Looks like no one added any tags here yet for you.
What is the definition of keratoconus
progressive bilateral, asymmetric disease characterized by steepening and distortion, apical thinning and corneal ectasia
What are the key characteristics of KCN
asymmetric
onset: early teens to early 20’s
progression: stops by 4th decade, faster during significant hormonal changes (ie. pregnancy, puberty)
What is the prevalence of KCN
1 in 375 people
1 in 223 children
What is the pathophysiology of KCN
Abnormality in biomechanics of anterior 1/3 of stroma weakens the structural integrity of the cornea —> protrusion forward of posterior surface of cornea
where in the cornea is it typically located
central or paracentral cornea
inferior temporal
What increases (inflammatory wise) in KCN
increase in MMP9, TNF-alpha, IL6
KCN is a disease of the _______ stroma
anterior cornea is affected in early stages
in later stages, descemet;s membrane and posterior limiting lamina may be affected
anterior stroma
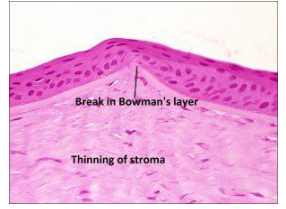
What is the classical triad of the histologic changes in KCN
thinning of the corneal stroma
breaks in bowmans layer
iron deposition in the basal layers of the corneal epithelium
when theres degeneration of epithelial cells what happens next?
fragmentation in bowmans layer
abnormal enzymes in epithelium > excess collagenase and reduced protease inhibitors in stroma > death of keratocytes in the stroma
What is helpful in differential diagnosis of subclinical early/ KCN
epithelial thinning over apex of cornea
Accumulation of ferritin particles within and between basal cells is known as what?
fleischer ring
Breaks in ______ layer are present in > ____% of eyes with KCN
bowmans
70%
What happens in the stroma during KCN
reduced number in lamallae/ density of collagen
loss of inerlamellar weaving
keratocytes turn into fibroblasts and myofibroblasts
induce fibrosis and contribute to formation of scars
What happens in descemet’s membrane during KCN
irregularities, thinning, breaks/ deformities in 20% of severe KCN cases
breakdown of corneal stroma results in descemet’s being more susceptible to hydrostatic pressure of IOP
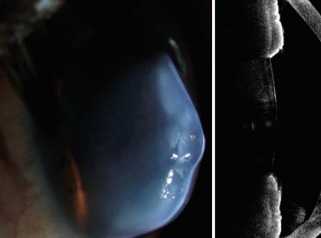
What are hydrops?
breaks that occur from forward -movement of posterior cornea —> allowing influx of aqueous into the stroma and epithelium
What are some common associations of KCN
metabolic changes in the corneal tissue
atopy
connective tissue disorders
eye rubbing
inheritance
___% of keratoconic patients have atopy
50%
excezma
allergies
atopic dermatitis
primary symptom of atopy is
itching
thus many KCN pts are aggressive eye rubbers
SO advise pts to not rub their eyes
________% of pts with keratoconus have a family history
6-16%
What are the associated genetic syndromes of KCN
down syndrome
woodhouse sakati syndrome
marfan syndrome
ehlers-danlos
What is the goal when treating KCN
stop progression of disease
preserve the pts visual acuity
To diagnose KCN the following must be present:
abnormal posterior ectasia
abnormal corneal thickness distribution
clinical non-inflammatory corneal thinning
symptoms of KCN
blurred/ distorted vision
ghost images
H/O several pairs of glasses that have not worked
asthenopia
halos around lights
Signs of KCN
gradual decrease in VA at distance and near
reduced contrast sensitivity
scissor reflex during retinoscopy
increasing myopia and irregular astigmatism (ATR/ oblique axis typically)
difficult refraction
How does KCN look on keratometry
distorted mires
oblique axis of corneal astigmatism
steep curvature
difficulty to diagnose early KCN with keratometry
what helps to locate the apex of cone and monitor progression of condition
topography
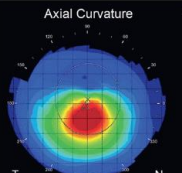
How is an axial map helpful in KCN
provides more global curvature
useful for GP lens fitting
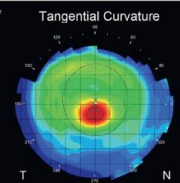
How is tangential map useful in topography
can detect subtle differences in curvature
early diagnosis
monitoring progression
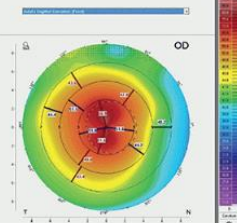
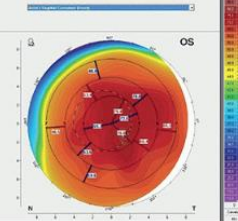
What are the 4 topography patterns that denote KCN
nipple
oval
globus
marginal
Nipple shape
smaller more centralized moutnain
oval shape
inferior, moderate mountain
globus shape
large diameter, encompassing most of cornea
marginal shape
nonround/ nonoval cone in the corneal periphery
How can you detect KCN via topography with:
central corneal power:
I-S value
>47.2D
>1.4D
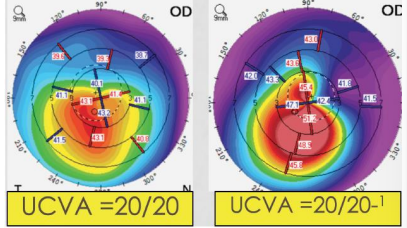
What is the bottom line of KCN
asymmetry
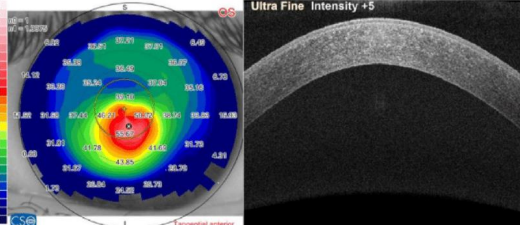
How does TOMOGRAPHY help with EARLY detection of keratoconus
changes in POSTERIOR corneal surface will occur FIRST
ectatic corneas exhibit more rapid thinning from the periphery of the cornea to the apex
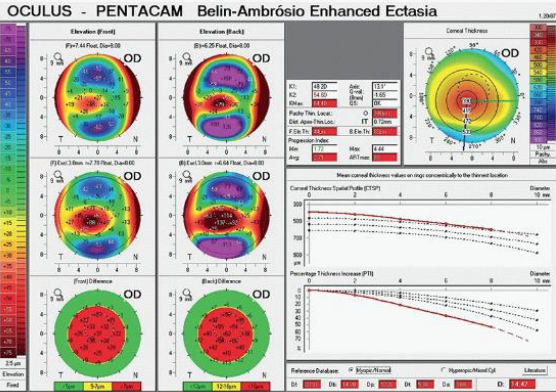
What is one of the best tomography maps for KCN monitoring
belin-ambrosio enhanced ectasia display
Anterior elevation at thinnest point
Posterior elevation at thinnest point
Change in anterior elevation
Change in posterior elevation
Corneal thickness at thinnest point
Location of thinnest point
Pachymetric progression
Ambrosio relational thickness
Kmax
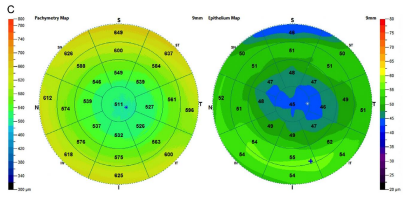
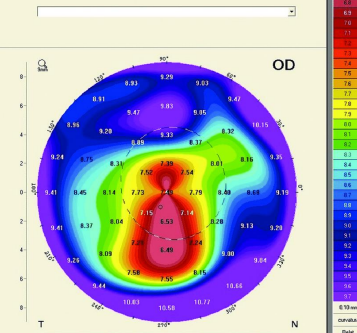
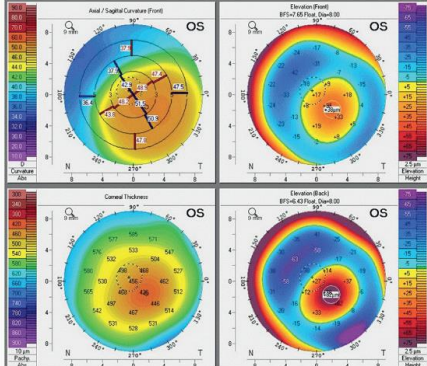
What are signs of KCN on tomography maps
areas of higher elevation on anterior and posterior maps
corneal thinning on pachymetric map
color map shows increased power in isolated area of cone
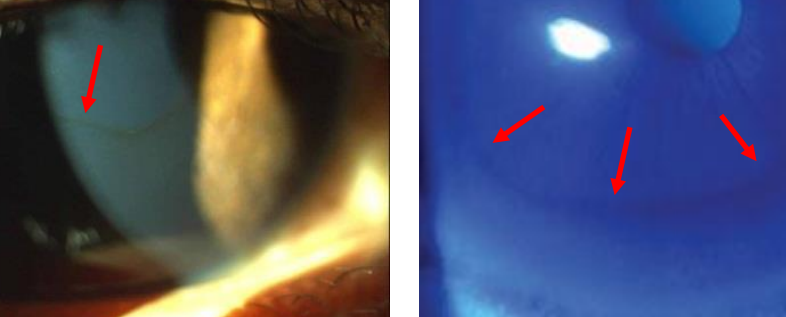
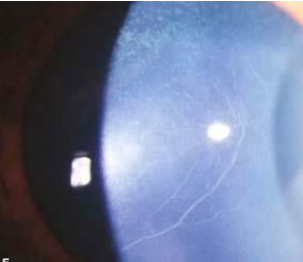
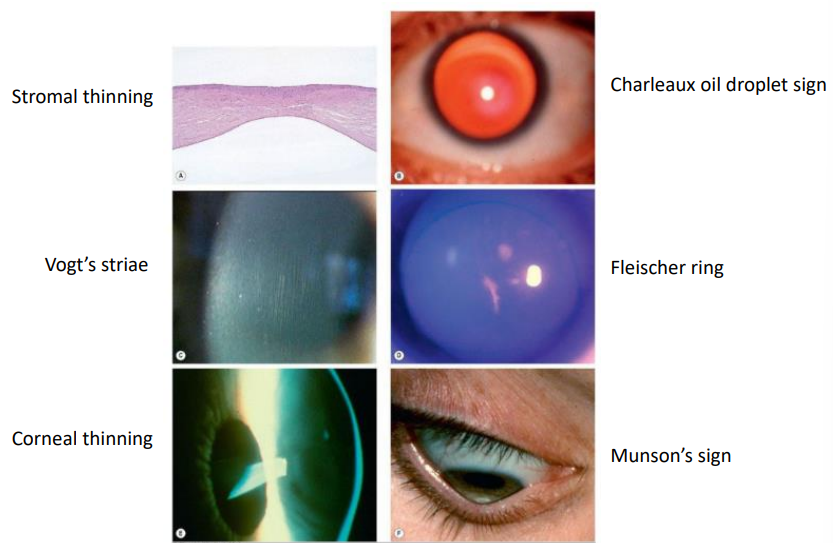
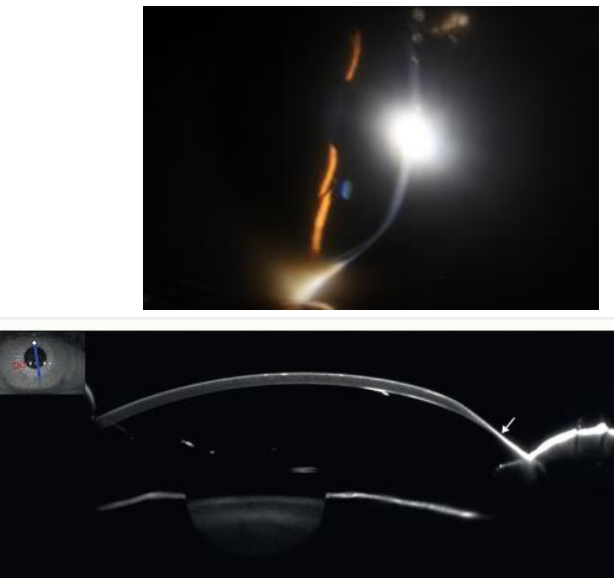
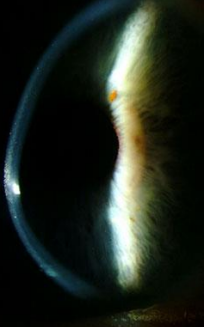
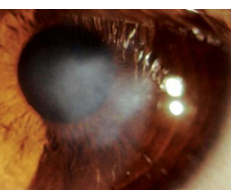
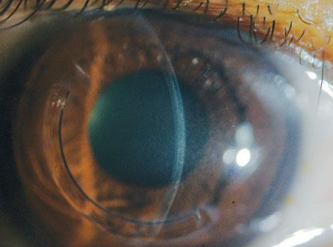
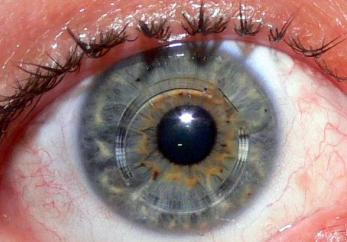
Name three slit lamp signs of KCN
fleischers ring
vogts striae
corneal scarring
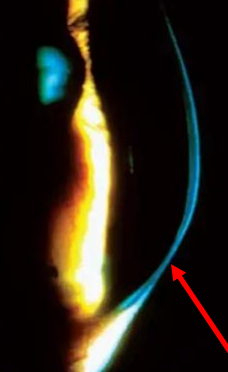
Fleisher ring
vogt striae
corneal scarring
Prominent corneal nerves
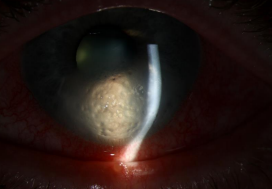
What causes corneal hydrops
rupture in descemets memrbane
aqueous humor flows through damaged endothelium > leading to corneal edema + eventual scarring
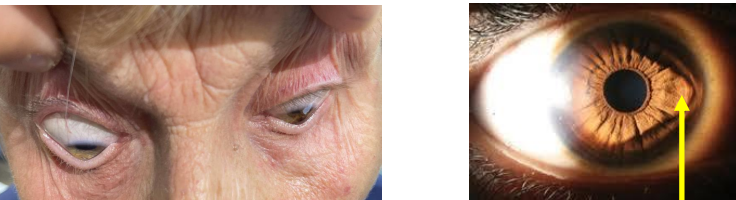
Name two external signs of KCN
munsons sign - altered shape of eyelid on downgaze due to protrusion of the cone
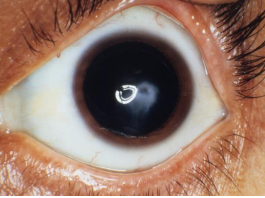
Rizzuti’s sign - point of light formed on iris by illuminating cornea with penlight from the side
More diagrams of hallmark signs
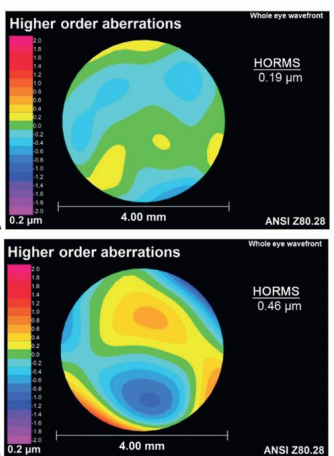
What are aberrations
optical imperfections that prevent light from achieving a tight focus on the retina, even with conventional optical correction
lower order: spherical and cylindrical refractive error
higher order: coma, trefoil
How can aberrations be measured
wavefront aberrometers
those with corneal ectasias experience MORE higher order aberrations
Most common aberration seen in KCN
coma
trefoil
spherical aberration
s/x: light distortion, comet-like tails on objects/lights, difficulty with night vision, starburst patterns, double vision
What are two common corneal warpages seen CL wear
(imitators of KCN)
inferior steepening on topography
scissor reflex on retinoscopy
ie. thick soft lenses worn for extended periods, high riding GP lenses
How is this different than KCN
CL warpage reverses completely within a few weeks of d/c CL wear
steepening below 50D
KCN have clinical signs and is progressive
no abnormal posterior elevation
how to manage CL warpage
discontinue wear
refit to higher DK lens material with better fitting relationship
what is pellucid marginal degeneration
progressive, bilateral corneal disorder with a peripheral band of thinning of the inferior cornea
What are common characteristics of pellucid
4-8’oclock location
1-2mm unaffected area between area of thinning and the limbus
may be a disease on the same spectrum as KCN
later age of onset
better vision for longer
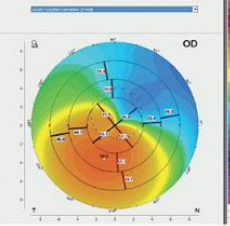
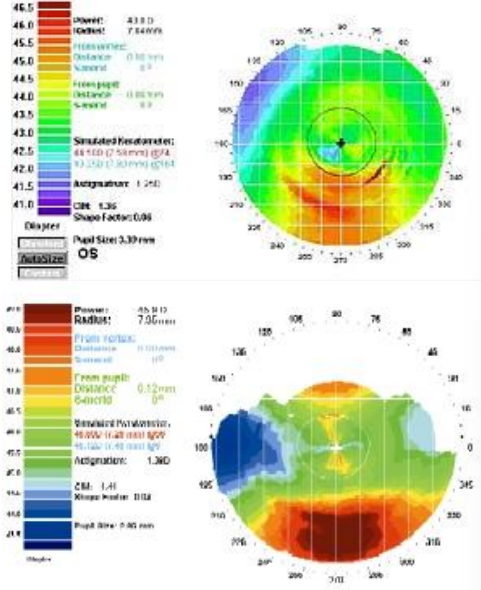
What is the infamous topography signs of pellucid
large amount of ATR astigmatism
“kissing dove” “crab claw” appearance
areas of greatest thinning and steepest corneal curvature are close to _______
the limbus
more images of pellucid
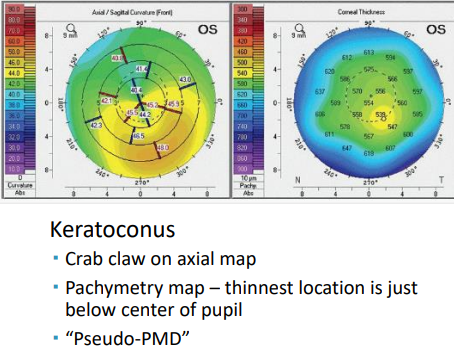
KCN on topography maps
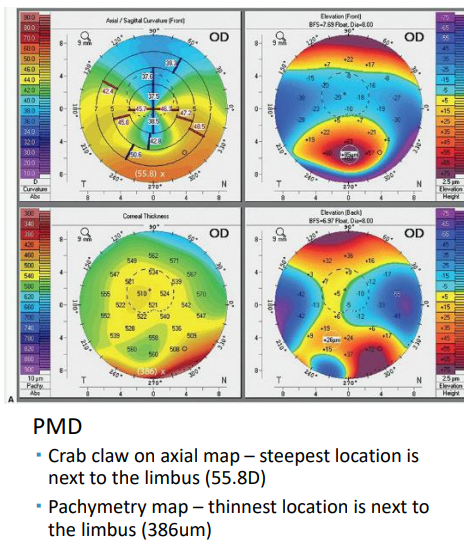
PMD on topography maps
what is keratoglobus
entire cornea THINS, mostly near the limbus
bilateral
present from birth
non-progressive
_____% of refractive surgery candidates have subclinical KCN
5-7%
post-op ectasia occurs in ___% to ____% of refractive surgery cases
0.04% to 0.06%
vast majority are LASIK cases
why surgeons like to evaluate corneal thickness and biomechanics pre-operatively to avoid this
What does the Amseler-Krumeich system look at to classify ectasias
based on K’s, CCT, refraction and degree of scarring
How did CLEK study grading of KCN characterize:
Mild
Moderate
Severe
mild: <45D
Moderate: 45-52D
Severe: >52D
What does the Belin ABCD system look at for KCN classification
anterior-surface curvature
posterior-surface curvature
corneal pachymetry at thinnest location
corneal scarring
Subclinical KCN
An eye with positive or suspicious topographic findings
NO slit lamp findings, but with KCN in the fellow eye
Forme fruste KCN
an eye with no topographic findings
NO slit lamp findings and KCN in the fellow eye
What is defined as progression:
At LEAST TWO of the following
steepening of ANTERIOR corneal surface
steepening of POSTERIOR corneal surface
THINNING or INCREASE in rate of corneal thickness change from periphery > thinnest point
T or F: it is possible to predict rate of progression for each patient
FALSE - impossible
typically progresses over 3-8 years
What does CLEK study signify as progression
0.20D increase in flat K per year
¼ patients steepened by 3D in 7 years
12% needed keratoplasty over 8 years
do NOT fit patients with KCN in flat GPs
___ % of KCN pts indicated the diagnosis had some impact on their lives
__% indicated a moderate or severe impact on life
90%
40%
why pt education is so important (ie. prognosis, loss of vision or need of transplant)
Overall. pts with KCN have more _______ coping mechanisms
dysfunctional
may impact their relationship with healthcare providers
influences clinical perception that they are less respectful, less conforming, and less cooperative than other patients
Why is spectacle correction a less common form of treatment for KCN pts
refractive error can change rapidly
do not correct irregular astigmatism and HOA
anisometropia may occur due to asymmetry of disease
only best used if specs are in early disease, before CL use (back up)
List 5 CL that may be useful in correction of KCN pts
corneal GP lenses
scleral lenses
soft lenses
piggyback lenses
hybrid lenses
In majority of KCN cases, lenses are considered _______ _________
medically necessary
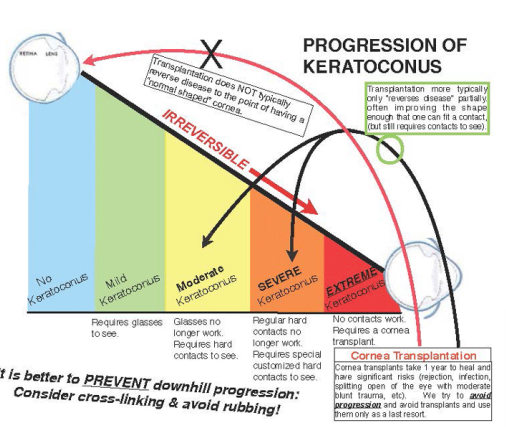
what is used as a last resort option for those with KCN and poor visual acuity and difficulty with fitting CL
surgery
10-22% of pts with KCN require a corneal transplant
IF impossible to achieve stable CL fit, IF excessive scarring + thinning
What was FDA approved in the US in 2016
(hint: age 14-65 years with progressive KCN or corneal ectasia after refractive surgery)
corneal cross-linking
How does corneal crosslinking work?
addition of molecular bonds to INCREASE the mechanical strength of the corneal stroma
increase rigidity of collagen lamellae
increase collagen fiber diameter
stabilize the shape of cornea
What is the exact mechanism that corneal cross-linking uses
riboflavin (vit B2) + UVA radiation
photosensitizer - absorbs UV radiation causing a cleavage of oxygen, which splits off and causes cross-linking in the tissue
more crosslinks = STRONGER tissue
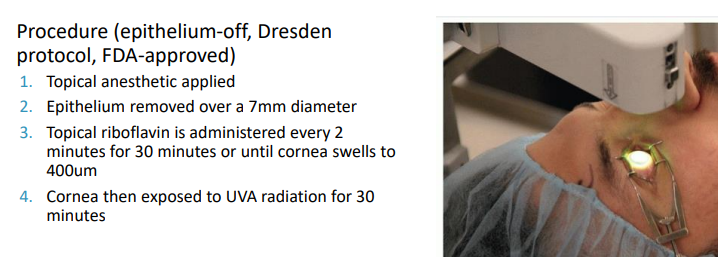
Mechanism of surgical procedure
What is the post-op care for corneal cross-linking
Bandage CL worn for 3-5 days until epithelium is healed
Topical antibiotic x 1 week
Topical corticosteroid x 2-3 weeks
Remain out of CLs for ~1 month after procedure
What may happen after the corneal cross-linking procedure
cornea may change shape after procedure
CL may need to be refit
epithelium may not fully heal for up to 1 year
What is the purpose for corneal crosslinking
stabilize progression of KCN
reduced myopic refractive error and flattens K readings by 2-3 D
may improve subjective vision function (glare, halos, starbursts)
resulted in 25% reduction rate of corneal transplants
Epi-off procedure requires a min. corneal thickness of _____ um
400 um
can be artificially thickened by using HYPOTONIC topical drops during procedure
what are the complications of corneal cross linking
corneal haze - 90% of pts
eye pain
abrasion
MK
sterile infiltrates
corneal edema
corneal opacity
scarring
Which treatment of cross-linking are currently “off-label”
epi -on (no epithelial debridement, less discomfort, takes longer to get riboflavin to stroma)
accelerated CXL - increased intensity of irradiation to reduce treatment time
combined CXL with other procedures
CXL + refractive surgery ‘
CXL + intrastromal corneal ring segments
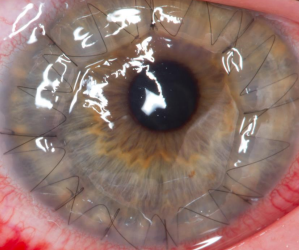
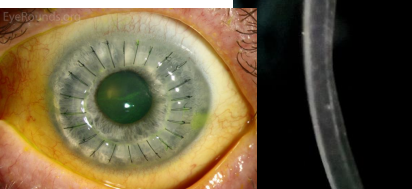
What is Penetrating keratoplasty (PKP)
full-thickness corneal transplant (all layers)
endothelial loss begins immediately (drops to 800/ mm2)
impacts tolerance to reduced O2 states
what is anterior lamellar keratoplasty (DALK)
leaves the endothelium
less risk of rejection
KCN may recur with with corneal transplant procedures
PKP
DALK
life expectancy of a graft is ______ years
15-25 years
What is a problem with intrastromal corneal ring segments (IRCS)
very LOW Dk - may observe neovascularization
implant may migrate - extrusion possible, inflammation + staining possible
difficult to fit CL over
SUMMARY 1
SUMMARY 2