Behavioral Medicine Lecture 13
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
2) Gender
-
Women are not men
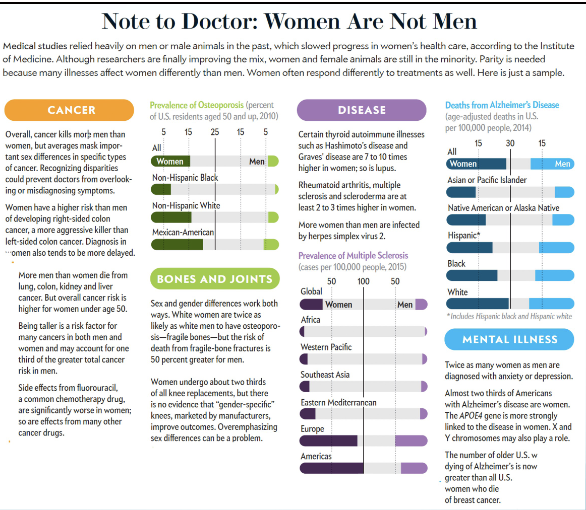
Bikini approach
Research on women tend to have a bikini approach of breasts and pubic area
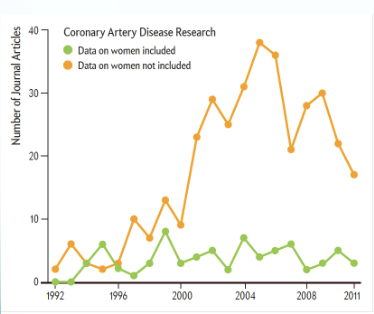
Heart disease and women
Under 10% of research has included data on women
Some not-so-fun facts
In 1977 the FDA banned most women of “childbearing potential” from participating in clinical research studies, concerned that hormone levels would muddy results
1993 that Congress codified a new NIH inclusion policy for women and minorities into law
As of 2020, only 10.8% (NIH) funding is allocated to women’s research
Despite living longer than men, women spend 25% more of their lives in poor health
(cont)
2024: analysis of common medical interventions, 64% were found to disadvantage women due to lower effectiveness, access or both.
WHO estimates that 1/10 women worldwide are living with endometriosis
Getting a proper endometriosis diagnosis can take up to 11 years.
Analyses of US health records and studies indicate that fewer than half of women living with endometriosis have a documented diagnosis
Frued
Freud coined the term hysterical
He believed that women overexaggerated pain or had psychosomatic pain
(cont 2)
2016: Review of 112 internal-medicine residency programs found:
~25% did not include menopause in the core curriculum,
~70% did not include infertility,
~ 30% did not include contraception
~40% did not include PCOS (which affects ~13% of women).9
2021: study showed that in 75% of cases where a disease impacts one gender, the research funding patterns favor men.
Diseases that predominantly affect women, e.g. migraines, headaches, anorexia and endometriosis, received funding that was a fraction of what was awarded for diseases that predominantly affected men, when funding amounts are matched to disease burden
2X the funding goes to diseases that affect men vs. those that mainly impact women
(cont 3)
1999: The American Heart Association published a Guide to Preventive Cardiology for Women finally recognizing that women experience heart disease (including heart attacks) differently.
Only 4.5% of funding for coronary artery disease research is targeted at women.
Cardiovascular disease is the leading cause of death in women; ~45 % of women 20 yrs old + are living with some form of cardiovascular disease
Women’s health gap amounts to 75 million years of life lost due to poor health or early death every single year.
Closing the gap would give the 3.9 billion women in the world an extra seven healthy days a year (or an average of 500 days over the course of a lifetime)
Research in women’s health primarily focuses on diseases with high mortality, overlooking diseases leading to disability
Endometriosis is a chronic inflammatory disorder in which women may experience debilitating chronic pain, infertility, and decreased health-related quality of life. While patients are waiting for a diagnosis, they can experience disease progression, onset of new symptoms, further decline in quality of life, and increasing health care costs
When women get diagnosed, it is much later in the disease process, which leads to treatment being more expensive
More information re Women’s Health
The Society for Women’s Health research found here:
Founded 35 years ago to address disparities in women’s health
Mission: Advance women’s health through science, policy, and education while promoting research on sex differences to optimize women’s health.
Vision: Make women’s health mainstream
Women pain
When women are in pain, it tends to be downplayed
In terms of gender stereotypes, men are viewed as rational, while women are viewed as irrational
*video on slides
Women talking about how their conditions were initially dismissed, and then diagnosed with a severe condition later
Why is women’s pain not taken seriously
sensitive to it BUT their reports are taken less seriously & receive less aggressive treatment
e.g. sedatives vs. pain medications
WHY?
Women have more coping mechanisms to deal with pain but this may suggest that they can tolerate it better and that their pain does not need to be taken as seriously
i.e. women continue to complete tasks in her day-to-day life, vs. men who stop when in pain
Halo effect “What is strong is beautiful”: More attractive patients (vs. unattractive patients) are viewed as experiencing less pain
Women are socialized to attend more to their physical appearance = more often a victim of these assumptions
(cont)
Because of childbirth, women are thought to be able to tolerate higher levels of pain and therefore need less treatment for it
Women more frequently report pain to a health-care provider but are more likely to have it discounted as "emotional” or "not real.”
Freud & conversion hysteria with Anna O.
The male gender role is associated with strength and emotional inhibition vs. the female gender role which encourages the expression of emotion.
The subjective nature of pain requires health care providers to view the patient as credible and objective; “emotional” stereotype is at odds with these qualities
Women & pain
S1: participants
981 (65% women) ER patients presenting with abdominal pain
Triage pain score (1–10), patient demographics, provider gender, and final ED outcome were recorded by RAs
The type/time of medications administered were obtained directly from the medical record
DV:
Time to analgesia: time from patient placement to time of analgesia administration
Type of analgesia administered: opioid or not
Results
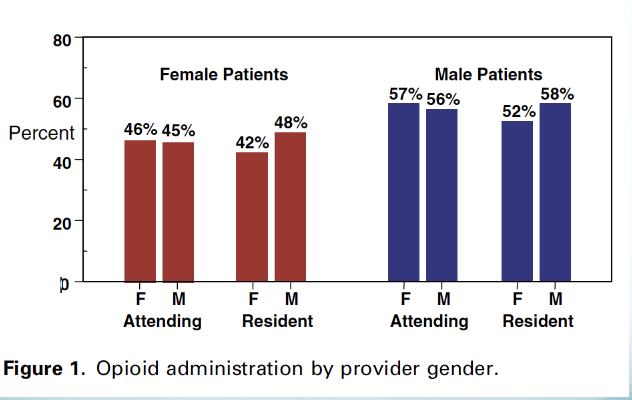
Analgesia was administered to 62% of the study group.
Compared to men, women had a similar mean pain score (6.7 vs. 6.5; p = 0.3), but were significantly less likely to receive any analgesia (60% vs. 67%), and less likely to receive opiates
Women who did receive analgesia waited, on average, 16 minutes longer for their medication than men (median time 65 minutes vs. 49 minutes)
For opiates, 63 minutes vs. 48 minutes, difference 15mins
This gender disparity in receipt of opioid analgesia existed regardless of attending or resident gender, suggesting an implicit bias
Women & pain
Schäfer et al., 2016
Effects of trustworthiness, patient gender, and patient history of depression on pain clinicians’ and medical students’ views of patients with chronic pain
34 pain clinicians and 29 medical students watched videos and used a scale to rate the extent they believed the patient was exaggerating/hiding/minimizing pain, and the likelihood that they would prescribe certain treatment
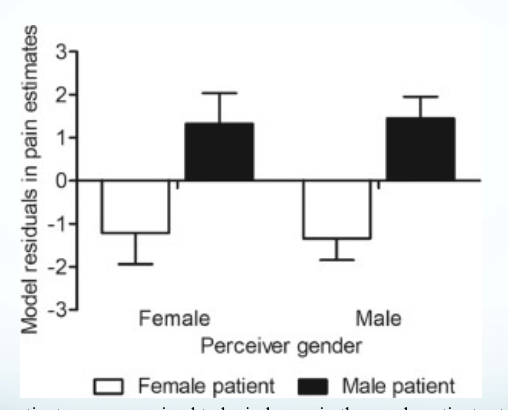
Men were seen as experiencing more pain than women, and more likely to be hiding or minimizing their pain, while women were seen as more likely to be exaggerating pain
True for both pain clinicians and medical students, but much more pronounced for medical students
Women & pain (cont)
Pain doctors and students were more likely to prescribe opioids and non-opioid analgesics to men than women, and these judgements were unrelated to the participants’ pain estimates
Trustworthiness perceptions had no effect on men’s pain estimates,
BUT women who were perceived to be untrustworthy were attributed less pain than those perceived to be trustworthy
Beyond doctor’s perceptions
Zhang et al 2021
Experiment 2:
197 participants reviewed video clips of men and women discussing their chronic shoulder pain
These videos were coded for pain expressiveness and self-reports of pain
DV: pps ask to behave like a doctor prescribing pain treatments, psychotherapy treatments, and a forced choice between the two.
Pps also completed Gender Role Expectation of Pain (GREP) questionnaire
Found
The prescribed amount of medication or therapy didn’t differed by gender of patient
In the forced-choice condition men were prescribed medication over therapy significantly more than women
GREP showed strong gender stereotypes:
Belief that men are less likely to report pain correlated with higher pain estimates/prescriptions,
Beliefs that women were more likely to report pain not correlated with estimates/prescriptions
Graph
Women’s pain is underestimated compared to men’s
Perceived to befit more from psychotherapy

3) Gender & Race: black women & birth
“The statistics show that even if you are a Black woman with a Ph.D., the likelihood is that a white woman with a high school diploma would survive pregnancy and childbirth more than you would,”
Pregnancy-related deaths
“The average rate of 17.4 maternal deaths per 100,000 live births for all American women is disturbing, but Black women are dying more than any other racial or ethnic group. The widest disparity is seen when compared with white women, where Black women are 2/3 x more likely to die of pregnancy-related causes. They are also more likely than white women to experience severe maternal morbidity, also known as “near misses.” [..] “Structural racism is a powerful social determinant of maternal health [..] and persists today in more subtle healthcare policies and practices.”
![<p>“The average rate of 17.4 maternal deaths per 100,000 live births for all American women is disturbing, but Black women are dying more than any other racial or ethnic group. The widest disparity is seen when compared with white women, where Black women are 2/3 x more likely to die of pregnancy-related causes. They are also more likely than white women to experience severe maternal morbidity, also known as “near misses.” [..] “Structural racism is a powerful social determinant of maternal health [..] and persists today in more subtle healthcare policies and practices.”</p>](https://assets.knowt.com/user-attachments/6c61802f-a4ae-4b23-9089-cd05f77cc553.png)
video on slides
Mortality rates during childbirth among black women is 2.6 times higher than white women
Childbirth mortality rate jumped 30% from 2020 to 2021
The US is the 99th ranked country in black mortality during childbirth
Serena Williams
Despite her obvious strength and good health, the world champion tennis player has a history of blood clots. [..] Williams takes blood thinners every day to prevent clots from forming. After the C-section, though, she stopped taking them to allow the surgical wound to heal. The next day, off the “anticoagulant regimen” medication, the 23-time Grand Slam winner began to gasp as she recovered in her hospital room. Not wanting to worry her visiting mother, Williams stepped into the hall and flagged a nearby nurse, insisting that she needed an IV with heparin, a blood thinner, and a CT scan to check for clots. The nurse believed that medications might have befuddled Williams, Vogue says, but a doctor arrived – only to perform an ultrasound, and not the CT scan that Williams believed she needed. The ultrasound revealed nothing, and […]Williams reiterated: “I told you, I need a CT scan and a heparin drip.” Obeying her request for the scan, the medical team found several small blood clots in her lungs and immediately began the medication.”
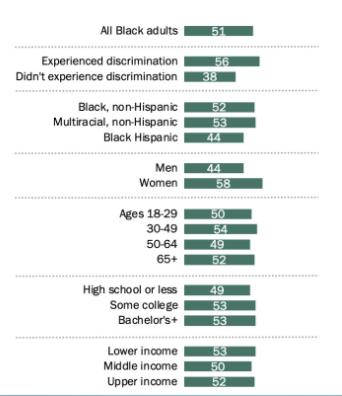
Black women are more likely than black men to say the healthcare system holds black people back
4) Obesity Bias
-
Obesity and evolution
Evolutionary basis to eating & weight-regulation
During pre-historic times inconsistent food supplies were one of the main threats to survival
Fittest individuals = preferred high calorie food (taste preferences), ate to capacity when food was available, efficient body-fat storage metabolism
Evolved strong mechanisms to start eating & weaker ones to stop eating
Current society
Retained prehistoric food preferences but food no longer requires tremendous energy expenditure
Cultural factors contribute to the centrality of high calorie
Fat cells and fat loss
The average human can have between 10 to 30 billion fat cells.
Cells are called “adipocyte” cells and store non-consumed fat as triglycerides.
Insulin (energy storage hormone) regulates the flow of triglycerides into your fat cells
Number of fat cells set during adolescence and levels off into adulthood
If you are an obese child, you will add twice as many fat cells compared to a child of average weight as you mature.
Fat cells shrink when you lose weight because of an energy deficit and your body's release of waste products.
Obesity and stigma
Weight stigma is the devaluation of an individual or group due to weight or body size
Affects up to 57% of all persons regardless of body size
People labeled as obese are more stigmatized than any other social group
Stereotypes of being lazy, weak-willed, unsuccessful, unintelligent, lacking self-discipline, and noncompliant with self-care and weight loss recommendations
Negative stereotypes often dictate healthcare provider’s behaviors (discrimination)
Fat and Stigma
Many significant contributors to obesity are beyond genetic/biological factors and are also beyond individuals’ control
Social disadvantages may increase obesity through chronic stress, anxiety, and negative mood – all are associated with abdominal obesity
Activating physiological mechanisms that can increase appetite and blunt the satiety system, increasing fat retention & food intake
‘‘a more accurate conceptualization of the obesity epidemic is that people are responding to the forces in their environment, rather than lacking in willpower and self-control.” D.A. Cohen
There is increasing consensus that environmental change is essential to the solution of obesity