[BOOK] HOST MODULATION
1/43
Earn XP
Description and Tags
chap 48
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
Host Modulatory Therapy (HMT)
Adjunctive treatment → used in addition to conventional therapies
Focuses on modifying the host response, not just bacteria
Conventional Periodontal Therapy
Mechanical:
Surgery
Scaling and root planing (SRP)
Early adjunctive therapies:
Antiseptics
Antibiotics (local/systemic)
Purpose of HMT
reduce destructive inflammatory responses
enhance protective and healing responses
balance shifts toward:
healing (resolution of inflammation, tissue repair)
away from disease progression
Why HMT is Needed
SRP reduces bacteria but:
Does not eliminate all bacteria
Recolonization occurs
Host response causes most tissue destruction
Helps manage risk factors:
Smoking
Diabetes
Genetic susceptibility
Can increase anti-inflammatory/protective mediators
How HMT Works
Does NOT stop normal defense or inflammation
Modulates excessive/pathologic inflammation
Targets:
Enzymes
Cytokines
Prostanoids
Regulates:
Osteoclast activity (bone resorption)
Osteoblast activity (bone formation)
Maintains normal tissue turnover
other inflammatory conditions that benefit from HMT
Arthritis
Cardiovascular disease
Dermatologic conditions
Diabetes
Rheumatoid arthritis
Osteoporosis
Existing Medications with HMT Effects
NSAIDs
Bisphosphonates
Tetracyclines
Cytokine-targeting drugs
Drug Classes Studied for HMT
NSAIDs
Bisphosphonates
Tetracyclines
Enamel matrix proteins
Growth factors
Bone morphogenetic proteins
Systemically Administered Agents
Used as host modulatory therapy (HMT)
Affect the whole body, not just local periodontal tissues
MOA of NSAIDs
Inhibit prostaglandin production (especially PGE2)
PGE2:
Increases bone resorption by osteoclasts
Inhibits fibroblast function
Modulates immune response
Result:
Reduced inflammation
Decreased osteoclast activity
Not indicated for periodontal HMT
examples of NSAIDs
Aspirin (salicylates)
Indomethacin
Ibuprofen
Flurbiprofen
Naproxen
NSAIDs Effects in Periodontal Disease
Slows alveolar bone loss with long-term use
Requires daily use for extended periods (up to 3 years)
Significant side effects of NSAIDs
Gastrointestinal problems
Hemorrhage (↓ platelet aggregation)
Kidney (renal) impairment
Liver (hepatic) impairment
Rebound effect:
Bone loss returns or accelerates after stopping drug
COX-2 Inhibitors
Target COX-2 enzyme → reduce inflammation
Initially promising (fewer GI side effects)
Later found to cause serious adverse effects
Some drugs withdrawn from market
Not indicated for periodontal HMT
MOA of Bisphosphonates
Inhibit bone resorption by disrupting osteoclast activity
May:
Interfere with osteoblast metabolism
Reduce collagen breakdown (anticollagenase effect)
bisphosphonates effects in Periodontal Disease
Increase bone density
Improve alveolar bone status
Reduce bone resorption (animal and human studies)
side effects of bisphosphonates
Inhibit normal bone calcification
Alter white blood cell counts
Risk of osteonecrosis of the jaw:
Especially after dental extractions
More common with intravenous use
Sub-Antimicrobial-Dose Doxycycline (SDD)
20 mg dose of doxycycline (Periostat)
Used as an adjunct to scaling and root planing (SRP)
Indicated for chronic periodontitis
Only systemic HMT:
Approved by FDA
Accepted by ADA
dosage of SDD
20mg, twice daily
Duration:
3 months standard
Up to 9 months maximum
MOA of SDD
Not antibacterial at this dose
Works by:
Inhibiting enzymes
Reducing cytokines
Decreasing osteoclast activity
side effects of SDD
No detectable effect on:
Oral flora
Bacterial flora in other body sites
Provides clinical benefits when combined with SRP
Oracea
Modified-Release SDD
Approved for rosacea (skin condition)
Also studied in periodontitis:
Showed greater clinical benefits than SRP alone
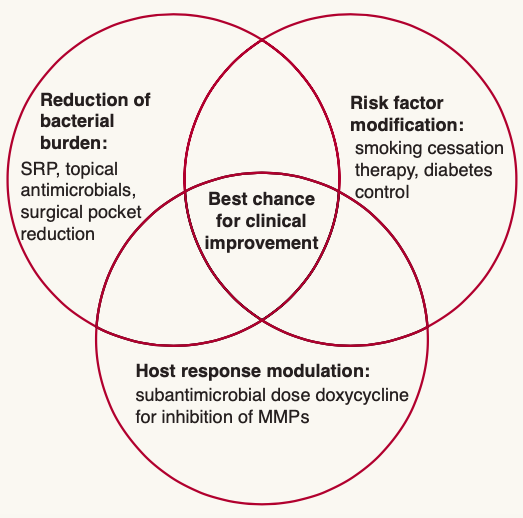
treatment strategies in periodontitis
Locally Administered Agents
Applied directly to periodontal sites
Used as adjuncts, often with surgical procedures
Not approved as local HMTs for periodontitis
Approved by FDA for surgical adjunctive use
examples of locally administered agents
topical NSAIDs
enamel matrix proteins (Emdogain)
Insulin-like growth factor
platelet-derived growth factors (GEM 21S)
bone morphogenetic proteins (BMP-2 (INFUSE) BMP-7)
examples of Topical NSAIDs
Ketorolac mouthrinse
Ketoprofen (local use)
effects of Topical NSAIDs
Reduce PGE2 levels in gingival crevicular fluid (GCF)
Decrease inflammation
May halt bone loss
EMP, GF, BMP
Improve wound healing
Promote regeneration of:
Bone
Periodontal ligament
Cementum
Assist in:
Clinical attachment gain
Bone regeneration
Ridge and sinus augmentation
Management
is broader than treatment
Focus on long-term control of a chronic disease
management includes
Medical and dental history
Clinical exam and radiographs
Risk factor assessment
Diagnosis and treatment planning
Reevaluation and maintenance
Prognosis assessment
indications of HMT
Patients with:
Nonmodifiable risks (genetics)
Difficult-to-modify risks (smoking, diabetes)
Avoid taking with calcium
Risk Factor Modification
Smoking
Major risk factor
Reduces treatment success
Smoking cessation is essential
Diabetes
Poor control increases risk
Periodontal therapy may improve diabetic control
Requires medical collaboration
Other Factors
Genetics
Gender
Race
Comprehensive Treatment Strategies
Patient education and motivation
Oral hygiene instruction
Antiseptics (rinses, toothpaste, irrigation)
Scaling and root planing (SRP)
Local or systemic antimicrobial therapy
Host modulation therapy (HMT)
Risk factor modification
Periodontal surgery (± HMT)
Sub-Antimicrobial-Dose Doxycycline (SDD)
Only FDA-approved systemic HMT for periodontitis
Used with scaling and root planing (SRP)
Not used alone (no monotherapy)
Previously called low-dose doxycycline (LDD)
Marketed as Periostat
Belongs to the tetracycline family
Tetracyclines
major impact in periodontal treatment
Used:
With SRP (nonsurgical therapy)
With surgical procedures (resective & regenerative)
Can be:
Local or systemic antimicrobials
Systemic host modulation agents (SDD)
Used for:
Chronic periodontitis
Aggressive periodontitis
Also used in systemic conditions:
Diabetes
Rosacea (e.g., Oracea)
Benefits:
Improved periodontal health
Better glycemic control (↓ glycated hemoglobin)
Enhance:
Reattachment
New attachment formation
Bone formation
Matrix Metalloproteinase (MMP) Inhibition
moa of SDD
Downregulates MMPs (collagen-degrading enzymes)
MMPs:
Produced by fibroblasts, keratinocytes, macrophages, PMNs, endothelial cells
Break down extracellular matrix (especially collagen)
Disease Association
MMP levels:
Increase with disease severity
Decrease after treatment
Excess MMPs → connective tissue breakdown → clinical signs of periodontitis
Key MMPs in Periodontitis
MMP-8
MMP-9
Derived mainly from PMNs
Degrade type I collagen (major component of gingiva & periodontal ligament)
Additional Actions of SDD
Reduces cytokine levels
Stimulates osteoblast activity
Promotes new bone formation
Increases collagen production
Tetracyclines as Host Modulation Agents
Effective due to pleiotropic effects (act on multiple host response components)
Only MMP inhibitors approved for periodontal treatment
Doxycycline:
More effective than tetracycline and minocycline
Preferred due to:
Safety
Good absorption
Favorable pharmacokinetics
Development of SDD
Created to reduce:
Side effects of long-term tetracycline use
Risk of antibiotic resistance
Dose:
20 mg (vs. 50–100 mg antimicrobial doses)
Microbial Safety
No changes in:
Oral flora composition
Bacterial resistance levels
Fecal or vaginal microflora
No overgrowth of opportunistic pathogens (e.g., Candida)
Short-Term Use Effects on MMPs and Collagenase
2-week regimen:
Reduced collagenase in GCF and gingival tissues
1-Month Use Effects on MMPs and Collagenase
Reduced collagenase levels
Rebound effect after stopping (returns to baseline)
3-Month Use Effects on MMPs and Collagenase
Sustained reduction in collagenase
No rebound after stopping
Greater reduction vs. placebo:
SDD: ~47.3%
Placebo: ~29.1%
Associated with:
Gains in clinical attachment
Clinical Trial Findings (3, 6, 9 months)
Reduced:
Probing depth
Collagenase activity
Increased:
Clinical attachment levels
Protected:
α1-antitrypsin (protective mediator)
Biochemical Effects
Decreased:
Bone collagen breakdown products (ICTP)
MMP-8 and MMP-13 levels