Drugs and Behavior Exam 1
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
Addiction
Repetitive, compulsive behavior of a person despite negative consequences to life and health
Examples of Addiction
-drugs, alcohol, internet use and video games
-things we are addicted to can feel good
-positive and negative reinforcement
-classical conditioning
-no difinitive demarkation
DSM-5
-Used to determine disorder by checking for symptoms and severity
-only need 2+ symptoms
-alcohol
-canniabis
-hallucinogen
-inhalant
-opioid
-sedative, hyponitc, anixolytic
-stimulant
-tobacco
The Disease Model
-Alcohol/drug addiction is an involuntary physical illness
-hereditary, medical nature
-works like an allergy
-no cure: no acceptable usage
Arguments for Disease Model
-conveys seriousness of addiction
-relieves guilt and increase help seeking behavior
-evidence that addiction nearly inevitable following prolonged drug use
Arguments against Disease Model
-Argue that no such disease exists
-scientifically indefensible
-strips person of freedom and responsibility
-labelling as incurable diseases is stigmatizing
-fails to consider complex factors
-many people eventually stop using on their own
Addiction Is A Choice Model
-Individuals have free will to decide to engage or not in addictive behaviors
-deeply ingrained habit and/ or result of learning history
- includes theory of addiction as physical dependence--tolerance and withdrawal, occur with repeated use
Arguments For Choice Model
Biology/physiology alone cannot determine whether someone will use a drug.
People can get better on their own, and can use moderation.
Arguments Against Choice Model
Can have dependence without addiction
Can have addiction without dependence
Psychology's Understanding Of Addiction
-called "disorders" not "diseases"
-view addiction as stemming from multiple variables;
-biology
-environment
-motives
-learned experiences
Why Study Drug Use?
-Prevalence rates
-consequences of use
-drug effects/ abuse potential
-risk factors for use
Types Of Research Designs
-descriptive/correlational: Positive and negative, move in same direction or in opposite directions
-experimental: IV and DV, experimental and control groups
- quasi- experimental: affects behaviors, no random assignment
General Issues with Human Subject Research
Risk/ Benefit: need to outweigh chances of risk, lower risk better the benefit
Informed Consent: Tell what risks are and if they'd like to continue, be careful around people who are long time substance users
Subject Selection; experience with drug, but no addiction, drug naive, people already using but also offer treatment, but not people who are in recovery
Confidentiality: # of precautions, data leakage, give people numbers, usually federal funding
Deception: researcher doesn't fully inform about what they may experience, need to tell truth at the end
Payment: compensation for participating
Do drug users have impaired capacity to provide consent?
-Drug users self report no impairments
-Most research finds drug users to have similar recall of IC as non- drug users
Paying Drug Users Coercive?
-Financial motivations do play a part in participating but money alone is not enough
-Cash vs. Non cash payments did not alter drug use or perceptions of coerciveness but increase retention
Who monitors/approves ethical research
_ Institution Review Boards (IRB)
-Institutional Animal Care and Use Committee (IACUC)
Measuring nonhuman behavior
-Spontaneous motor activity
-Stereotyped behavior : rats bob heads
-Paw licks : pain relief
-Elevated plus maze :reduced anxiety
Ratio
Number of behaviors
-fixed ratio; same number of behaviors over and over
-variable ratio; set of numbers change overtime find average over trials
Interval
passage of time
-fixed interval; set amount of passage of time: runs for 5 minutes and gets a reward and repeat
-variable interval; passage of time, average time over : 4 times a year, never know when it is coming
classical conditioning
Associative learning
-relative to tolerance and withdrawal
-conditioned ---> unconditioned
-the CS predicts the US
-the UR is the same as CR ( most of time)
-CR preparing for the US

Operant Conditioning
-consequence learning
-relevant to reinforcement value of drugs
-1.) what is the persons original behavior? Increasing or Decreasing?
-2.) does the consequence of behavior involve something being added or removed?
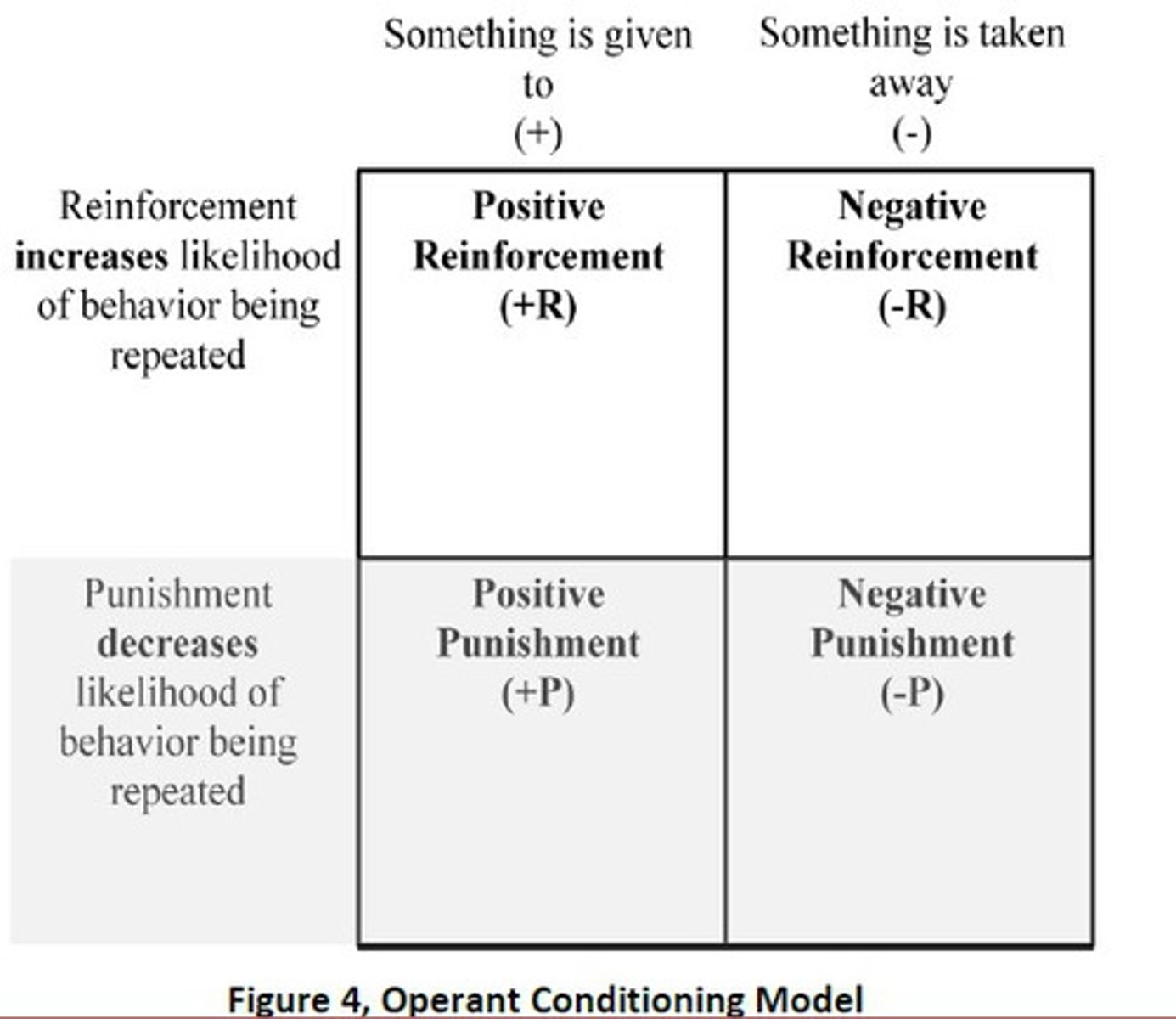
disciminative stimulus
In environment to behave someway in its presence or absence. " if a cop is around you slow down'
Pharmacology
Scientific study of the actions of drugs and their effects on a living organism
Psychopharmacology
Scientific study of the actions and their effects on behavior
Pharmacokinetics
The process by which drugs are absorbed, distributed within the body, metabolized, and excreted.
What is a Drug?
A substance that is taken deliberately that alters the physiology of the body but is not a food or nutrient and is not taken for taste or sustenance.
-to get high and achieve certain feelings or to treat disorder
-Psychoactive Drug: drug that affects processes like thoughts memories and behaviors
Drug Names
chemical- molecular structure
generic- legal name
trade- trademark name
Drug Effects
Depends on:
Types of drugs
Dosage
Route of administration
The user
Dose Response Curves
Understand the full range of physiological and behavioral effects of a drug
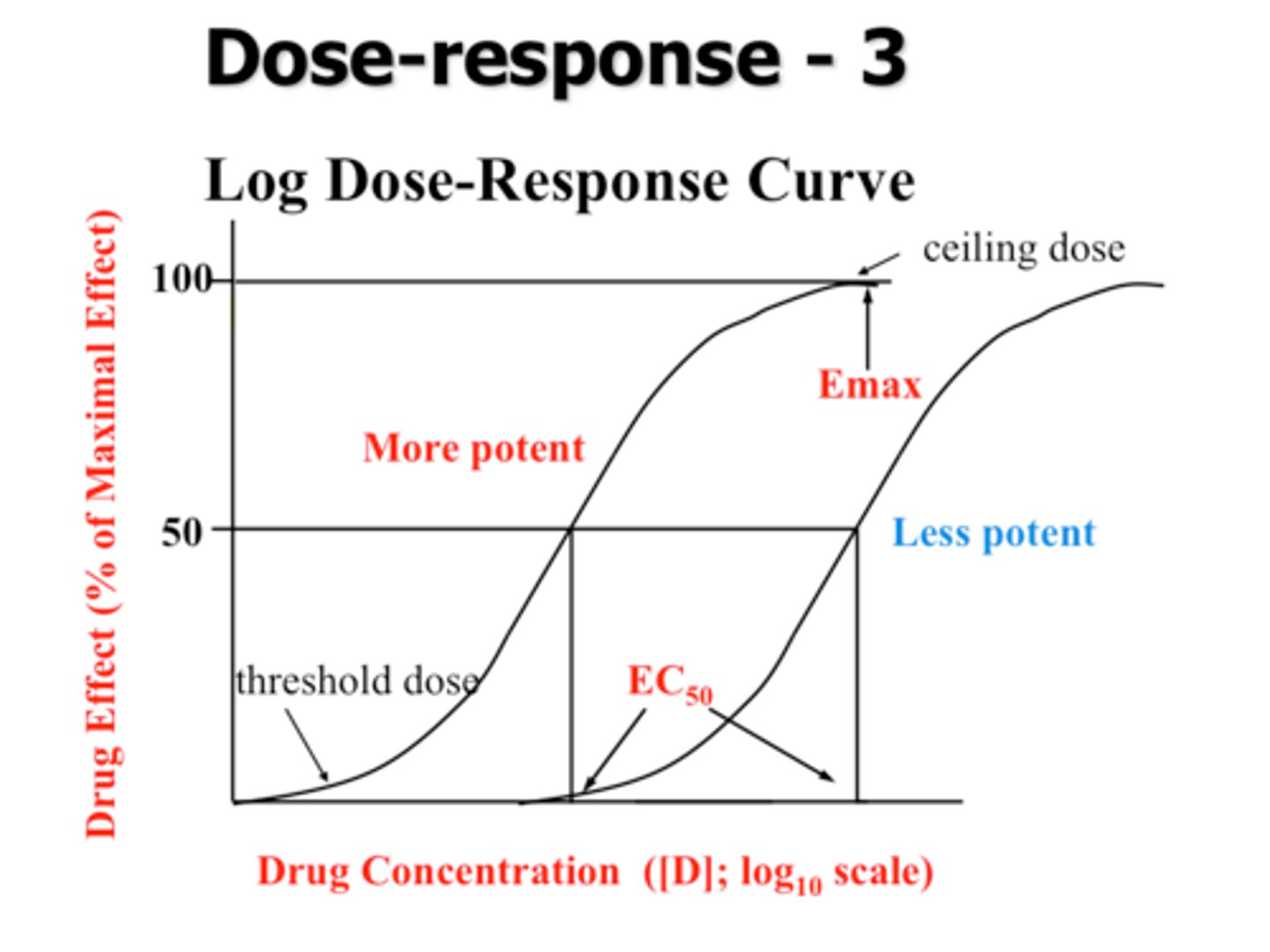
Threshold
Minimum dose required for any effect
Efficacy
Maximum effect obtainable
Potency
Dose required to elicit an effective response, dose on average for relief
Slope
Depicts the difference in dosage between eliciting a small effect and maximal effect
Shallow: change dose substainally to see an effect
Steep: change dose a bit and see effect
Drug Safety
ED50: Therapeutic, median effective dose
LD50: Toxic, median lethal dose
Therapeutic Index : LD50/ED50
-Smaller number is dangerous
-Larger number hard to overdose on
Routes of Administration
Affects of Bioavailability: portion of original drug dose that reaches site of action. How much will it take for the drug to reach the brain for effects?
Oral
safe, all of drug doesn't enter bloodstream, takes longer to work, but lasts longer
-lower bioavailability
Rectal
not common, used when person is unconscious or vomiting
Transdermal
skin, usually mixed with something to be absorbed
-nicotine patch, fetynal patch
-delay to effects but long lasting
Mucous
snorting, absorbs in mucous membrane in nose or put in mouth to dissolve
-cocaine
-intermediate, quicker than oral but not like inhalation
-shorter than oral
Inhalation
smoking, inhaling smoke with drug molecules from lungs to blood; moth, tobacco
-fast doesn't last long, low bioavailability
Injection
right into blood, short length, instant
Distribution of Drug
Receptors in brain
-reaches through bloodstream
At any time, only a small portion of total amount of drug is in contact with receptors
-most drug found is areas of the body remote from site of action
-explains side effects
Influence of Lipid Solubility
High lipid soluble: can be readily passed through membranes to blood
Low lipid soluble: cant be readily absorbed and passed through membranes, usually stay in water and break down
-drugs really lipid soluble, our body fat takes it in and not effects administered. Releases it in small amount, reduces bioavailability
Termination of Drug Action
Most drug leaves body through urine
-either as unchanged molecule or as metabolite
-involves kidney and liver
Half Life
Period of time required for the concentration of a drug in body to be reduced by half
-usually eliminated in body by 6 half lives
Drug Testing
The metabolite of a drug is in our body, cant say specifically what drug is used because many drugs have the same metabolite
-high lipid solubility makes it stay in systems longer
Placebo
Nothing about drug is creating it, you are expecting effects
-feeling more awake after sip of coffee
-placebo is wanted
Nocebo Effect
An effect that is being experienced but not a wanted one
-jittery from coffee, side effect
Drug Scheduling
Schedule I: High abuse potential and no current medical uses.
II: High abuse potential, but there are current medical uses.
III: Slightly less abuse potential, but high psychological dependence.
IV: Even less abuse potential
V: Even less abuse potential
Hindbrain
Medulla
-coordinates basic life support systems
Cerebellum
-balance and motor control
* affected by depressants and sedative drugs
Midbrain
Center for control of important sensory and motor reflexes
-Substantia Nigra
- control of body movements
Ventral Tegmental Area (VTA)
-cognition, motivation, addiction, intense emotion
Forebrain
Basal Ganglia
-includes the nucleus accumbens and striatum
-motor movements
-plays role in dopamine
Hypothalamus
-motivatied behaviors for survival, homeostasis
Limbic System
-hippocampus and amygala
-memory, emotion, reward
Prefrontal Cortex
-complex cognitive behavior, personality, decision making, and social behavior
Neurons
Communicate with another to govern behavior.
Dendrites; get a chemical message from the neuron in front of it
messages passed down to axon to the terminal buttons then release neurotransmitters
-synapse; space between neurons
Neuronal Communication
-Electrochemical Event
-Action Potential
intra-neuron process, passing electrical current to another neuron
electrical signal
occurs during opening of ion channels
-Neurotransmission
interneuron process
chemical signals
Reuptake
Neurotransmitters are reabsorbed back into the presynaptic neuron after they have transmitted a signal to the postsynaptic neuron
Drugs and Neurotransmission
-drugs can effect release of neurotransmitters
-drugs either speed up or slow down or block reuptake process
-increase or decrease how much enzyme is in neurotransmitter
-some drugs look similar to neurotransmitters molecularly, and can get into the synapse pretending to be it, to pass along a message that does not belong. Or they can block the real neurotransmitter to pass message.
Agonist
Drug increases action of neurotransmitter and availability
Antagonist
Drug decreases action of neurotransmitter and availability
Major Neurotransmitters
Acetylcholine- Nicotine
Serotonin and Epinephrine: Psychedelic drugs
Endorphins: opioids
Glutamine: alcohol
Dopamine: 2 major pathways dopamine is released
-Nigrostriatal: motor movements
-mesolimbic: reward
Drug Tolerance
Progressively decreasing responsiveness to a drug
Pharmacokinetic tolerance
increased metabolism due to regular use.
-before drug reaches brain and destroys it, have to take larger dose so it doesn't break down as fast (enzymes)
Pharmacodynamic tolerance
NT adjustments to compensate for drug effects
-shut down dopamine receptors and neurotransmitters
Conditioned tolerance
classical conditioning of environmental cues to predict drug, and elicits CR opposite to UR
-conditioned response is not the effect of the drug itself, but the body's attempt to resist it
-explains human overdose
Cross tolerance
tolerance effect for one drug can automatically induce tolerance for another
occurs because different drugs may bind to the same receptors in brain
Sensitization
"reverse tolerance"
in some cases the effect of the drug may increase with repeated administrations of the same drug
- may be conditioned, similar to tolerance
Withdrawal
Compensatory adjustments of homeostatic mechanisms to the effects of drugs after administrations
-physical and mental symptoms from opposite drug effects by not using
all symptoms are negative
Withdrawal and Opponent Process Theory
-Drug stimulates A process ( euphoria, stimulation)
-Compensatory B process evoked ( dysphoria, sedation)
-With continuous use, A process remains constant but B process strengthens
-A process: drug effect, never changes
-B process: cancels out A process, changes over-time
OPT and Classical Conditioning
CSa; previously neutral stimuli preceding A state
-independently capable of producing pleasurable A process and ultimately B process
-Drug effect, a process
CBs: previously neutral stimuli preceding B state
-independently capable of producing aversive b process
-environmental effect, process, withdrawal
What is Craving
1.) urge reflects a broader spectrum, craving is an urge but really strong
2.) reinforcing effects, intent to use drugs
3.) stable or momentarily- depends
Basic Theories of Addiction
Drugs are administered because they act as reinforcers
-Problem: Positive reinforcement paradox: when reinforcing behavior with rewards can lead to negative outcomes
Opponent Process Theory
Effects of drug automatically counteracted by opposing actions in the body (to maintain homeostasis)
-Explains compulsive drug use as a negative reinforcement process
-A process: Driven by brain rewards systems
-B process: Craving, driven by anitreward systems
-Both withdrawal and craving
OPT cont
- B lasts a long time and is extremely adverse
-eliciting A process is effective in removing B process
- drug users learn to use the drug to elicit A to rid of B
-amounts of drug used need to increase to keep A-B greater than 0
-exposure to both CSa and CSb ultimately result in more craving
-explains challenges of quitting: weaken b to withstand A
Hedonic Dysregulation Theory
-A process: driven by brain reward systems: positive emotions
-B process: driven by brain anit-reward systems: negative emotions
Homeostasis: optimal constant set point
Allostasis: Changing set point in response to environment
-More A and B elicited the more our mood goes down
-Tolerance goes up as allostatic goes down
-experiencing bad mood all the time, not momentarily
-need to increase dose (A) to feel something, but also (B) goes down more
incentive-sensitization theory
-Positive Reinforcement
-seeking out reward, not about positive mood
-No A or B process
-Dopamine = positive reinforcement
Motivational Circuitry
1.) need state detected by motivation control system
2.) discovery of reward causes release of dopamine (reward related stimuli acquire incentive salience)
3.) when future need state arises, general activity increases but behavior is guided more toward reward- related stimuli
4.) simply observing these reward- related stimuli releases dopamine ( results in approach behavior, even if not in need state)
Incentive Salience
cues associated with reward, quickly grab attention in future, faster (CS)
Dopamine
-nothing to do with learning
-positive reinforcement
-reward DOES NOT equal pleasure
-reward and reinforcement neurtransmitter
Dopamine Release
1.) When there is a homeostatic need (activates motor behavior)
2.) When we were rewarded (to develop incentive salience)
3.) To signal reward is in the environment ( craving)
Drugs as Reinforcers
-Satiatied Mechanism: "fullness", how you feel full when you drink water so you do not want anymore, not the case with drugs
-Immediacy/ intensity; more dopamine response if drug is much higher than in natural resources
Incentive Sensitization Theory & Motivational Control System
-Motivational circuitry helps us get our need met (reward) when we have a homeostatic need
-when rewarded, dopamine is released to develop incentive salience
-activated even when not in a need state
-sensitization results in huge dopamine surge in response to drug related cues
-positive reinforcement; substance use maintained due to addiction of motivational sensitization
Incentive Sensitization Theory & Motivational Control System CONT
-homeostatic input: drug to get homestatic
- U.T.A + N.A = release of dopamine to basal ganglia
-Basal Ganglia = triggers motor movement
-Hippocampus + Amygala= release drug feelings to memory
-ALL of this will remind one where they get drug from (CS)
-incentive salience so strong activates entire circuitry when reward is " near"
- explains compulsive drug use
-silent on withdrawal
Types of Cognitive Processing
- Controlled Processing
Dependent on attention
Slow
Flexible
Subject controlled
Serial
-Automatic Processing
Independent of attention
Fast
Stimulus bound
Somewhat beyond subject controlled
Parallel
Cognitive Processing Model
Schemata: mental framework that tells you how to behave, automatic drug use action plan
- Theory explains most instances of repeated compulsive substance use behavior as automatic processes that're triggered by various environmental stimuli. When triggered, activates automatic drug use behavior.
-Habitual
-ONLY automatic behaviors are stored in this schemata
-Craving is conceptualized as controlled processes
-most of time, we are not using because of craving, but not ignoring it
Cognitive Processing Model and Craving
-Schemata is involunarily or voluntarily blocked
-The mental effort needed to engage and deal with blockages is the craving
- using because of habit not craving
-craving not apart of schemata, only when blocked