him to say more. Also shows listening from our side.
Passive listening (Science)- Use of waiting time and brief silence. It helps encourage the client to speak. It also helps the patient to have a moment when he’s overwhelmed by deep emotions.
Reflections - The therapist mirrors the client's emotional experience or underlying feelings. It allows us to check if we understood his feelings correctly, allowing him to be more aware of his inner feelings.
Literal meaning of psychotherapy
Treatment for the mind.
The difference between psychotherapy and just talking
Conducted by a trained proffesional
WIthin a set framework
It’s done in order to improve the patients mental and emotional health
Specific and non specific factors in psychotherapies
Nonspecific- Common to all psychotherapies and is the foundation for the patient’s improvement.
Studies show that these factors are the main cause of change in therapy.
Specific - Intervention techniques that are unique to the type of therapy.
These are important in the whole treatment, but critical in the early stage.
These factors help engage patients and strengthen the technical components of treatment.
Non- specific factors
Positive expectations - The patient expects some positive change in their lives.
High expectations add to the effectiveness of treatment.Therapeutic relationship - A strong therapeutic alliance helps treatment in these ways:
A. Precondition to change
b. Process of change
C. Content to change.
It is essential in Rogers’ therapy, and considered unimportant in radical therapies. In psychoanalysis, it is regarded as content to consider.Hawthorne effect - Special attention to the client can help him improve.
Raising Consciousness - It is done by giving the patient feedback and education.
Catharsis - Experiencing emotions as a personal relief and behavioral improvement. We help the patient access deep and dark emotions.
Type of people who come to therapy:
Visitor- Came because others requested it (court, insurance, employer).
He doesn’t believe he has a problem, only that others have a problem with him.
He is not invested in the change and has no motivation for it.
Complainer- He is aware of the problem and affected by it, but doesn’t see himself as contributing to it.
Customer - Ideal patient. Ready and willing to solve the problem.
He is open to new ideas, prepared to change.
The role of the therapist in the alliance:
1. Must genuinely relate - Being authentic and allowing the patient to see him as a human being. it includes supporting nonverbal behavior, matching words and behavior, spontaneity, and role modeling.
2. Must relate with unconditional positivity- Showing the patient respect and that his words are valued. It includes commitment, a nonjudgmental attitude, and displaying warmth.
3. Must be accurately empathetic- to be able to understand experiences from another person’s point of view. Asking questions respectfully is seen as a validating response.
Stages of change in therapy the client goes through
Precontemplation- there is no intention to change behavior in the foreseeable future. The patient is unaware or under aware of his problem. Probably pressured to come to therapy.
Contemplation - There is a problem, maybe I should do something, but I’m not sure. It takes a lot of time and effort to overcome this, and also there are benefits to this “problem”.
Preparation- There’s intention and behavioral criteria. Individuals in this stage are intending to take action in the next month and have unsuccessfully taken action in the past year. There is a reduction but not full remission of behavior.
Action- Individuals modify their behavior, experiences, and/or environment in order to overcome their problems. The action takes a lot of time and energy and extreme, and visible, behavioral changes.
Maintenance - hardest to stay at. You need to prevent relapse.
Emotional grounding technique
These techniques allow for more intense perception of physiological manifestations of the body. It reduces emotional flooding and achieves stabilization . "Blocked breathing" - allow to breath.
Focus on emotional or physical needs at that moment.
gaining control of heart palpitations- breathing
"54321" -Name 5 things they can see. Name 4 things they can feel. Name 3 things they can hear. Name 2 things they can smell. Name 1 thing they can taste.
This engages the five senses to anchor them in the present moment and divert attention from distressing thoughts.
Butterfly hug" = bilateral body stimulation - activation of the parasympathetic effect - hug, .. tapping the biceps ...
Secure place imagination
When someone is dissociating
Try to calm him down
Focus on my eyes
Pinch in the face, in the hand, ... (return back to the body)
Get out of the situation (take a few steps to the side) - change position, ...
walk around - feel the movement and the ground under your feet (change body position)
What to assess during psychodynamic therapy session
Defense mechanisms
Resistance (avoidance)
Family History
Symptoms
Focus on patient’s expression of emotions
Dream history, past and present
Transference, countertransference
Interpretation of attachment pattern with mother, romantic partner, therapist.
Psychodynamic therapy goals
The psychodynamic therapy goal is to bring more of our mind to the conscious level.
Becoming aware of unconscious processes allows us to control them.Symptoms and behaviors are the result of mostly unconscious forces.
We want to strengthen the patient’s ability to understand his and others’ motives and the meaning of his experiences, behavior, and relationships.
We wish to help the patient be aware of the inner mechanisms. This will increase emotional awareness and help the person to deal with different pressures in his life .
Using empathy, we want the patient to feel authentic.
Freud Tools
Model of personality
Free association
Interpretation of dreams
Stages of sexual development
Transference, resistance, defense mechanisms
From Freud - The structural model of personality
Id- unconscious impulses that want to be gratified, without regard to potential punishment. It is a source of psychic energy (libido).
Ego - tries to satisfy id impulses while minimizing punishment, guilt. Preconscious.
Superego – the moral center of our personality (somewhat conscious).
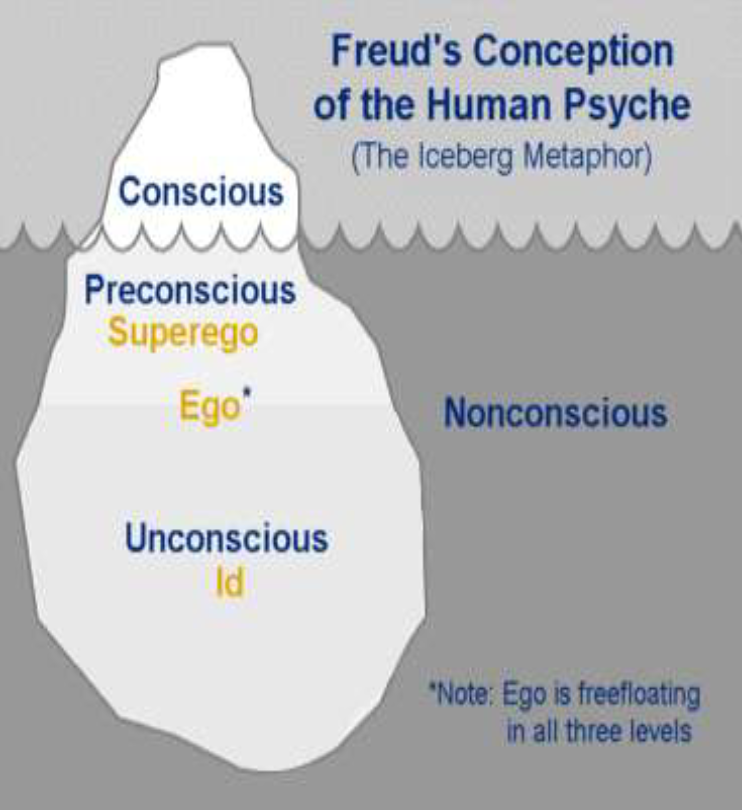
The Unconscious
Invented in 18 century by Friedrich Schelling
Freud believed most of our drives, emotions, and beliefs come from the unconscious.
It hurts our conscious mind
It is reflected in dreams and everyday disruptive behavior, representing that the world is dynamic.
Freud Psycho -sexual theory stages
Oral Stage (1 - 1.5) - The libido is focused on the mouth.
Frustration : dependance on others
Getting fixated: excessive use of oral stimulation. for exampl drikning or eating, cigarrest, gum, biting nails.Anal stage (1.5 - 3) - The libido is focused on the anus. First time there are rules, as they are potty trained.
Getting fixated- can lead to either:
anal-retentive personality- early or harsh toilet training. These people are rigid, obsessively organizedm overly subservient to authoroty.
anal expulsive- Overly passive parent-child interaction in this stage. Leads to limited levels of self control, defiance, hostility, and a messy personality.Phalic stage (3 - 5) - Libido is focused on the phallus- genitalia.
This stage has the Oedipus Complex- the boy wants to hav sexual relations with his mother and sees his father as his rival.Latency stage (7 - 13) - Oedipus conflict has been resolved. there are no developmental events here.
Genital stage(13- ?) - The genitals develop and libido begins to be used in a sexual role. But the feelings for the opposite sex bring anxiety, because they are reminiscent of the feelings for the parent and the trauma that followed.
Current understanding of Freud Psycho -sexual stages
•Early childhood experiences influence our adult personality
•Early experience is an ingredient determining adult personality and later psychopathology
•Psychodynamic theory explains adult personalities and psychological difficulties in relation to our developmental history
•We have a number of memory systems, but episodic memory (long-term) is active from three/ five years old.
Bowlby’s theory- Early childhood experiences affect adult personality. (Attachment theory)
•Babys develops strong bond to their mothers
Between 12-18 months start the separation phase of development, where mother is „secure base“ from whitch the baby can explore world
Relationship to mother represent our internal working model how to relate to others
Secure- The world is safe. I am effective at getting my needs met. Mom is there when I need her.
Avoidant: The world is dangerous. Relationships can’t help. I have to manage on my own.Resistant: The world is dangerous. I can’t cope alone. I must keep mom focused on me.
Disorganized: The world is very dangerous. I don’t know what to do! Nothing I try makes me feel safer.
Defense Mechanisms
Sigmund Freud describes how the Ego uses a range of mechanisms to handle the conflict between the Id, the Ego and the Super ego'.
Defense mechanisms develop early in childhood to manage challanges and cope with discomfort
We can use them consciously, but the unconscious are more interesting for therapy
They can be problematic when they are rigid and unhelpful
They are representations of Coping
Internal conflict
IT is the tension between what we want for ourselves and what others expect from us
It Is our competing wishes
Inner conflict is represented in symptoms
Example from class:
- Layla conflict was wish to merry and not to leave mother alone in town it is in preconscious level. Deeper is maybe conflict that Layla feels responsible for parents divorce)
- Layla should first recognize preconscious conflict and then go to deeeper conflict
Resistance- definition
It’s a door to unconscious. If this happens in therapy= the therapy has „struck a nerve“
Resistance and analysis of defense mechanisms IS ESSENTIAL PART OF ANALYTIC WORK
"Resistance" as initially used by Sigmund Freud, referred to patients blocking memories from conscious memory.
Today is more resistance to give up on something, like quitting therapy, giving up on moving forward (Layla resistance to move to Edinburg)
Resistance became when unconsious feeling and thought are to intensive, patien feels anxiety and use resistance to hide it
Specific patterns of resistance
-specific motivations (e.g., wish for power, envy, vengeance, specialness, shame),
-specific attitudes (e.g., entitlement, injustice),
-specifiC defenses (e.g., rationalization),
-specific symptoms (e.g., eating disorders).
-In theraphy – client do not want to talk about some topic; he changet the topic immediately; late to the appointment....
Transference
The patient’s feelings are not really towards the therapist, but are repetitive to earlier relationships.
This is key in psychodynamic therapy.
The patient transfers his inner world into the relationship/expectation with the therapist.
Transference can reflect childhood relationships
the focus in psychodynamic psychotherapy is, in large part, the therapist and client recognizing the transference relationship and exploring what the meaning of the relationship is.
The therapist-client relationship is what drives change.
Counter- Transference
The feeling the therapist has towards the patient, or even cases when the therapist takes on himself the suffering of the patient.
If we don’t recognize and analyze this on time, it could put us into a blind spot and damage progress,
Awareness of this can provide a glimpse into the patient’s inner world and the emotions and reactions he induces in others.
Psychodynamic therapy definition
long-term (>6months) psychodynamic psychotherapy can be defined as a treatment that focused on thoughtfully timed interpretation of transference and resistance and a sensitive appreciation of how the therapist contributes to the interaction with the patient
Different orientations in psychodynamic therapy
The dynamic therapiest decide if the therapy will be oriented toward:
1.Supporting the ego
2.Uncovering the id impulses, uncovering how unconsciou affect real life
3.Changing the external condition in client life
7 assumptions of psychodynamic therapy
1) The problems that people bring to psychotherapy can be usefully discussed in terms of thoughts and feelings.
2) To understand uconscious experiences, we need to refer to other mental states of which the individual is unaware and experience them safely.
- (Dream of Layla)- where are the symbols from unconsciousness
- Dream about beginning the journey (represent start the therapy )
3) interpersonal relationships, and early chilfhood experiences particularly attachment relationships are central to the organization of personality.
Early relations and early experiences determinant our adult personality and psychological difficulties
It is source of our inner conflicts
4) wishes, affects, and ideas will sometimes be in conflict. these conflicts are seen as key causes of distress and symptoms
5) DEFENSES: mental operations that distort conscious mental states to reduce their potential to generate anxiety.
6) Behavior can be understood in terms of mental states that are not explicit in action or within the awareness of the person concerned
7) Orientation to the developmental aspects of their patients' problems (when and how a problem started, how it relates to an idealized "normal" developmental sequence)
Psychosynamic therapy tools
Uncovering – unconscious (dreams)., transference (family history), defence mechanisms
Suporting – strength of ego
Interpreting
Empathy
Listening (free associations)
Resistance -identification
CBT main points to know
CBT has strong empirical support from randomized clinical trials.
1.It is a short-term focused treatment
2. It puts emphasis on current behavior and thinking
3. Behavior isn’t only symptom, it’s a problem
4. Thoughts cause emotion and behavior. Our goal is to help the patient understand how his thoughts determine bith his emotions and his behavior.
5. CBT is a collaborative effort between the therapist and the client.
The clients role is to:
define goals
express concerns
learn
implement learning
The Therapist role is to:
Help client define goals
listen
teach
encourage
CBT teaches how to remain calm or at least neutral when face with difficult situations. It teaches you new, better behavior.
It is based on “rational thought” - facts and not assumptions
CBT is structured and directive. It is based on the notion that maladaptive behavior is the result of skill deficit.
CBT is based on the assumption that most emotional and behavioral reactions are learned. Therefore, the goal of therapy is to help clients “unlearn” their unwanted reaction and learn a new way of reacting.
Homework is a central feature of CBT - client learns to use the new skill in his everyday life.
Creating a Contract: how the problem developed, current example, when was it activated, what maintained the problem.
Therapies that fall under the CBT umbrella
REBT Rational Emotive Behavior Therapy
PST Problem Solving Training
RP Relapse Prevention
Dialectical Behavior Therapy
Biofeedback and Neurofeedback
Mindfulness
What kind of problems can CBT help with?
Anxiety and phobias
Substance abuse
Depression
Obsessive-compulsive disorder (OCD)
Chronic pain
Chronic fatigue syndrome
Bipolar disorder
Cognitive of theories in CBT
Information processing model
Working with negative thoughts in psychotherapy
Cognitive interventions
Information processing model
1 .Three step model:
Event—> Cognitions —> Feelings —> Behaviors
It’s not the event itself that causes emotional reactions, but how we interpret it.
2. ABC Model:
Activating event —> Belief —> Consequences
Activating event
↓
Person’s thinking becomes rigid and distorted
↓
Dysfunctional beliefs and thoughts are activated.
↓
Behaviors and self-thoughts become fixed
↓
Specific emotions, behaviors, and physical reactions. (Consequences)
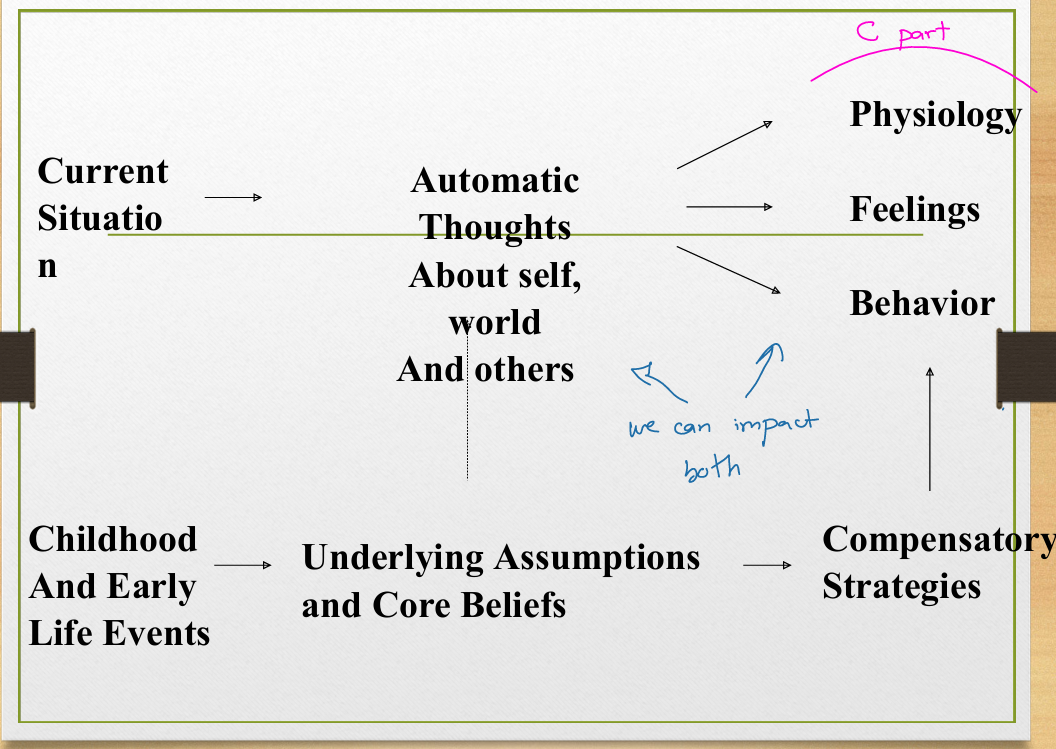
3 . Hierarchical organization of thinking
Core beliefs -
rigid and unconscious.
Usually formed in childhood.
Can be negative/positive.
Example: “I have to be perfect”Underlying assumptions/beliefs- These are conditional beliefs, often in the form of "if-then" statements, expectations, or rules.
Come from and protect Core beliefs.
These are unarticulated assumptions.Negative automatic thoughts-
Come when you are in a stressful situation.
These are immediate, involuntary thoughts in response to everyday situations.
They don’t come from reasoning.
We can impact the automatic thoughts which can change the way we react physically, emotionally and behaviorally.
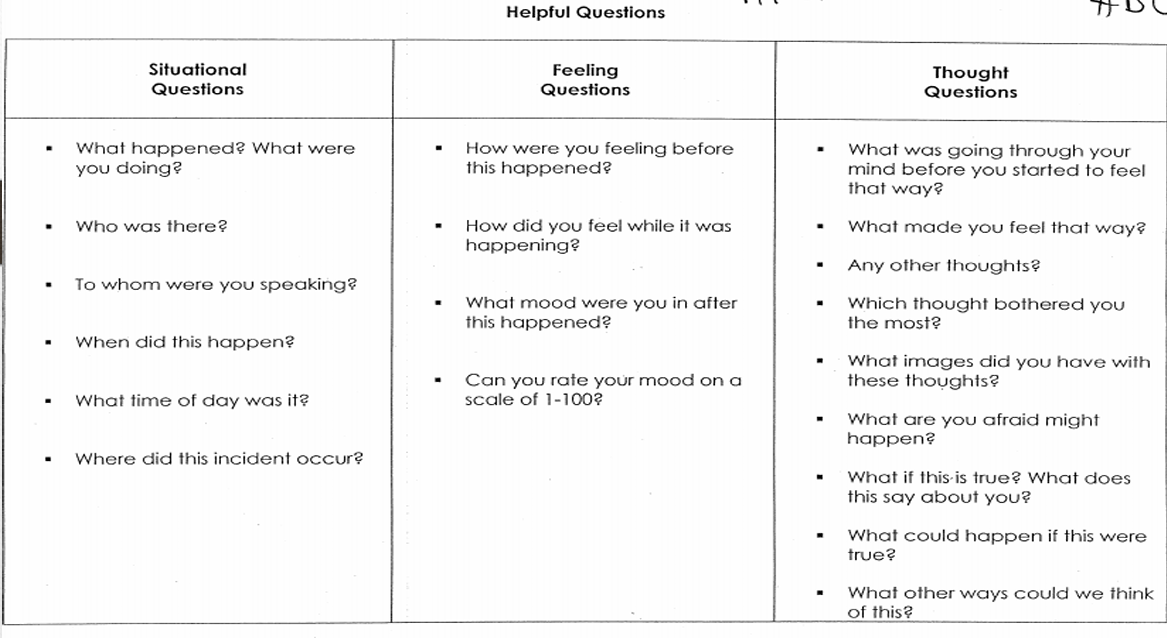
Working with negative thoughts in psychotherapy
Identify the negative automatic thoughts
“what were you telling yourself?”
“what did the situation mean for you?”Modifying dysfunctional beliefs - ABCDE Model
D- Dispute. What evidence is there for and against these thoughts?
E- Effective alternative thought.
What are the alternative ways to think in this situation. Is there any other way of looking at the situation?
What are the implication of thinking that way?
Cognitive interventions
Monitor automatic thoughts
Teach imagery techniques
Promote cognitive restructuring
Examine alternative evidence
Modify core beliefs
Generate rational alternatives
Behavioral theories of CBT
Classical conditioning – Pavlov
Operant conditioning – behavior is a function of its consequence. When behavior is valued ,the person continues this behavior.
Observational Learning (Modeling) – we learn by imitaiton
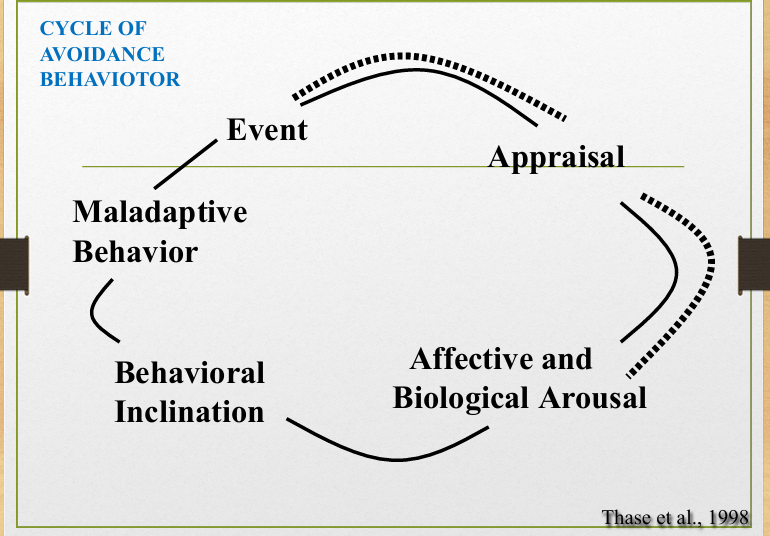
Cycle of avoidance behavior
Event
↓
appraisal
↓
Affective and biological arousal
↓
Behavioral Inclination
↓
Maladaptive behavior
Behavioral Intervantions
• Breathing retraining
• Relaxation
• Behavioral activation
• Problem-solving skills
• Exposure and response prevention
• Social skills training
• Graded task assignment
• Asertivness training
• Systematic desensitization
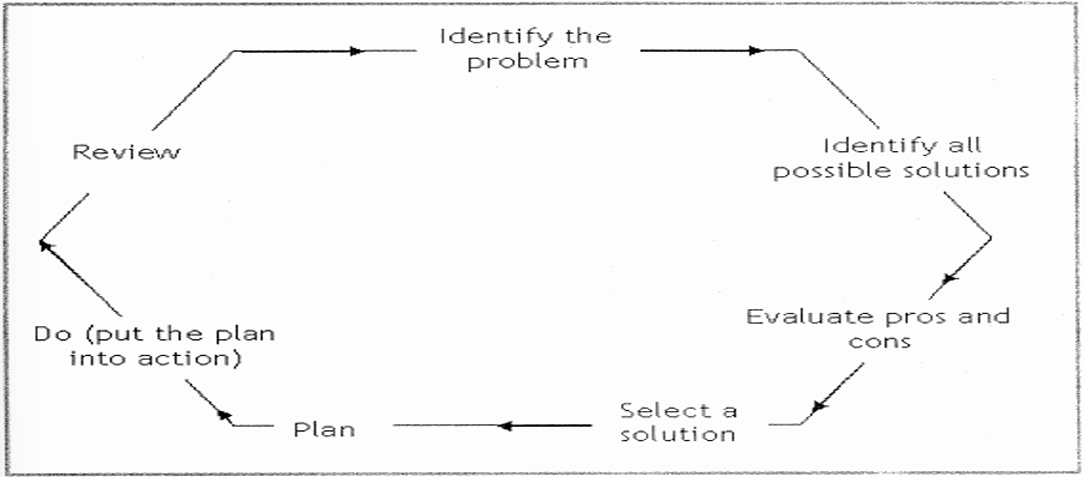
Problem solving technique
A CBT behavioral intervention.
Identify the problem
Identify all possibe solutions
Evaluate Pros and Cons
Select a solution
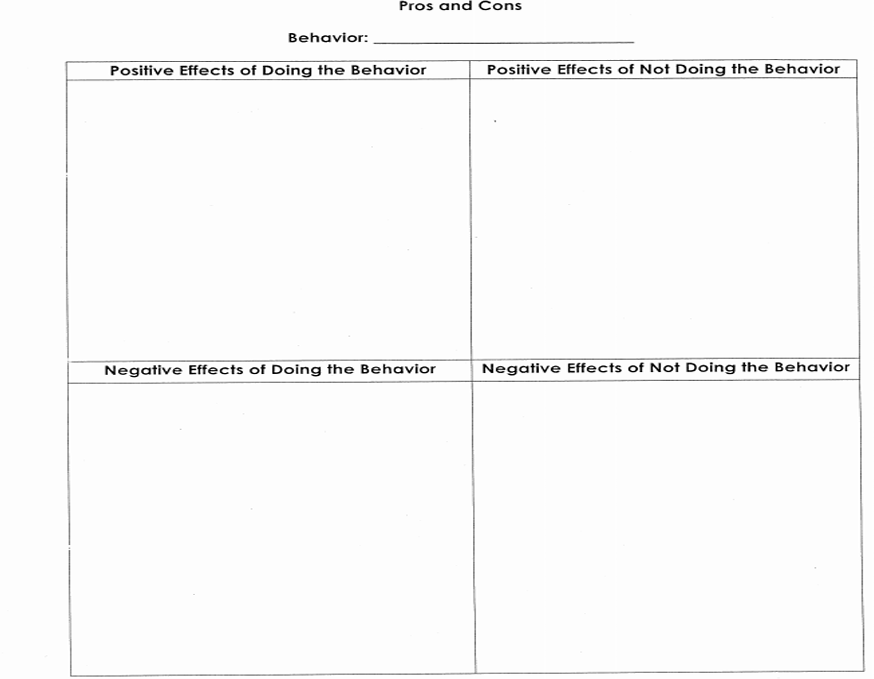
Pros and Cons page
You write a behavior then write:
1. positive effect of doing the behavior
2. negative effect of doing the behavior
3. positive effect of not doing the behavior
4. negative effect of not doing the behavior
Systematic desensitization
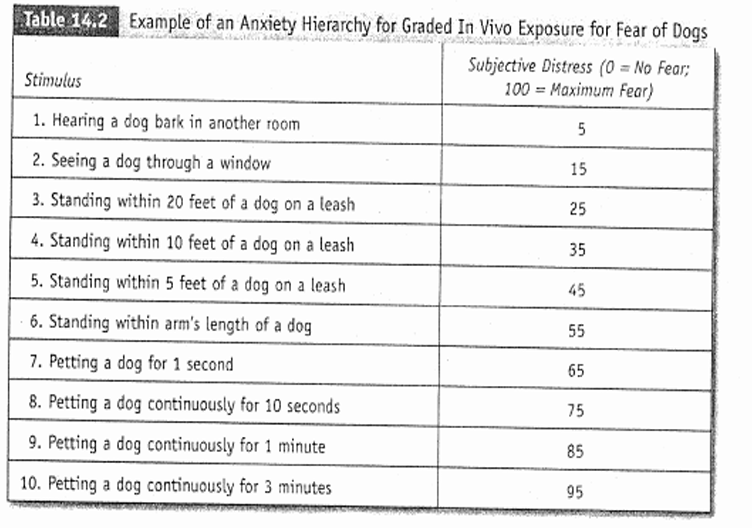
Common component of CBT
Establish good therapeutic relationship
• Educate patients - model, disorder, therapy
• Assess illness objectively, set goals
• Use evidence to guide treatment decisions
• Structure treatment sessions with agenda
• Limit treatment length
• Issue and review homework to generalize learning
Basic principles of CBT
Change mood states by using cognitive and behavioral strategies:
• Identifying/modifying automatic thoughts & core beliefs,
Regulating routine
Minimizing avoidance.Emphasis on ‘here and now’
Preference for concrete examples-Start with specific situation (complete thought log)
Reliance on Socratic questioning - Ask open-ended questions
Empirical approach to test beliefs -
• Challenge thoughts not based on evidence
•Cognitive restructuringPromote rapid symptom change
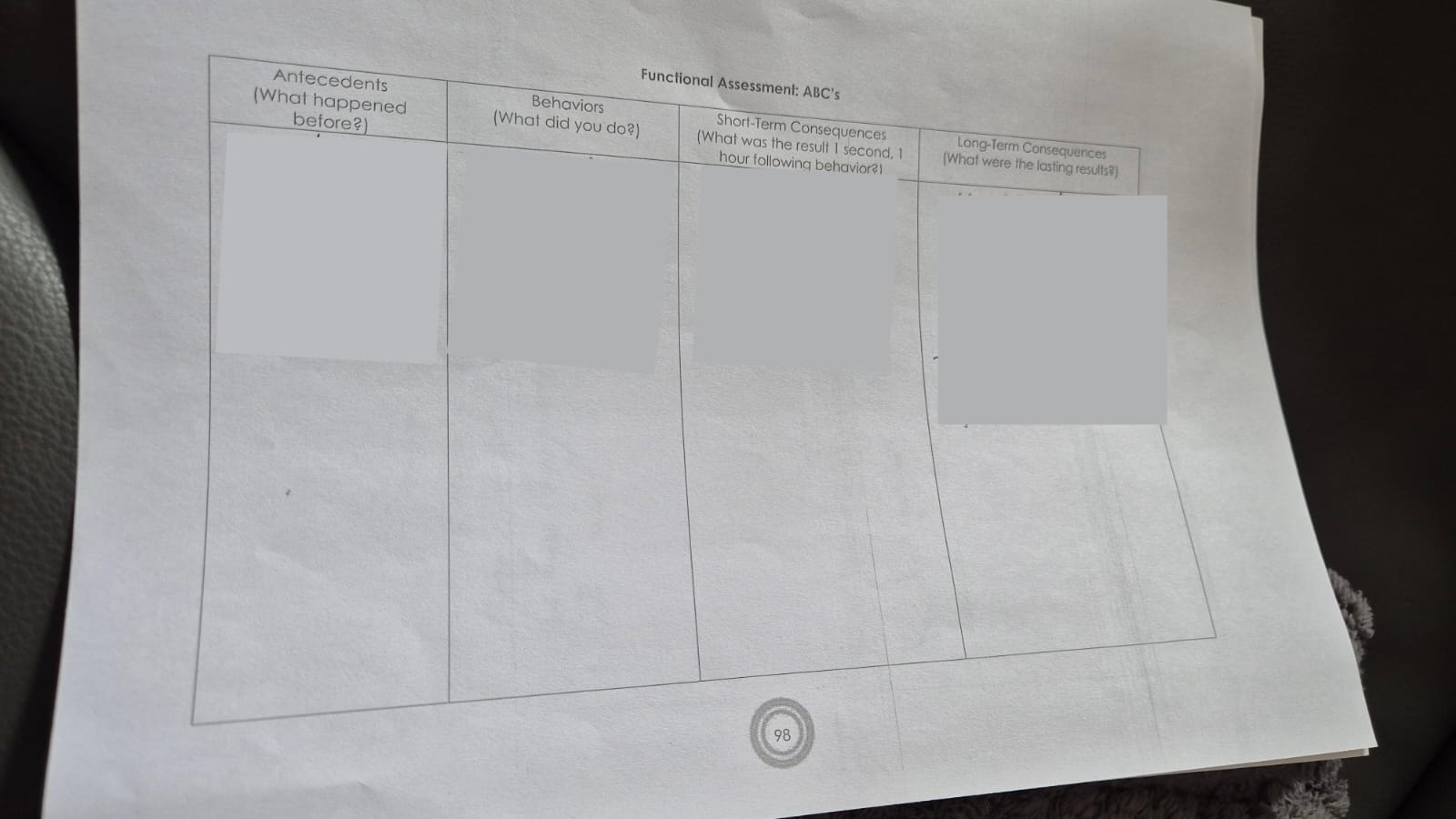
Functional Assessment: ABC’s (sheet)
Antecedent (what happened before?”
Behaviors (what did you do?)
Short-term Consequences (result one hour after behavior)
Long-term Consequences (What are the lasting results?)
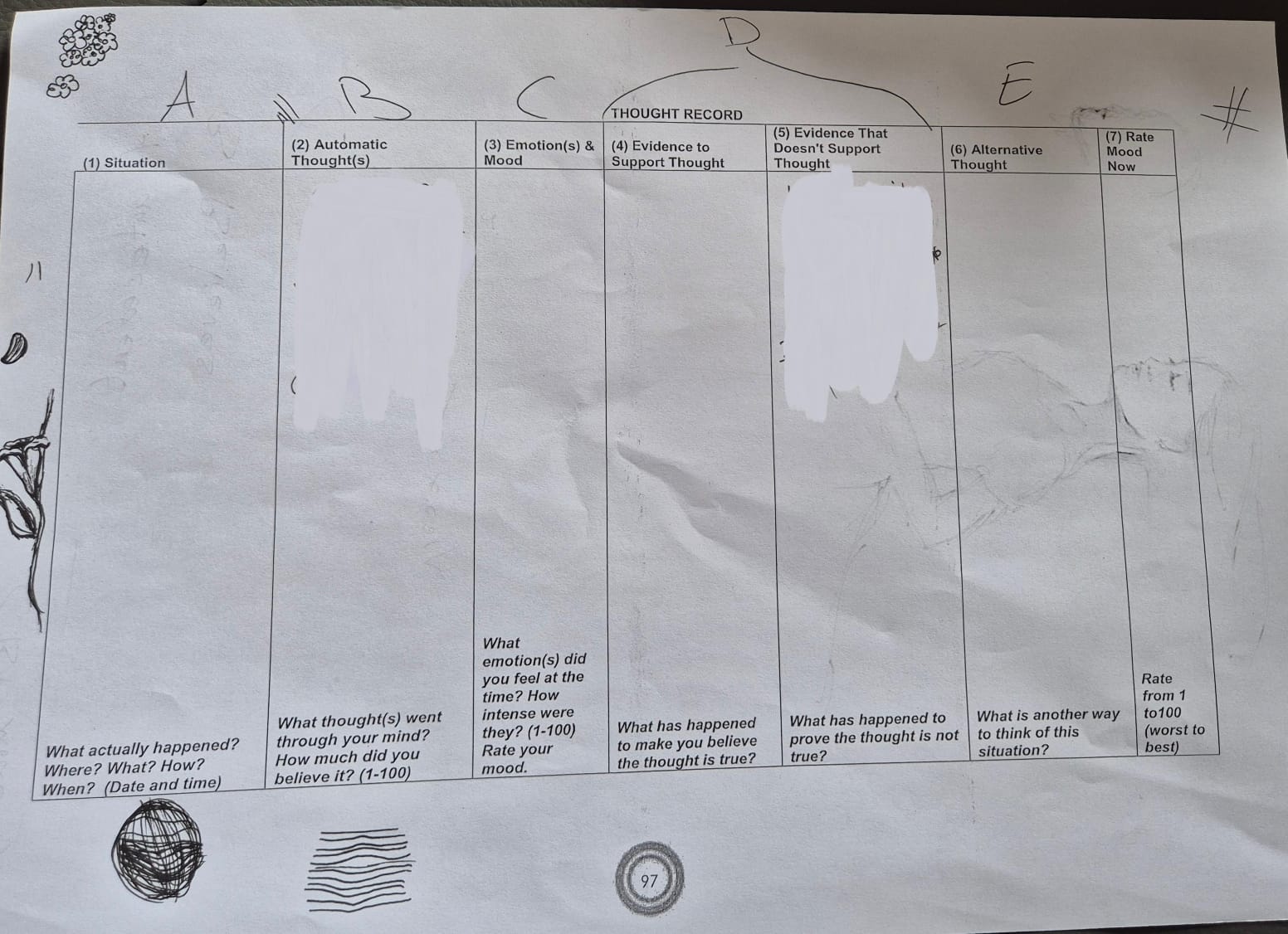
ABCDE thought record
Main point of interview with Kristína Kotrčová
Psychotherapy offers deep, long-term healing by addressing the root causes of psychological problems—something medication or unqualified helpers cannot achieve alone.
Cognitive Distortions types
All-or-Nothing Thinking: Viewing situations on one extreme or another instead of on a continuum.
Ex. “If my child does bad things, it’s because I am a bad parent.”Catastrophizing: Predicting only negative outcomes for the future.
Ex. “If I fail my final, my life will be over.”Disqualifying or Discounting the Positive: Telling yourself that the good things that happen to you don’t count.
Ex. “My daughter told her friend that I was the best Dad in the world, but I’m sure she was just being nice.”Emotional Reasoning: Feeling about something overrules facts to the contrary.
Ex. “Even though Susie is there at work late everyday, I know I work harder than anyone else at my job.”Labeling: Giving someone or something a label without finding out more about it/them.
Ex. “My daughter would never do anything I disapproved of.”Magnification/Minimization: Emphasizing the negative or downplaying the positive of a situation.
Ex. “My professor said nice comments on my paper, so I know I’ll probably fail the class.”Mental Filter/Tunnel Vision: Placing all your attention on the negatives of a situation or seeing only the negatives of a situation.
Ex. “My husband says he wished I was better at housekeeping, so I must be a lousy wife.”
Ex. “My daughter’s boyfriend got suspended from school. He’s a loser and won’t ever amount to anything.”Mind Reading: Believing you know what others are thinking.
Ex. “My house was dirty when my friends came over, so I know they think I’m a slob.”Overgeneralization: Making an overall negative conclusion beyond the current situation.
Ex. “My husband didn’t kiss me when he came home this evening. Maybe he doesn’t love me anymore.”Personalization: Thinking the negative behavior of others has something to do with you.
Ex. “My daughter has been pretty quiet today. I wonder what I did to upset her.”“Should” and “Must” Statements: Having a concrete idea of how people should behave.
Ex. “I should get all A’s to be a good student.”