EMT Bleeding, Musculoskeletal, Head and Spine
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
Arteries
Carries blood away from the heart. Normally oxygenated (except pulmonary and umbilical arteries)and are responsible for supplying oxygen and nutrients to tissues throughout the body
Aorta
Largest artery, originates at left ventricle and extends to abdomen. Distributes oxygenated blood to all parts of the body
Pulmonary
Carries deoxygenated blood from the heart to the lungs
Brachial
Inside upper arm artery that supplies blood to the arm and hand.
Radial
In the wrists
Carotid
Located in the neck
Femoral
Medial portion of femur
Veins
Carries blood towards the heart. Most carry deoxygenated blood back to the heart (except pulmonary vein and umbilical veins, carrying oxygenated blood to the heart)
Capillaries
Only one cell thick enables the exchange of water, oxygen, carbon dioxide, and many other nutrients and waste chemical substances between blood and surrounding tissues
Detailed Order of Blood Flow:
Superior/Inferior Vena Cava: Deoxygenated blood returns to the heart.
Right Atrium: Chamber receiving oxygen-poor blood.
Tricuspid Valve: Valve between right atrium and right ventricle.
Right Ventricle: Chamber pumping blood to the lungs.
Pulmonary Valve: Valve leading to the pulmonary artery.
Pulmonary Artery: Carries blood to the lungs for oxygenation.
Lungs: Blood picks up oxygen and releases carbon dioxide.
Pulmonary Veins: Carry oxygen-rich blood back to the heart.
Left Atrium: Chamber receiving oxygen-rich blood.
Mitral (Bicuspid) Valve: Valve between left atrium and left ventricle.
Left Ventricle: Chamber pumping oxygen-rich blood to the body.
Aortic Valve: Valve leading to the aorta.
Aorta: Largest artery, distributing oxygenated blood to the body.
Perfusion
Circulation Within Tissues In Adequate Amount To Meet Cells Need For Oxygen
Shock (hypoperfusion)
Failure To Provide Adequate Circulation (Blood Is Not Circulating)
Cardiogenic
- Heart Loses Ability To Pump Blood/Not Circulating Blood & O2
Septic
Infection (Usually Bacterial) Of Blood -> Usually The Appendix (Appendicitis)
Anaphylaxis
Severe allergic reaction
Hypovolemic
Decreased Water Volume -> Blood Gets Thicker And Slower
Hemorrhage
Bleeding
Hemorrhagic Shock
Low Blood Volume Results In Inadequate Perfusion
Average Amount of Blood in an Adult
6 Liters
Maximum blood loss tolerated for an adult
no greater than 20%
Signs and Symptoms of Being Hemorrhagic
Rapid, Weak (Thready) Pulse
Clammy (Moist, Sticky, Cold) Skin
Rapid And Shallow Respirations
Hypothermia (Due To Decreased Perfusion And Evaporation Of Sweat)
Shivering stops and temperature decreases quickly (Enzymes can function under 94 degrees F)
Thirst and Dry Mouth
EMS Treatment for Hemorrhaging
Control bleeding
Elevate feet (if no suspected neck injury)( getting blood out of/away from the injury)
Cover with blanket (if body is too cold, patient becomes unconscious)
Oxygen (15 Liters Per Minute via Non Rebreather)
Characteristics of Bleeding
(Order from most to least dangerous)
Arterial: bright red spurting blood
Venous: dark red non-spurting blood
Capillary: easily controlled oozing blood
Control Bleeding
Direct pressure with bandage
Elevate injury
Bleeding continues, add more dressings (don't remove the dressings, pile them on instead)
Use pressure points (joints) to control
Tourniquet (Last Resort to Control Life Dangering Bleeding)
Wrap bandage around injury, twist and tie
Write TK and time applied on patients forehead
(May lose a limb if bleeding doesnt stop/tourniquet on for too long)
MAST Pants (Military Anti-Shock Trousers) or PASG (Pneumatic Anti-Shock Garments)
Stabilizes and controls blood loss in fractures of pelvis and femur
puts pressure on the wound which limits blood flow + limits amount of pain
(made due to the Vietnam War)
Nose Bleed Directions
Have pt lean forward and pinch nostrils
Apply gauze under pts upper lip
Apply ice over nose
Hematoma (bruise/contusion)
Capillaries are damaged allowing blood to seep into tissue
Hematemesis
blood in vomit (pools up in the stomach)
Hemoptysis
Coughing Up Blood
Internal Bleeding Signs
pain, tenderness, bruising, swelling, broken ribs, bruises on chest distended abs
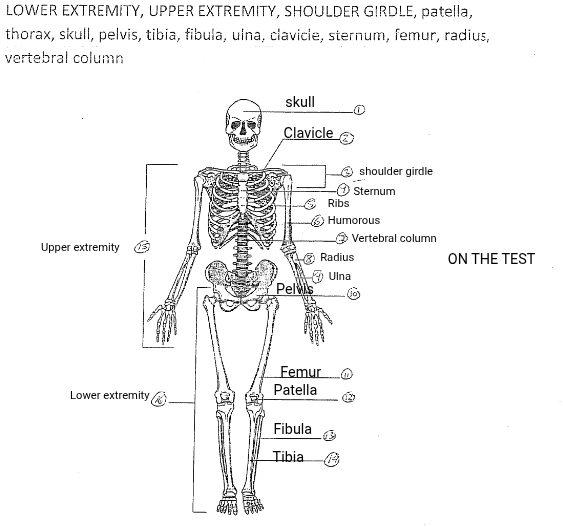
Skeletal System
Protects internal organs, contains 206 bones
Pelvis
Connects the base of the spine to the rear limbs
Lower Extremity (Legs)
Includes foot, thigh, and hip regions
Upper Extremity (Arms)
The deltoid region to the hand
Mechanism of Injury (MOI)/ How the Injury Happened
Used to determine how likely it is that a serious injury has occured
Direct blow? Indirect blow? Twisting force? High-energy injury?
(A low-speed fender-bender in a parking lot is much less likely to cause a life-threatening injury than a rollover accident on the freeway.)
Significant Mechanisms of Injury
Ejection from vehicle
Death in same passenger compartment
Falls over 20 feet
Roll-over of vehicle
High-speed vehicle collision
Vehicle-pedestrian collision
Motorcycle crash
Unresponsive or altered mental status
Penetrations of the head, chest, or abdomen
Fracture
Broken Bone
Closed Fracture
Does not break skin
Open Fracture
External Would from Fracture
Signs of Fractures
Deformity, tenderness, guarding(holding/protecting it), swelling, bruising, etc

Dislocation
Disruption of a joint
Sprain
Joint Injury; tearing of a ligament
Strain
Stretching or tearing of a muscle
Emergency Care
To evaluate injured limb check for CMS
Circulation (pulse and capillary refill), Motor function, and Sensation
Cover wound; apply splint; apply ice if swollen
Rules of Splinting
Remove clothing from the affected area
Note CMS (neurovascular) status
Immobilize the joints/bones above and below injured area

Traction Splint
Legs only
Hazards of Improper Splinting
Damage nerves, tissues and blood vessels
Reduced distal (blood flow in vessels farthest from the heart)circulation
Aggravate the injury
REMEMBER: ULNA IN, TIBIA TUCKED (CLOSER TO THE INNER SIDE OF THE BODY)
Spinal Column
Vertebrae protects spine
Cervical and lumbar are most susceptible to injury
Cervical (anything related to the head)
Thoracic (ribs)
Lumbar (lifting)
Sacrum
Coccyx
(Descending Order)
Extra facts
Cartilage can shift/swell and cause a cartilage disc
Movement of head or neck could make the head/spine injury worse
Effects of nerve damage depends on nature and location of the injury
Assessment of Spinal Injuries
MOI: MVA (Motor Vehicle Accident); fall; trauma; hanging; etc.
If patient is conscious ask the following:
Does your neck or back hurt?
What happened?
WHere does it hurt?
Can you move your hands and/or feet?
Can you feel me touching your fingers and/or toes?
Medical Care I
Restore airway using spinal precautions
Manually immobilize cervical spine
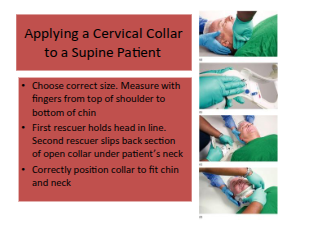
Medical Care II
Apply cervical collar
Medical Care III
Immobilize patient on long board with head blocks
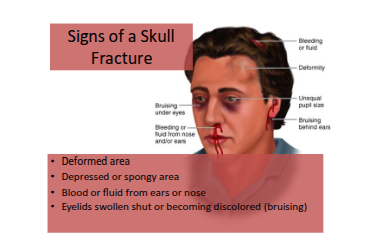
Signs and Symptoms of Head Injuries
Visible skull fractures
Bruising around eyes and behind ears
Failure of pupils to respond to light
Unequal pupils
Unconsciousness
Loss of sensation or numbness
Nausea and Vomiting
Combative or abnormal behavior
Heachache
Clear fluid from nose or ears (CSF: cerebral spinal fluid)
Stiff neck
Inability to move any body part
Tingling

Medical Care IIII
Manually stabilize the head and neck
Establish airway (jaw-thrust if needed)
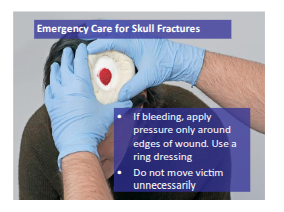
Control bleeding (no direct pressure on skull fracture)
Apply C-collar and immobilize patient
Oxygen (15 LMP via NRB)
Monitor vital signs
Skull Fracture Care
Emergency Care for Spinal Injuries
Supports head position as found if cannot move
Cervical Collar
Helmets
Leave the helmet in place if it does not compromise airway or prevent improper immobilization
Removing a Helmet
Remove a helmet only to care for life-threatening condition
Remove helmet, following local protocol, when face guard prevents giving ventilations
With many helmets, faceguard can be removed/pivoted so helmet is left on for ventilations
For athletic helmets, first unsnap and remove jaw pads
Removing Helmets with Non-pivoting Faceguard
Requires two rescuers
First rescuer slides one hand under neck to support base of skull and holds lower jaw with other
Second rescuer tilts helmet back slightly as first rescuer prevents head movement
Second rescuer pulls helmet back until chin is clear of mouth guard
Second rescuer tilts helmet forward slightly moving helmet back past base of skull, then slides it straight off
Backboarding
Backboarding PT2
Positioning Patients on a Long Backboard
Three or more rescuers needed
Position long backboard beside patient
One rescuer maintains head in line while other rescuers take position (head line rescuer is in charge of the operation)
On cue from rescuer at patients head, other rescuers roll the patient towards them as a unit
Slide backboard next to patient
On cue, other rescuers roll patient as a unit
Patient is secured to backboard using straps
Concussion
Traumatic Brain Injury (Temporarily interferes with the way your brain works, and it can affect memory, judgement, reflexes, etc.)(brain bounces back and forth in the skull)
Signs and Symptoms
Drowsiness
Confusion
Headache
Loss of consciousness
Memory loss (amnesia)
Nausea and Vomiting
Seeing flashing lights
Alarming Signs and Symptoms
Changes in alertness and consciousness
Convulsions (seizures)
Muscle weakness on one or both sides
Repeated vomiting
Unequal pupils
Unusual eye movements
Walking problems