W11.3 Common Conditions of the Elbow Chart
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
What practice patterns are commonly associated with elbow and forearm conditions?
4c muscle performance
4d connective tissue dysfunction
4e local inflammation
4g fracture
4h joint arthroplasty
4i bony or soft tissue surgery
5f peripheral nerve injury
What is epicondylalgia and why is that term preferred over epicondylitis?
Epicondylalgia refers to pain at an epicondyle and is preferred because the condition is not always a true inflammatory process
What types of activities commonly contribute to epicondylalgia?
Overuse of the arm, especially repetitive rotation with flexion and extension
Which is more common: lateral or medial epicondylalgia?
Lateral epicondylalgia is 4-7x more common than medial epicondylalgia
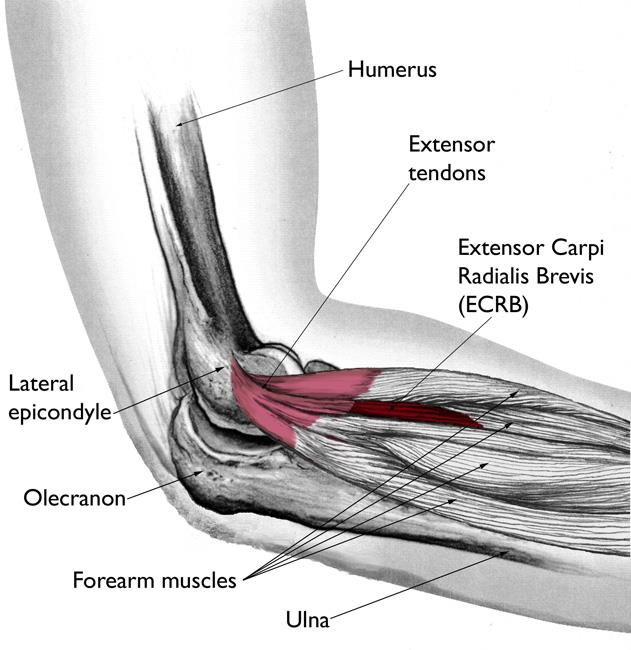
What muscle-tendon structures are commonly involved in lateral epicondylalgia?
ECRB most commonly
Possible involvement of ECRL, ECU, and EDC
What are common aggravating activities in lateral epicondylalgia?
Gripping (with wrist extension)
Such as in tennis, racquet sports, golf, swimming, and weightlifting
What are the typical symptoms of lateral epicondylalgia?
Lateral elbow or forearm pain with extensor contraction
Diffuse achiness
Morning stiffness
Pain with grasping or wrist-extended activity
Dropping objects
What are common palpation findings in lateral epicondylalgia?
Tenderness at the ECRB and ECRL
Especially anterior to the lateral epicondyle and around the radial head
What resisted motion often reproduces symptoms in lateral epicondylalgia?
Resisted wrist extension with radial deviation and the elbow extended
What special tests are commonly positive in lateral epicondylalgia?
Cozen’s test
Mill’s test
Extensor digitorum test
What proximal regions should be assessed in patients with lateral epicondylalgia?
Shoulder
Scapulothoracic region
Cervical spine
Thoracic spine
What is the general prognosis for lateral epicondylalgia with conservative treatment?
Often self-limiting over 8 to 12 months
About 95% recover with conservative management
What are the main exercise priorities for lateral epicondylalgia rehab?
Wrist extensor eccentrics
Elbow isometrics progressing through angles
Isotonic and plyometric loading
Shoulder and scapular stabilization
Cervicothoracic stabilization
Sport-specific technique training
What manual therapy options may be used for lateral epicondylalgia?
Scaphoid manip
Radial head mobs or manip
Mill’s manip
Neurodynamic techniques
Cervical and thoracic mobs or manip
MWM
Cross friction massage
How do corticosteroid and PRP injections differ in lateral epicondylalgia management?
Corticosteroids may help in the acute phase but can be detrimental in chronic cases
PRP is mainly used to stimulate regeneration in chronic cases
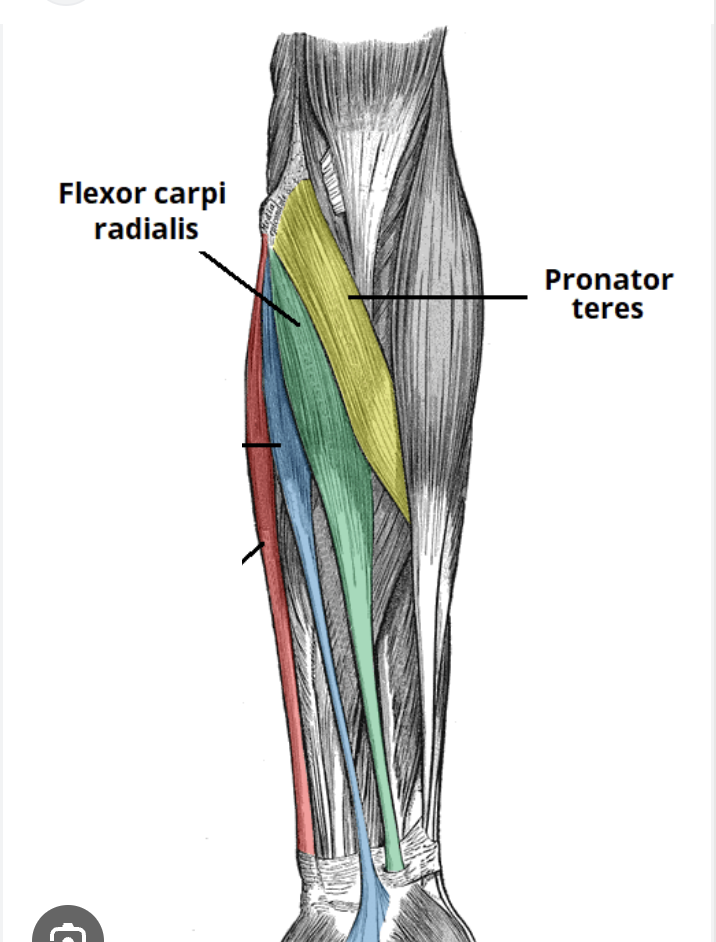
What structures are most commonly involved in medial epicondylalgia?
Common flexor origin
Especially flexor carpi radialis and pronator teres
What is the typical mechanism of medial epicondylalgia?
Overuse injury to the flexor tendons at the elbow with valgus stress
What are the main clinical findings in medial epicondylalgia?
Pain and tenderness over the flexor-pronator origin
Sx with resisted wrist flex or pronation
Sx with passive wrist ext and supination
What special test is used for medial epicondylalgia?
Golfer’s elbow test
Palpate med epicondyle
Elbow flexed to 90
Elbow ext. supinate, wrist ext. → elbow ext
(+) pain at med epicondyle

What important differential diagnoses should be considered with medial epicondylalgia?
MCL insufficiency
Pronator teres syndrome
Ulnar nerve entrapment
Medial intra-articular pathology
What are the main rehab principles for medial epicondylalgia?
Initial rest and activity modification
THEN ROM, strength, and flexibility work
Progressing from multi-angle isometrics → concentric → eccentric exercise
Scapular and shoulder stabilization has to be done
What is the usual mechanism of a distal biceps tendon rupture?
Forceful resistance to elbow extension, usually traumatic
What population is classically associated with distal biceps tendon rupture?
Males
What are the hallmark findings of distal biceps tendon rupture?
Burning sharp pain in the antecubital fossa
Marked elbow flexion and supination weakness
Ecchymosis (bruise) after 48 to 72 hours
A Popeye sign (high peak in bicep) from tendon retraction
How is distal biceps tendon rupture commonly managed?
Surgical tendon repair in young or active patients
What are key post-op rehab considerations after distal biceps tendon repair?
Protocol-driven rehab with bracing and limited ROM for 6-8 weeks
Maintenance of shoulder and hand or wrist function
Control of pain and swelling
THEN progression to stretching, strength, and endurance
Return to unrestricted activity after >6 months
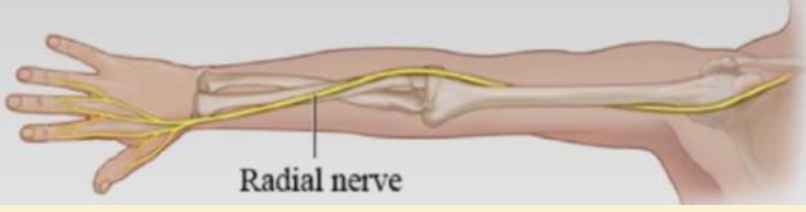
Which nerve around the elbow is most commonly injured?
Radial nerve
What nerve entrapment is most common overall?
Carpal tunnel syndrome
What is the mechanism of humeral supracondylar process syndrome?
Compression of the median nerve under the Struthers’ Ligament
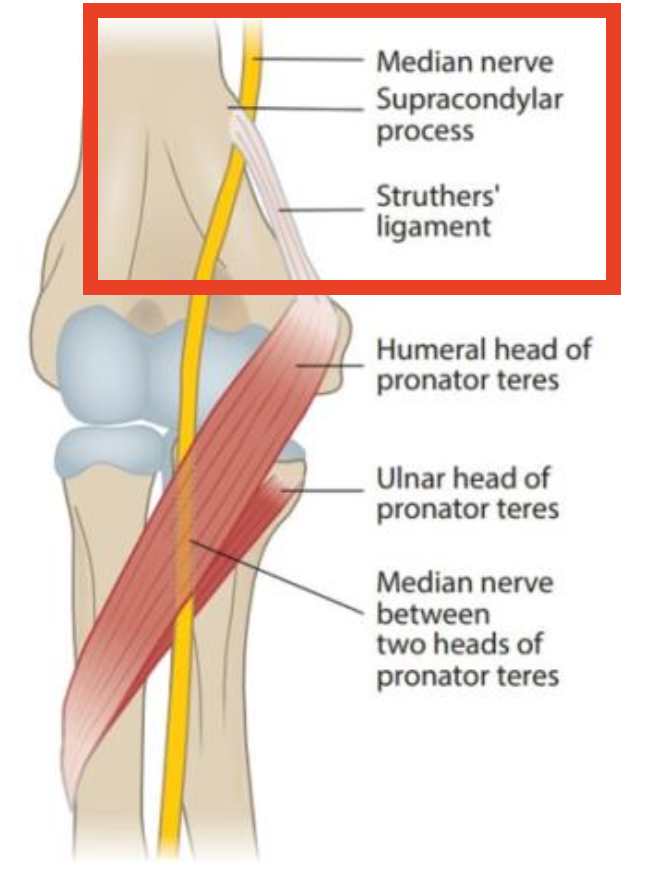
What are typical findings in humeral supracondylar process syndrome?
Pain in the wrist or medial forearm
Worse with full extension or pronation
Paresthesias in the index and middle fingers
What are the functional deficits seen in a high median nerve injury?
Hand of Benediction pattern
Loss of extrinsic flexors on the median nerve side → inability to flex DIP and PIP joints and weakened MCP flexion
Loss of APB function → thumb rests in adduction
When making a fist, the 1st and 2nd digits cannot flex
What is the typical presentation of pronator teres syndrome?
Insidious onset of anteromedial forearm pain or “heaviness”
Pain/paresthesias or sensory impairment in the median nerve distribution
What strength test may reproduce symptoms in pronator teres syndrome?
Pronation strength testing at 90 degrees of elbow flexion
How can pronator teres syndrome be differentiated from carpal tunnel syndrome?
Pronator teres syndrome does NOT usually have:
Tinel’s at the wrist
Nocturnal symptoms
What are key management strategies for pronator teres syndrome?
Activity modification
Relative rest
Ice or anti-inflammatory care
Stretching
Soft tissue mobilization
Neural gliding
Maintaining strength
Scapular and shoulder stabilization
Addressing cervical mobility and posture
What is the defining feature of anterior interosseous nerve syndrome?
Motor involvement only with no sensory loss
What are the key findings in anterior interosseous nerve syndrome?
Weakness in the flexors of the index finger and thumb
Positive pinch test, and no sensory deficits
Which muscles are innervated by the anterior interosseous nerve?
Flexor pollicis longus
Lateral half of flexor digitorum profundus
Pronator quadratus
How is anterior interosseous nerve syndrome usually managed?
Resolves spontaneously
What boundaries form the cubital tunnel?
Floor is the UCL
Ceiling is the arcuate ligament from FCU
Anterior border is the medial epicondyle
Posterolateral border is the olecranon
Ulnar nerve passes through it
What are common causes or contributors to cubital tunnel syndrome?
Repetitive use
Shortened FCU
Ulnar nerve subluxation
Elbow synovitis
Cubitus valgus deformity
Repetitive flexion traction forces
Trauma
Laceration
What are the sensory symptoms of cubital tunnel syndrome?
Activity-related pain or paresthesias in the ulnar nerve distribution
With medial elbow pain, often worse at night
What are the motor findings of cubital tunnel syndrome?
Inability to abduct the digits
Loss of grip power or dexterity
Late atrophy or weakness of ulnar intrinsic muscles
What special tests may be positive in cubital tunnel syndrome?
Elbow flexion test
Tinel’s sign
Wartenberg’s sign
Froment’s sign
ULTT 4
What hand deformity may appear later in cubital tunnel syndrome?
Ulnar claw hand
Caused by paralysis of the ulnar lumbricals and interossei → loss of MCP flexion and intrinsic control of the extensor mechanism in digits 4–5
Unopposed extensor digitorum hyperextends MCPs while FDP flexes PIP and DIP → claw posture
Finger flexion remains intact via FDS and FDP, but full finger extension is impaired due to loss of intrinsic muscle function

What conservative treatment is used for cubital tunnel syndrome?
Activity modification
Elbow pad over the cubital tunnel
Limiting extreme elbow flexion
Night splinting at 40 to 60 degrees
Possibly full-time splinting in more severe cases
Exercises in a limited arc
Stretching the FCU
When is surgery considered for cubital tunnel syndrome?
When symptoms fail to improve after 3 to 4 months of conservative care
OR when there is muscle atrophy, persistent sensory change, or persistent symptoms
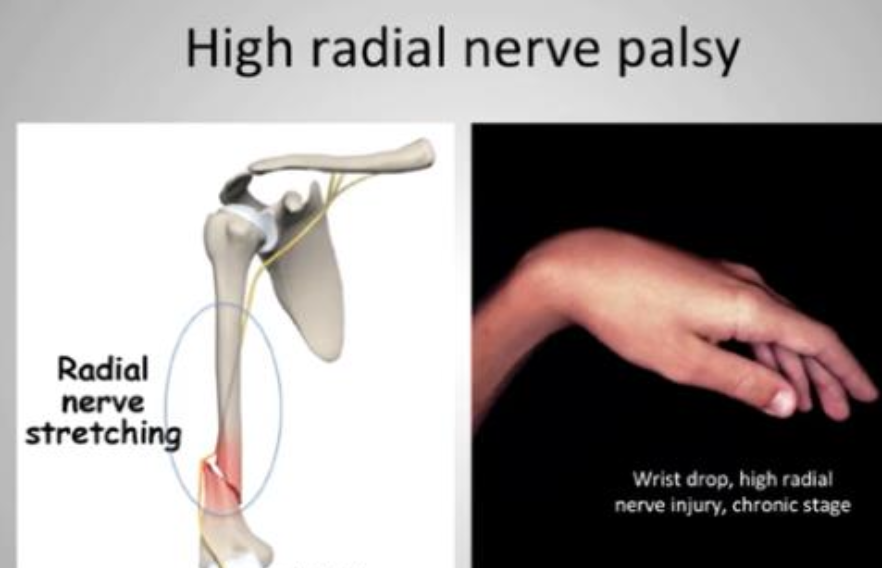
What is the classic sign of high radial nerve palsy?
Wrist drop with extensor atrophy and the hand hanging in flexion
What is compressed in radial tunnel syndrome?
The deep branch of the radial nerve, often by ECRB and the supinator
How does radial tunnel syndrome commonly differ from lateral epicondylalgia?
Pain is usually more distal in the extensor mass and tenderness is about 5 cm distal to the lateral epicondyle
What tests commonly provoke pain in radial tunnel syndrome?
Resisted third digit extension, resisted supination with the elbow extended, and elbow extension plus pronation plus wrist flexion
How is radial tunnel syndrome managed?
Activity modification, splinting in about 45 degrees of wrist extension, extensor stretching, soft tissue mobilization, nerve glides, and surgery if conservative care fails
What is the key distinguishing feature of posterior interosseous nerve syndrome compared with radial tunnel syndrome?
Posterior interosseous nerve syndrome has motor loss without sensory deficits
What motor deficits are seen in posterior interosseous nerve syndrome?
Loss of extension at the MCPs of the fingers and thumb, loss of thumb IP extension, and loss of thumb abduction
What is a common mechanism for UCL or medial elbow instability?
Throwing-related valgus stress, FOOSH, or iatrogenic causes such as excessive medial epicondylectomy
What clinical tests are used for UCL or medial elbow instability?
Valgus stress test at 25 degrees of elbow flexion, moving valgus stress test, and milking maneuver
What findings distinguish complete versus incomplete UCL tears?
Complete tears may show palpable medial gapping, while incomplete tears cause pain without gapping
What are the phases of conservative rehab for UCL or medial elbow instability?
Acute phase reduces inflammation and restores ROM, subacute phase gradually restores ROM and strengthens, and chronic phase builds strength, power, endurance, neuromuscular control, and throwing mechanics
Who is more likely to be a surgical candidate for UCL injury?
High-level athletes and heavy manual laborers
What graft is classically used in Tommy John reconstruction?
An ipsilateral palmaris longus tendon autograft
Why is little league elbow important to recognize early?
It involves a medial epicondylar physeal injury in a skeletally immature athlete and can affect growth if not managed properly
What age group is commonly affected by little league elbow?
Ages 9 to 14
What is the red flag palpation finding in little league elbow?
Tenderness at the medial epicondyle in an adolescent thrower
What imaging finding may be seen in little league elbow?
Widening of the apophyseal line, fragmentation, or enlargement, with oblique views helping visualization
What is the core management principle for little league elbow?
Rest from throwing, ice, gradual progression through ROM and strengthening, shoulder rehab, and correction of throwing mechanics before return
What ligament complex is insufficient in posterolateral rotary instability?
The lateral collateral ligament complex, especially the lateral UCL
What is the classic mechanism of posterolateral rotary instability?
Axial compression plus supination plus valgus force, often with a FOOSH
What symptoms suggest posterolateral rotary instability?
Buckling or clunking with the arm in extension and supination
What special test is used for posterolateral rotary instability?
The PLRI apprehension test, also called the pivot shift test
What is emphasized in rehab for posterolateral rotary instability?
Whole kinetic chain rehab, immobilization or bracing, AROM, swelling control, progressive strengthening, and avoiding valgus loading
Who is a typical candidate for total elbow arthroplasty?
A person with rheumatoid arthritis or an elderly patient with humeral fractures and low ADL demands
Why is total elbow arthroplasty considered a last resort?
It is performed rarely, mainly for pain relief in low-demand patients, and is not recommended for younger high-level patients
What is the typical mechanism of radial head fracture?
Traumatic FOOSH
What associated injuries should be considered with radial head fracture?
Osteochondral injury, wrist or shoulder injury, torn capsule, UCL tear, RCL tear, brachialis tear, distal radioulnar instability, medial elbow instability, and PLRI
What is the red flag symptom in radial head fracture suggesting forearm compartment syndrome?
Severe pain even after immobilization and reduction
What are the key rehab principles after radial head fracture?
Restore ROM, restore strength, maintain function during immobilization, and mobilize as soon as appropriate depending on fracture stability
What defines a Monteggia fracture?
Dislocation of the proximal radius with fracture of the ulna
What mechanism commonly causes a Monteggia fracture?
A direct forearm blow or FOOSH
What is a common mechanism of olecranon fracture?
Fall backward or FOOSH, sometimes with triceps avulsion from forced flexion during muscle contraction
What special test may be positive with olecranon fracture?
The elbow extension test
What is a coronoid fracture?
An injury where the anterior humerus shears off part of the coronoid process during posterior dislocation
What early management is used for a stable non-displaced elbow fracture?
Sling or splint for about 3 days with immediate active elbow flexion exercise
Why should early PROM often be avoided after elbow fracture or ORIF?
Because it may stimulate heterotopic ossification
What is a common ROM complication after elbow dislocation?
Loss of terminal extension, often around 10 to 15 degrees
What vascular complication can occur with humerus dislocation?
Brachial artery injury
What nerve is most commonly injured in elbow dislocation complications?
The ulnar nerve
What is nursemaid’s elbow?
A partial slippage of the annular ligament over the radial head into the radiocapitellar joint
What age group commonly gets nursemaid’s elbow?
Children around 2 to 3 years old
What mechanism causes nursemaid’s elbow?
Longitudinal traction on an extended and pronated elbow
How does a child with nursemaid’s elbow typically hold the arm?
At the side with the palm facing down
What is Panner’s disease?
Aseptic necrosis of the capitellar epiphysis in a growing child
What age group is commonly affected by Panner’s disease?
Ages 5 to 12, mostly males
How does Panner’s disease usually present?
Insidious lateral elbow pain in a self-limiting condition
How is Panner’s disease usually managed?
Short immobilization, avoiding repetitive stress, symptom management, and gradual return once symptoms resolve
What is osteochondritis dissecans of the capitellum?
Localized fragmentation of bone and cartilage of the capitellum with loss of subchondral bone and breakdown of articular cartilage
What age group commonly develops capitellar OCD?
Athletes ages 10 to 16, mainly in the dominant arm
What mechanism is associated with capitellar OCD?
Insidious onset from repetitive valgus loading and microtrauma, such as in baseball pitchers and gymnasts
What symptoms suggest capitellar OCD?
Lateral elbow pain, possible locking or catching in advanced stages, flexion contracture, pain with extension and pronation, and possible MCL laxity
How is capitellar OCD generally managed?
Stop aggravating activity, do ROM exercise, gradually strengthen once symptoms stop, and use surgery for unstable lesions or failure of conservative management
How can capitellar OCD be distinguished from Panner’s disease?
OCD occurs in older children or adolescents and is associated with repetitive sports trauma, while Panner’s disease occurs in younger children and is self-limiting