sagittal plane
cuts body left and right
Coronal plane
cuts body front/back
concentric contraction
shortens
eccentric contraction
lengthens
Bone Cell types
Osteogenic: develops into osteoblast
Osteoblast: forms
Osteoclast: Destroys
Osteocyte: maintains
Skeleton
Axial: skull, vertebral, rib. 80 bones
Appendicular: Limbs. 126 bones
Bone types: Long/short/flat/irregular
Cartilage
Hyaline: smooth surface for gliding joints
Elastic: v flexible (ext ear and epiglottis)
Fibro: resists strong compression/tension forces
Functions: support, extra layer of protection btwn bones
joint types (contact btwn 2+ bones)
Fibrous (skull suture): no large movements, practically none
Cartilaginous (pubic symphysis, vert, cart ribs): mostly stability, allows for some movement
Synovial: island caryilage in middle, joint capsule filled w/ synovial fluid. Double layered, inner syn fluid, outer protects. ligs thicken capsule and stabilize joint. Bursae- fluid filled sacks tendon/tendon or tendon/bone to reduce friction. tendon sheaths= elongated bursa
Axes: (perpendicular w/planes)
frontal axis: sagittal plane: flexion extension
sagittal axis: frontal plane: add/abduction
longitudinal axis: transverse plane: rotation
Tissue Types
Epithilium: covering. Secretes substances, regenerates easily. Three types:
surface -sheetlike, protective mechanical barrier (skin), excretes substances
glandular: produces/delivers substances to surfaces or blood stream
Sensory: specialized cells for 4 senses
Connective: supporting
Contains- individual cells dispersed through intracellular matrix. Ground substance (h20, glycoproteins, cosamino/proteoglycans), collagen, reticular, and elastic
Ratios of fibres:ground substance dictate connective type (loose-most GS, Dense-most CF, Fluid-watery due to plasma/water, supporting -calcium deposits)
Muscle
network of muscle cells, contain myofibrils(protein structures which contract), first stim nerves, then transmittes to connective tiss to create movement.
Nervous
complex network of neurons and support cells. Can be stimulated/conduct simuli, respond to stimulation. electrical impulses neuron-neuron or neuron-other cells to communicate to other tissues, regulating int/ext env
Body structures Inv in movement
Bone/Osseous Tissue
supporting connective tissue, movement framework, protects vulnerable organs, stores minerals, produces red blood cells. collagen fibres/minerals.
Ligaments
fibrous, made up of dense connective tissue (dif directions tp resist multidirectional stress). bone-bone. Prevent unwanted joint movement. If wrapped around entire joint -capsule Static stabilizers. Ex. interroseous membrane/joint
Muscle
pulls on periosteum of bones creating movement. 3 types..
Smooth: walls hollow organs
Cardiac: heart walls, pulses
Skeletal: voluntary, connects bones for movement at joints
Tendon
muscle to bone connection, collagen= strength and elasticity. shapes vary
Fascia
Thin membrane loose connective tissue, body structure to unit, surrounds and seperates bones, muscles, joints, skin, muscle layers, compartments. Thickens joint capsules. Interconnects everything. Layers…
superficial: directly under skin. stores fat + water, creates nerve passageways, loose
Deep: around muscles + internal structures, helps movement (muscle attachment), cushions layers. Dense
Subserous: seperates deep fascia of thoracic and abd cavities. Loose connection for movement. Dense.
Special Structures
Skin
protects invasion/radiation, excretion, sensory. 3 layers…
Epidermis: epithelial. thin layers, produce keration and pigment. defensive cells
Dermis: beneath epidermis, dense, contains hair follicles/glands/nerves/blood/ small musc
Hypodermis: beneath dermis. loose, contains adipose to cushion + protect.
Blood vessels:
circulatory sys. Large -arteries, medium -arterioles/venues, smallest -capillaries (indv cells). through lymphatic movement.
Lymphatic vessels/nodes
collect excess lymph fluid from body. Edema= abnormal acc of fluid in tissue.
Nerves:
sensory
Motor
Types of syn joints
Planar: gliding flat surfaces. no axis
Hinge: Convex/concave. A1
Pivot: round surface/bony ring. A1
Condyloid. rounded concave/vex A2
Saddle: Convex/concave (2 pringles). A2
Ball and socket. A3
Joints by function
Synarthrotic: lim mobility, art surfaces nearby
Amphiarthrotic. medium mobility. surfaces slightly further apart
Diarthrotic: most mobility. surfaces furthest apart
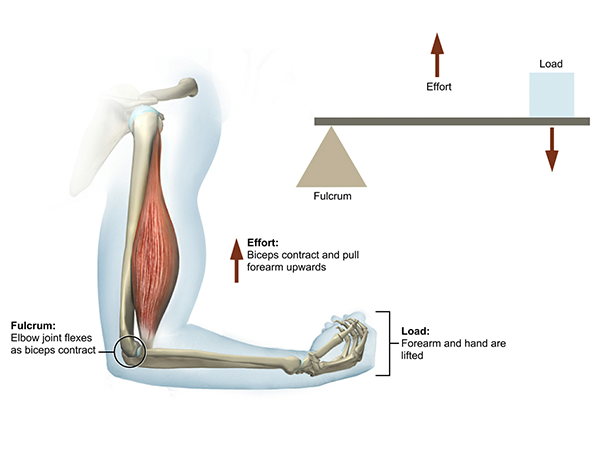
Levers: Points of system
Fulcrum -joint
Force of resistance: weight of bone
Applied force: force on muscles to move
Levers: Mechanical advantage
Kinetic advantage
Fast motion, opposite of MA
1/MA (length of FR over length of AF)
Most levers
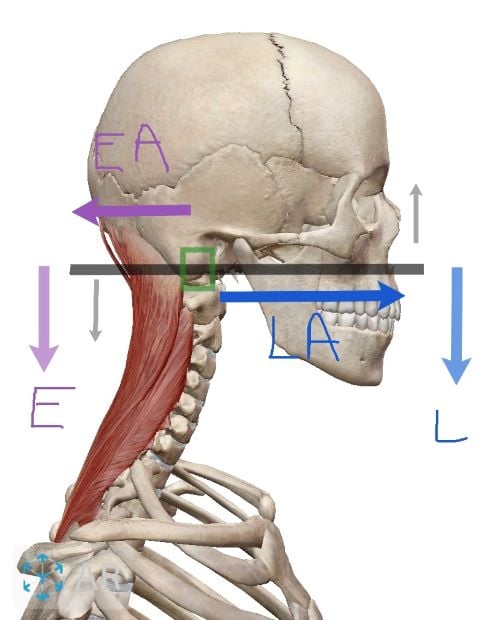
1st class lever
fulcrum inbtwn AF and FR. MA or KA. ex: head and neck extension
2nd class lever
FR btwn fulcrum and FA, AF longer arm then FR, therefore always MA
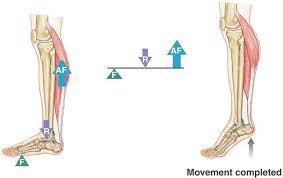
3rd class lever
FA and FR same side. AF shorter then R. KA
Functional Groupings
agonist: prime movers
Synergiste: accesory
Fixator: helps agonist by stabilizing attachments
Antagonist: opposes prime mover, works at end ranges to prevent injury
Endfeel
Bone to Bone
Soft tissue approximation
Tissue stretch
Cranial bones
Frontal
Parietal 2
Occipital
Sphenoid
Ethmoid
Temporal 2
Facial Bones
My mandible chews nine very large zucchini pizza’s
Maxilla
Mandible
Concha (nasal)
Vomer plate
Lacrimal
Zygomatic
Palantines 2
Joints of skull
Sutures
Coronal: front/parietal
Sagittal: L and R parietal
Squamish: Parietal/temporal
Lambdoid: occipital/parietal
Occipitomastoid: occipital/temporal
1 JOINT
Temporomandibular: hinge/planar/condyloid hybrid
allows depression/elevation (open close), protraction/retraction, lat displacement
Skull foramen
Optic canal: optic nerves exit orbits, enter skull
Sup/inf orbital fissure and foramen
Carotid canal: major blood supply
Foramen spinosum: major artery into skull
internal acoustic meatus: cranial nerve exits temp bone to brain (balance and hearing info)
Hyboglossal canal: nerves of tongue muscles
jugular foramen
Paranasal sinuses
warm air entering nose for lungs. improves voice sound (vibration). Flexibility and protection to facial bones, reduces weight/hollow
Orbits
Protect eyes. Made of sphenoid, frontal, zygomatic, ethmoid, lacrimal, maxilla, palantine
Hyoid bone
axial skeleton. Moves when swallow to let food go down, no art w/ any other bone
strongest ligament in the body
iliofemoral
Spine and rib cage functions
protects spinal cord, provides stability, attachements for ribs, supports head, allows for full vision. Wants to make eyes level, scoliosis to compensate
Regions + Curvatures
Vertebrae: 7 C, 12T, 5L
2 Lordosis (cervical and lumbar): vertebrae moving in
2 Kyphosis (thoracic and sacral): vertebrae moving out
better absorbs compression
When neck is bent, spine is straight therefore cannot absorb compression. Head trauma= fracture
Gravity: mastoid process, 2nd sacral vert, hip knee ankle
Cervical Region
2 SP -bifid
short TPs
Triangular vert foramen
2 transverse foramen: Vert artery produces blood flow to head as reserve supply
C1 atlas: no vert body, ring, small TP, lat masses for head
C2 axis: SP 2 bumps, bony landmarks shaped by muscles.
Thoracic region
Ribcage: limits movement, protects heart and lungs. Ribs attach btwn segments, progressively wider, c shaped
True ribs: sternum via cartilage
false ribs: attach cartilage, combine ,then sternum
floating ribs: only to vert column
intercostal #’s allow for space btwn
Sternum: protects front via cartilage for expansion
manubrium, body, xiphoid process
Vertebrae: circular V foramen, costal facets inf/sup, longest downward SPs
Lumbar region
Thick vertebrae to support upper body compression, issues most common
Large often concave body/SPs
triangular V foramen
Sacral/Coccygeal:
Sacrum fused due to force. Ossified, vert bodies/SPs are still there, pelvic movement
coccyx: no purpose
Sitting: not evolved for that, many issues. towel under spine= healthy lordosis
Joints of spine
Facet/apophyseal/zygapophyseal: synovial joint (close to planar but not!). allows spine movement, bilat. phys block L rot, T lat bend
Vert disk (interbody): Gelatinous centre disperses forces. Not innervated=no pain=wear disk w/o knowing. Bulging/herniated disk can compress spinal nerve (numbness burning pain, L/C). Vert endplates -nourish disk, triggered by movement.
Ligaments: reduce movement.
Front of body, ant longitudinal lig: Limits extension.
Behind ““: posterior longitudinal/ligamentum flavum: limits flexion.
Intertransverse: lat flex, rot
Movements of spine
Flex ext/lat flex LR/axial rot
Protraction/retraction: improves vision, lots of strain on neck
Thoracic joints
Costocorpeal: head of ribs/vertebrae
Thoracolumbar flexion: flexion of spine
Thoracolumbar extension: extension should be distributed evenly
Specific Joints
Atlanto Occipital: condyloid
foramen magnum makes instability fatal, many ligs support
Atlanto Axial: pivot
transverse lig stabilizes
resp for 1/2 cervical rot. Vert artery is stretched.
Uncovertebral: bony edges can rub
L5/S1: most herniated. much force of vert column/ where vert angle switches sacrum.
Spondylothesis: vert body adopts angle of sacrum
Imp land marks
Occipital bone:
Sup/inf nuchal line: muscles attch
ext occipital protuberance: bony bomp mid head
occipital to C7: ligamentum nuchae, muscles attch
temporal: mastoid process (behind ear)
ipsi/conralateral
-same side
-opposite side
Sternocleidomastoid
ant neck
O: med clavicle, sternum sup/lat
I: Mastoid process, temp bone
A: if muscles contract, head and neck ipsi lat. ant muscle fibres conralat
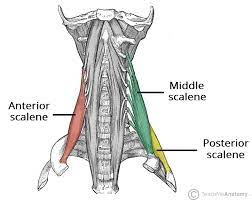
Scalenes (ant/middle/post)
ant neck
O: TP C2/C7
I: sup border 1st rib
A: ant/mid: elevate 1st rib, ipsi lat neck bend
post: elevate 2nd rib, ““
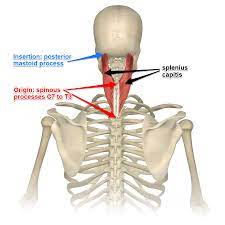
Splenius Capitis
Post neck
O: lig nuchae, SP C3-T3
I: mastoid process, lat sup nuchal line occipital.
A: Bilat ext head and neck, unilat flex, ipsi lat rot
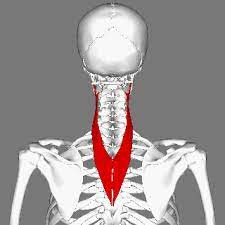
Splenius Cervicis
Post neck
O: T3-T6
I: TP C1-C3
A: ext of C spine. Ipsilat bend/flex and rot
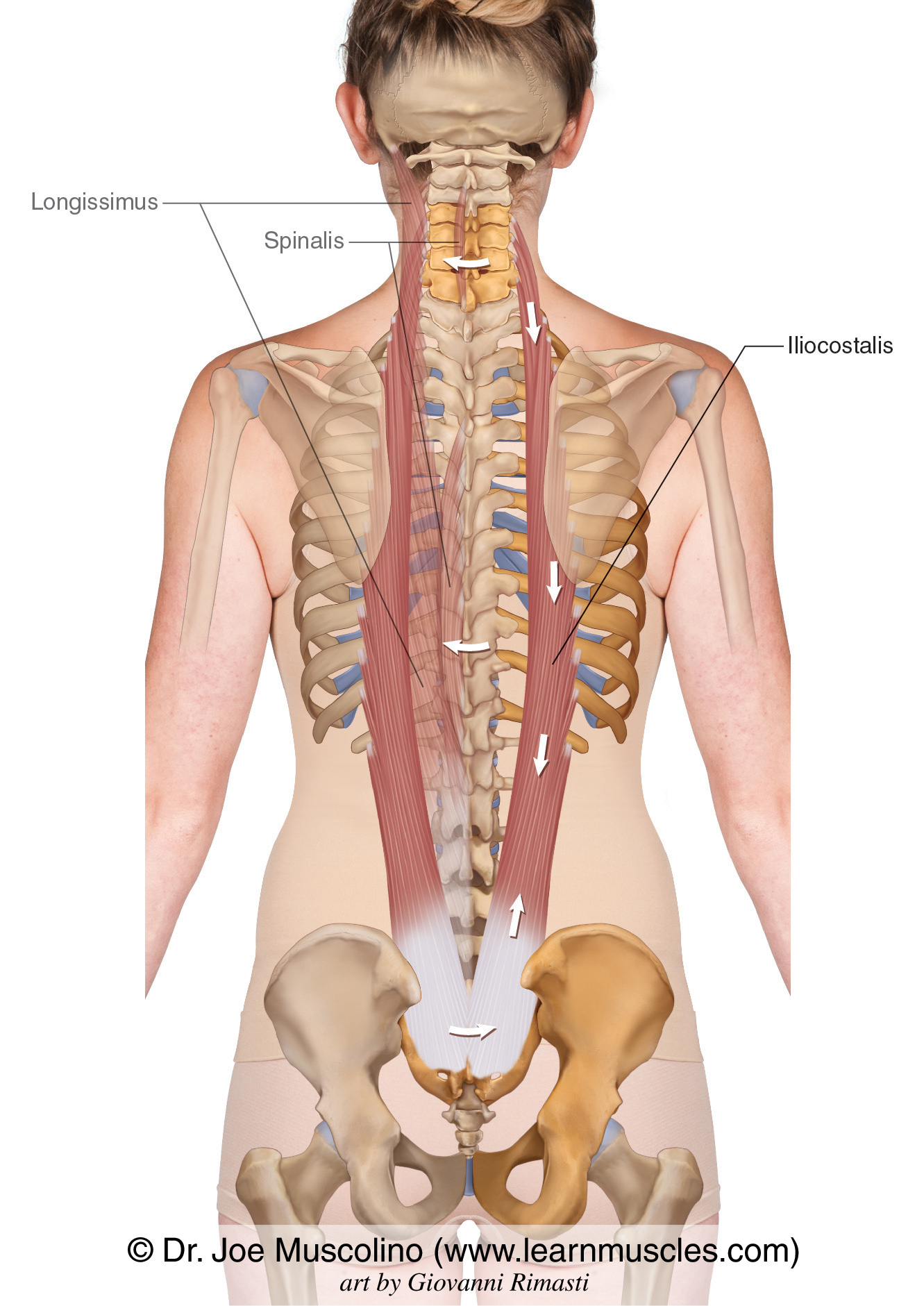
iliocostalis
intermediate deep back: erector spinae
most lat
3 dif segments: cervicis thoracis lumborum
extension
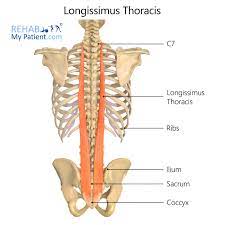
Longissimus
intermediate deep back: erector spinae
middle
3 dif segments: cervicis thoracis lumborum
extension
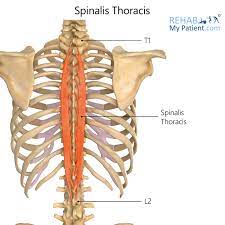
Spinalis
intermediate deep back: erector spinae
most medial
3 dif segments: cervicis thoracis lumborum
extension
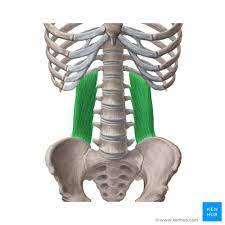
Quadratus Lumborum
square like
O: iliac crest
I: rib TPs
A: forced inhalation
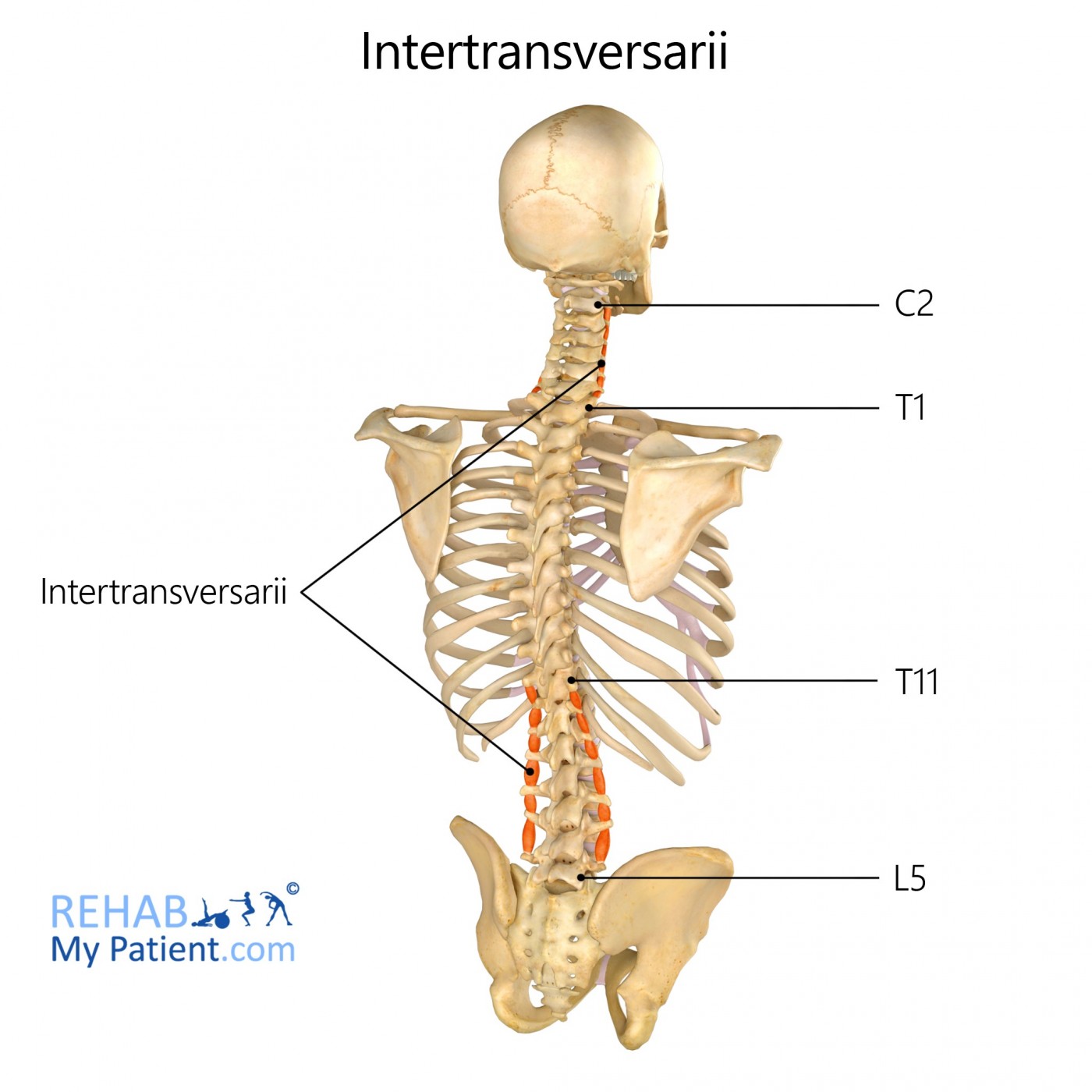
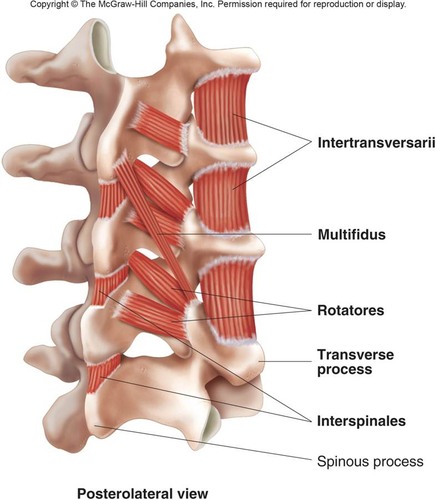
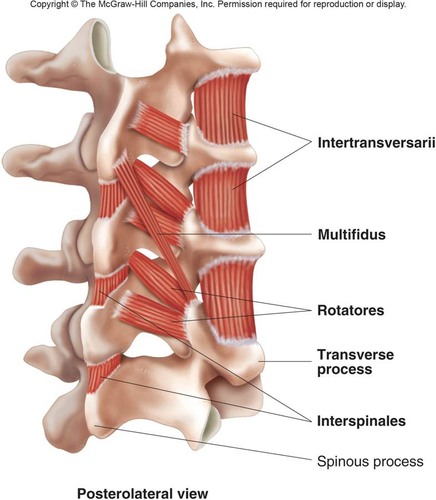
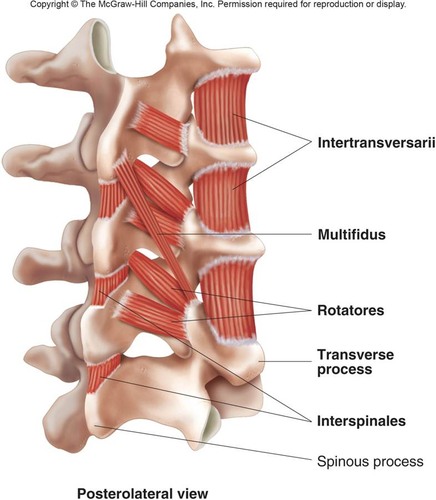
Intertransversarius
Deepest Back: stabilize spine, small movements
O/I: btwn TPs L5-C1
A: lat flex
Rotatores
Deepest Back: stabilize spine, small movements
O/I: btwn TPs L5-C1
A: rotation
Multifidus
Deepest Back: stabilize spine, small movements
O/I: btwn TPs L5-C1
A: rotation
Interspinales
Deepest Back: stabilize spine, small movements
O: SP C3-T1
I: SP C2-C7
A: prevent flex
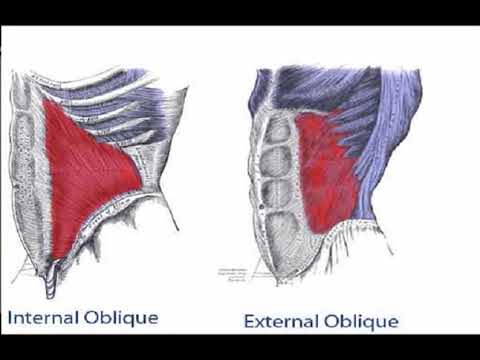
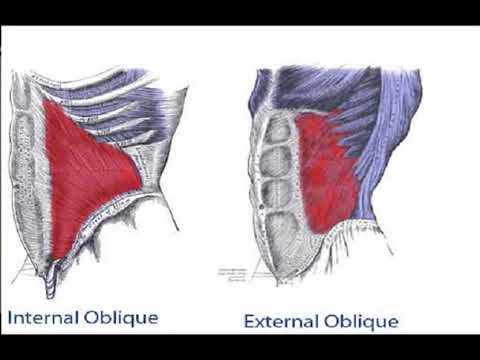
ext oblique
Ant trunk
O: ext surface ribs 5-12
I: iliac crest, pubic tubercle, abdominal aponeurosis
A: rot to opposite side
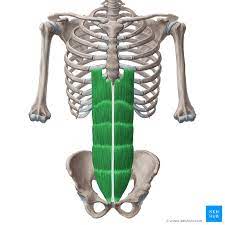
Rectus abdominus
O: Pubic crest/symphysis
I: ribs 5-7, cost cart, diploid process
A: flex, mild lat flex
Int oblique
O: thoracolumbar aponeurosis, iliac crest, inguinal lig
I: int surface ribs 10-12, abd aponeurosis
A: trunk flex bilat. ipsi lat flex/rot
Transversus abd
O: Int surf ribs 7-12
I: abd aponeurosis
A: Abd muscles compress + support abd organs
Breathing muscles
Diaphragm
rib cage
abdominal muscles
Elbow Joints
[ ] 3 synovial joints in same articular cavity/capsule
Humeroulnar joint (hinge/trochlear): flexion/extension
Btwn trochlear notch of ulna and trochlea humerus. Hinge/trochlear joint
Bony congruency (strong concave/convex connection). Very stable, enhanced by strong capsule + ligaments
Flexion, coronoid process of ulna enters coronoid fossa humerus (stops with biceps)
Extension.
Ulnar vagus: approx 15 deg (w>m). Axis of movement is not 100% frontal -oblique due to orientation of trochlea. >15 excessive.
Humeroradial joint: hybrid ball and socket: flex/extension +pronation/supination DOES ALL MOVEMENTS
Btwn fovea radial head and capitulum of humerus
Spheroid
Poor bony congruency/stability
Movements dictated by two other joints of elbow (flex ext-ulna) (rot long axis pron/sup)
Proximal radioulnar joint: pronation/supination
Btwn head radius + radial notch of ulna
Trochoid
Pron/sup w/distal counterpart
Head of radius and radial notch, held by annular (deep surface hyaline+fibrocartilage to allow motions) and quadrate lig
Distal radioulnar joint
Btwn head of ulna + ulnar notch radius
Poor bony congruency
Held together by capsule, ligaments + arctic disc btwn head of ulna and carpal bones
Elbow stability
Medial blow: increases vagus
Lateral blow: increases varus
Elbow injuries must have weight
Little league elbow results in soreness/fractures/ripped ligaments (fractures to growth plate, evulsion fracture- lig pulls out piece of bone) Stability btwn radius and ulna
interoseuss membrane: +stability, greater SA for muscle attachment for muscles forearm, hand, fingers
Oblique cord
Distal oblique fibres
Hiatus: openings in soft tissue for blood vessels + nerves
Good bony congruency therefore stable joint
ROM elbow
ROM ELBOW:
Flex: active= 120/pass 140
Ext: 0 to -5 (hyperextension)
Pron/sup: 80-90
Radius bony landmarks
Head (prox)
Radial tuberosity (medial)
Styloid process (lateral)
Superior aspect: fovea
Ulnar notch
Bony landmarks ulna
olecranon process
Radial notch (lateral)
Trochlear notch
Coronoid process
Ulnar tuberosity
Styloid process (med)
Head (dist)
[ ] Bone coverage is high at articular surfaces : very stable, bones fit together really well. Baseball -bone issues
Distal humerus two distinct surfaces
Distal humerus two distinct surfaces
Trochlea w/trochlear notch of ulna
Capitulum (head) articulating w/ head of radius
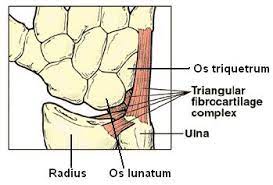
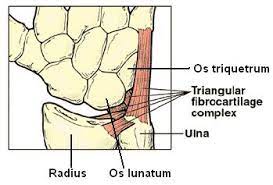
Triangular Fibrocartilage complex
Fibrocart disc dist radioulnar
Edges continuous with radioulnar capsular ligs
Keeps head of ulna snug against ulnar notch radius
stability ulnocarpal joint
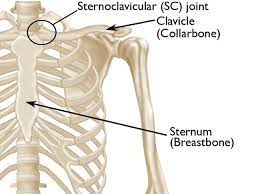
Sternoclavicular joint
attach upper body to thorax
saddle: post/ant rot, elev/dep
Movements: elevation (35-45), dep (10), pro/ret (15-30), ant rot (none), post rot (20-35). Flex/add most common injuries
Stabilized by ant/post SC ligs, art dis, interclavicular lig, costoclavicular lig (ant +post bundles: stabilize).
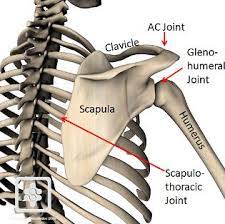
Scapulothoracic
false joint (muscle - muscle gliding)
up down rot, add/abduction, elev/dep
allows GH +ROM
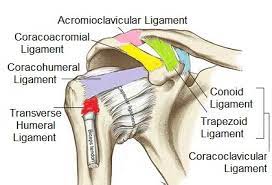
accromioclavicular joint
articulates w/acromion. Planar joint, accomodates GH
stabilized by disc, acromioclavicular/coracoacromial/coraclavicular (conoid-med, trapezoid-lat) ligs
Clavicle landmarks
Costal facet 1st rib, costal tub, subclavian grrove, conoid tubercle (coracoclavicular ligs attach)
Serratus ant
attaches on to ribs + ant scapula. ext rot/protraction
Muscles of scapula attach tvert spine latissimus dorsi, iliac crest, thoracolumbar fascia. functional +
Humerus
unstable, hum head> glenoid fossa. Reduced space=pain by raised glenoid fossa head
135 def= incline angle btwn head and shaft. 30 deg retroversion hum (back) vs dist hum.
humerus landmarks
ANT
lesser tubercle: subscapularis, lats, terres minor
greater tubercle: supraspinatus, pec major
POST
deltoid tuberosity
lesser tub: infraspinatus, terres minor
radial groove: radial nerve, innervates all upper extremity
anatomical neck: shoulder joint/hum head
Surgical neck: mid epiphysis
Glenohumeral
mobility>>> stability
ball and socket
cavity deepened by glenoid labrum but not enough to be stable
ligs lax w/ repetitive movement, very common injury
subacromial bursae and supraspinatus are often squeezed leading to tendonopathy, bursitis
Movements= f/abd(120+60-scap/hum=180), e(65), add(50-75), c(200)
Glenohumeral ligs
Sup glenohumeral: anatomic neck above lesser tub. ext rot and inf/ant translation hum head
Mid ““: anatomic neck/scapularis. Ant translation hum head 45-90 deg add, ext rot
Inf ““: 3 parts, ant/post band and axillary pouch. broad sheet post inf anatomic neck. Ax pouch: 90 deg abd + ant post + inf trans. Ant band: ““ + full ext rot + ant trans, Post: full int rot.
Coracohumeral: ant greater tub, goes to supraspinatus
Scapulohumeral rhythym
ROM at dif joints to obtain full ROM. abd. GH=120+20-40GH ext rot. ST=60 up rot+ 20 post tilt +0-5 ext rot. SC= 25 SC post rot. AC= 30 upward rot
Upper trapezius
Elevators
O: ext occipital protuberance, ligamentum nuchae
I: acromion and lat 1/3 clav
A: ““ upward rot scap
Levator Scapulae
Elevators
O: TPs C1-C5
I: sup angle scap
A: ““
Rhomboid Minor
Elevators
O: SPs C7-T1
I: med border spine scap
A: ““ retraction
rhomboid major
Elevators
O: SPs T2-T5
I: med border scap below spine
A: ““ retraction
Lower trapezius
Depressors
O: SPs T4-12
I: spine scap
A: ““ retraction, upward rot scap
Latissimus Dorsi
Depressors
O: SPs T6-L5, ribs 10-12, iliac crest
I: inf angle scap + med border intertub groove hum
A: ““ ext/add/int rot hum
Subclavius
Depressors
O: 1st rib
I: subclavian groove clavicle
A: ““ stabilize scap
Serratus Anterior
O: ant ribs 8-9
I: ant med border scap
A: protract+upward rot scap. Maintains scap to T wall
Pec minor
O: ant surf ribs 3-5
I: coracoid process
A: protraction/downward rot
Middle trapezius
O: SP C7-T4
I: acromion+spine scap
A: retract/upward rot scap
Pec major
O: med 1/3 clavicle
I: lat border intertubercular groove
A: flex/add/int rot/ horizontal add
Biceps Brachii (long head)
O: supraglenoid tub (labrum)
I: radial tub and biceps aponeurosis
A: flex/abd shoulder, flex/sup forearm.
Coracobrachialis
O: coracoid process of scapula
I: ant med surface, hum disk, crest of lesser tub
A: flex/add shoulder
Latissimus Dorsi
O: SP T6-L5, ribs 10-12, iliac crest
I: Inf angle of scap + med intertubercular groove
A: dep scap, ext/add/int rot hum
Teres major
O: post inf angle scap
I: med border inter tubercular groove
A: ext/add/int rot hum
Triceps brachii
O: infraglenoid tubercle
I: ulna olecranon
A: ext add shoulder, elbow ext
post deltoid
O: inf border spine scap
I: delt tub
A: ext +ex rot shoulder
Middle deltoid
O: acromion
I: delt tub
A: abd
Supraspinatus
O: supraspinatus fossa scap
I: sup greater tubercle
A: 15 deg abd+ ext rot (rotator cuff)
compresses head into glenoid fossa to restrict sup translation of hum. issue: compression between hum head and acromion
Infraspinatus
O: infraspinatus fossa
I: greater tub
A: lat rot (rotator cuff)
dep hum head
Subscapularis
O: subscap fossa
I: lesser tub
A: med rot +add shoulder (rotator cuff)
dep hum head
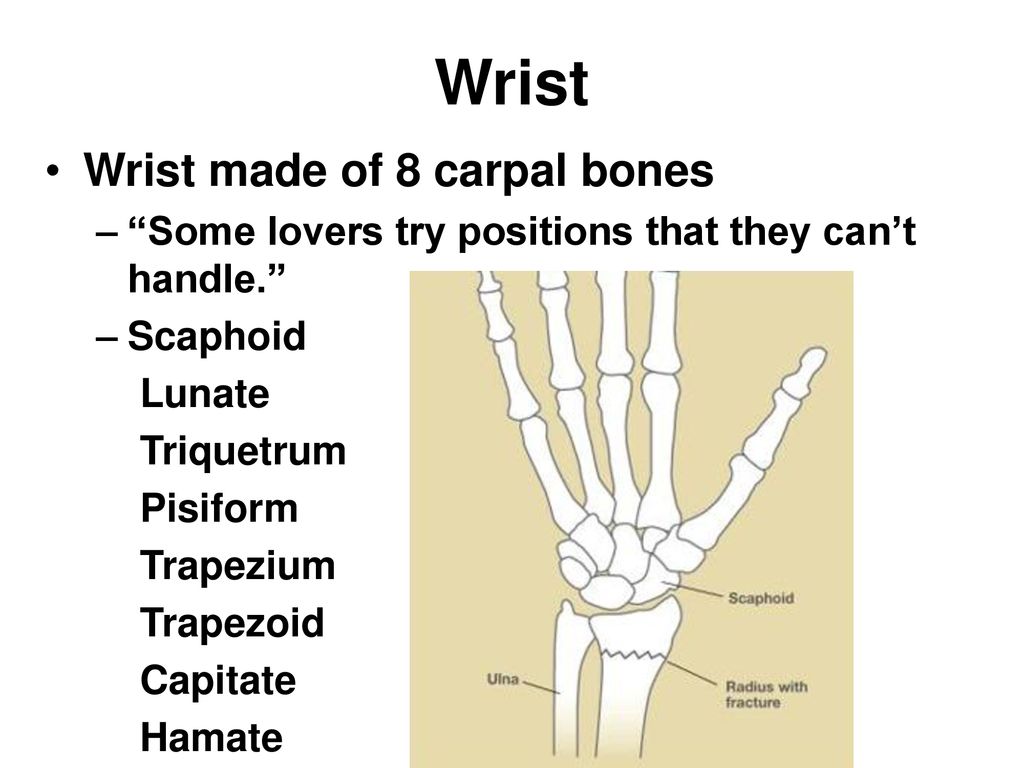
Carpal Bones
Some Lovers try positions that they cant handle
Scaphoid -necrosis if injured, needs surgery
Lunate - most moveable
Triquetrum - triangle shaped, connects w/ulna in ulnar deviation
Pisiform - embedded within flexor carpi ulnaris
Trapezium
Trapezoid - small solid
Capitate - all axis of motion
Hamate - hook for structures to pass to pinky
Palmar tilt
limits extension



![<p></p><ul><li><p>[ ] 3 synovial joints in same articular cavity/capsule</p></li></ul><p>Humeroulnar joint (hinge/trochlear): flexion/extension</p><ul><li><p>Btwn trochlear notch of ulna and trochlea humerus. Hinge/trochlear joint</p></li><li><p>Bony congruency (strong concave/convex connection). Very stable, enhanced by strong capsule + ligaments</p></li><li><p>Flexion, coronoid process of ulna enters coronoid fossa humerus (stops with biceps)</p></li><li><p>Extension.</p></li><li><p>Ulnar vagus: approx 15 deg (w>m). Axis of movement is not 100% frontal -oblique due to orientation of trochlea. >15 excessive.</p></li></ul><p></p><p>Humeroradial joint: hybrid ball and socket: flex/extension +pronation/supination DOES ALL MOVEMENTS</p><ul><li><p>Btwn fovea radial head and capitulum of humerus</p></li><li><p>Spheroid</p></li><li><p>Poor bony congruency/stability</p></li><li><p>Movements dictated by two other joints of elbow (flex ext-ulna) (rot long axis pron/sup)</p></li></ul><p></p><p>Proximal radioulnar joint: pronation/supination</p><ul><li><p>Btwn head radius + radial notch of ulna</p></li><li><p>Trochoid</p></li><li><p>Pron/sup w/distal counterpart</p></li><li><p>Head of radius and radial notch, held by annular (deep surface hyaline+fibrocartilage to allow motions) and quadrate lig</p></li></ul><p></p><p>Distal radioulnar joint</p><ul><li><p>Btwn head of ulna + ulnar notch radius</p></li><li><p>Poor bony congruency</p></li><li><p>Held together by capsule, ligaments + arctic disc btwn head of ulna and carpal bones</p></li></ul><p></p>](https://knowt-user-attachments.s3.amazonaws.com/47f9d4efbfa245bf8699a5a6d13b8aaf.jpeg)