PS3120: Evidence-Based Health Psychology
1/93
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
94 Terms
What is health psychology?
A critical reflection about what it means to put people and their context at the centre of health research and practice.
What is the biomedical model?
Led understanding of health historically. Assumes any health issue can be explained by what happens in the body biologically and chemically.
What is the biomedical model based on?
Empiricism, needs evidence to exist. Heavy use of scientific method. Still guides us today.
What are the benefits of the biomedical model?
Increases life expectancy, quality of life for chronic patients and advances in medical technology - much more understanding of how body works.
What are the problems with the biomedical model?
Not all conditions can be cured - only focuses on absence of health, curing, not health itself and how to manage wellbeing. Reductionist, does not consider anything outside body. Disease (not health) oriented. Patriarchal and capitalist - power imbalances with clinicians and patients.
What causes illness according to the biomedical model?
Diseases come from outside the body and invade it or originate as internal involuntary physical changes
Who is response for illness according to the biomedical model?
Not individuals themselves.
How should illness be treated according to the biomedical model?
Medical treatments e.g. vaccination, surgery, chemotherapy
What is responsible for treatment according to the biomedical model?
The medical profession
What is the relationship between health and illness according to the biomedical model?
Seen as qualitatively different, no continuum between the two.
What is the role of psychology in illness according to the biomedical model?
Illnesses may have psychological consequences, but not causes.
What is the biomedical model not successful in, despite helping cure disease and allowing people to live longer?
Chronic diseases. People live longer, therefore develop chronic diseases which cannot be cured but need to be managed.
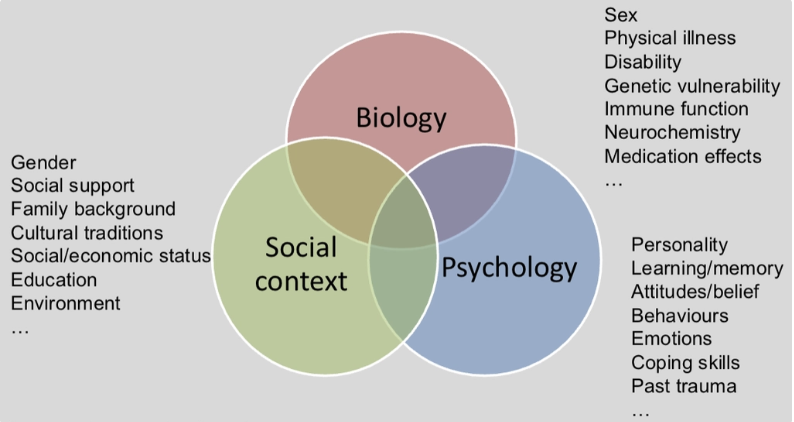
What is the biopsychosocial model? (Engel, 1977)
Health is not just caused by biology but an intersection of biology, psychology and social context.
Why is the biopsychosocial model just a guiding principle?
We do not have the tools to account for all the factors, not yet able to bring them altogether. Can focus in one aspect and also look at how it may interact with other things too however.
What causes illness according to the biopsychosocial model?
A combination of biological, psychological and social factors.
Who is responsible for illness according to the biopsychosocial model?
Individual behaviours is seen as one of many causes
How should illness be treated according to the biopsychosocial model?
Modifying the person as a whole, via many different means to address multi causality
Who is responsible for treatment according to the biopsychosocial model?
Multiple professions
What is the relationship between health and illness according to the biopsychosocial model?
A continuum
What is the role of psychology in the biopsychosocial model?
Illness may have psychological causes and consequences
What is the WHO’s definition of health? (1948)
A state of complete physical, mental and social wellbeing and not merely the absence of disease or infirmity.
What is health psychology? (Matarazzo, 1980)
The aggregation of educational/scientific/professional contributions of psychology to the promotion and maintenance of health, prevention and treatment of illness, identification of etiological and diagnostic correlates of health, illness and related dysfunctions, and the improvement of the healthcare system and health policy formation.
What is evidence-based practice (EBP) according to Sackett et al. (1996)?
Conscientious, explicit, judicious use of current best evidence in making decisions about the care of individual patients
What is evidence based practice (EBP) according to Straus et al. (2019)?
The integration of the best research evidence with our clinical expertise and our patient’s unique values and circumstances
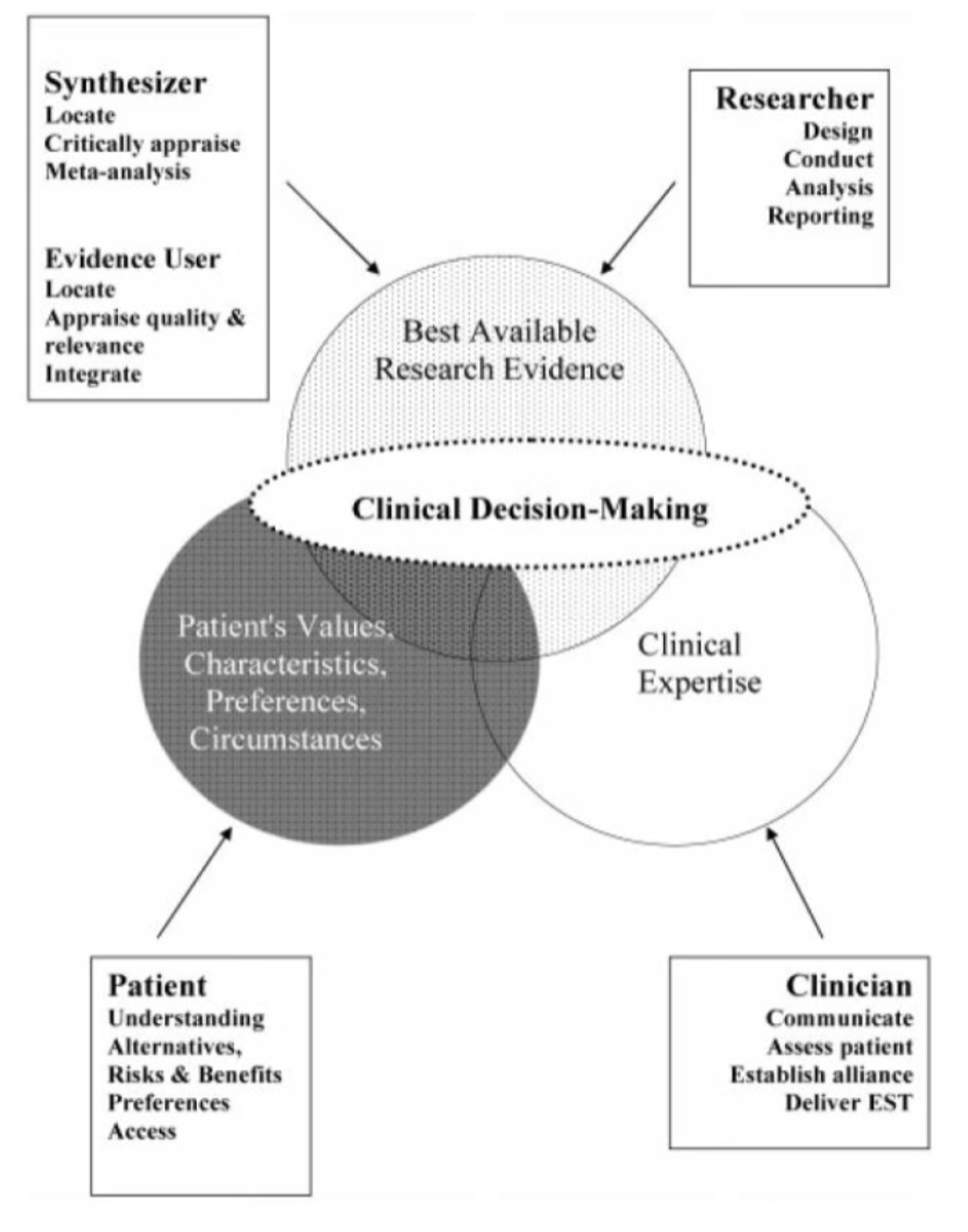
What is clinical decision making?
What is clinical expertise in clinical decision making model?
Ability to use clinical skills and past experience to rapidly identify a patient’s unique health state and diagnosis, their individual risks and benefits of potential interventions/exposures/diagnosis tests, or their personal values and expectations. (Straus et al., 2019)
Non-specific therapeutic factors, general professional role skill sets
What are patient’s values and preferences in the clinical decision making model?
Concerns and expectations that each patient brings to clinical encounters that must be integrated into shared clinical decisions if they are to serve the patient
What are patient’s circumstances in the clinical decision making model?
Patient’s clinical state and clinical setting where they are.
What is the overall reason for patient’s values, preferences, characteristics and circumstances in the clinical decision making model, and what is the problem with it?
Moving towards personalisation as all treatment is individualised, but be successful needs should be considered. Not very feasible currently as only have 15minute GP appointments, hard to gather this information in that time.
What is the role of best available research-evidence in the clinical decision making model?
Need to critically analyse research papers and apply this in practice, which takes time. Therefore there is an emphasis on evidence synthesis, where evidence is digested for practitioners in the form of systematic reviews and meta-analyses.
Helps practitioners apply an evidence based approach to healthcare.
What basic assumptions should be made about the quality of evidence in healthcare decisions?
The treatment needs to cause a change in patients - focus on RCTs. Qualitative studies are more low quality, but it takes account for the patient’s role as well.
Researchers no longer focus on just RCTs but embedding other evidence to have greater insight into why treatments may or may not work.
Why are qualitative studies important in EBHP despite being low quality evidence?
Involves patient’s role in management of health, allows co production of research and healthcare.
What is the NICE guidelines?
National Institute for Health and Care Excellence
What are the issues with the NICE guidelines currently?
Small proportion of guidelines consider sex and ethnicity. Less individualised treatments.
Why does evidence based practice matter?
Quality, accountability, healthcare management, policy influence, growth of evidence base, common language for transdisciplinary collaboration, production of meta-synthesis, tool for lifelong learning.
How does the clinical decision making model benefit evidence based practice?
Justifies emphasis put on evidence. Should improve results of decisions - is how clinical practice improves overtime. But all factors involved play a role. But synthesising evidence is one of the most important.
What were Rousseay and Gunia (2016)’s critiques of evidence based practice?
Ecological validity of RCTs is poor due to rigour to allow causality to be inferred. Study design does not match reality of healthcare of which is a chaotic landscape. However there is evolution to ensure ecological validity of accounted for. Need a strong evidence base for communities to be served well.
What is the response to the critique that EBP is a one-size-fits-all approach to practice decisions?
It involves substantial adaptation of evidence to fit with local conditions and practitioner judgements.
What is the response to the critique that EBP stifles innovation?
It helps diffuse new practices that may otherwise have spread more slowly. Has lead to new forms of research to provide more useable evidence to practitioners.
What is the response to the critique that EBP relies solely or primarily on RCTs?
Reviews and evidence synthesis incorporate the diverse array of studies relevant to practice questions.
What is the response to the critique that EBP relies heavily on human judgement, which may create biases or conflicts of interest?
Integrates quality control procedures, such as transparency in reporting or disclosure requirements.
What is the response to the critique that EP guidelines can undermine EBP, if based on low quality evidence and not subjected to regular updates etc?
Transparency in methods. Use of qualifiers in recommendations e.g. could be useful, strongly recommended.
What NICE guidelines were heavily criticised due to a weak evidence base?
Myalgic encephalomyelitis (ME)
What were clinical psychologist students’ perceptions of EBP?
Found those with any contact with EBP were more likely to believe it should integrated in training, classes and work. Were more likely to agree with underlying practices. More likely to endorse something you have experience with.
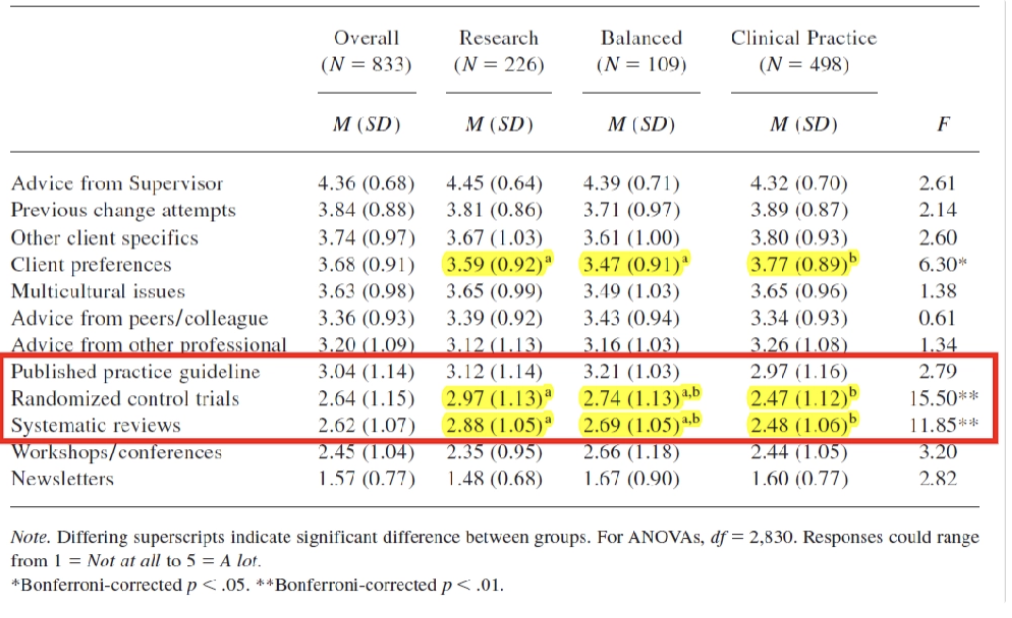
What was found regarding how psychology students make decisions and what they rely on for it?
EBP was very low and limited.
What is the Scientist-Practitioner model?
Training of psychologists must put equal emphasis on research and practice. Must be able to apply available scientific knowledge and inquiry into practice.
Why was the Scientist-Practitioner model implemented?
Reviewed training of clinical psychologists, found they were not evidence based enough. When put in place in 1949, all clinical psychologists had to learn as much about research and evidence, as much about its applications.
Need to work equally between research and practice.
What are the competences required of a scientist-practitioner?
Scientific view, methods, navigate evidence and access in effective ways but also understand the role and limits of clinical judgements and how to use evidence with a patient and their needs.
What is the role of best available research evidence in the scientist-practitioner model?
Scientific view of psychology. Knowledge of research design and methods. Strategies for accessing best available research. Ability to critically appraise evidence.
What is the role of clinical expertise in the scientist-practitioner model?
Understand role and limits of clinical judgement. Skills in relationship building. Assessment and diagnosis skills. Skills to implement empirically supported treatments. Integration of empirically supported treatments with client characteristics.
What is the role of patient values and needs in the scientist-practitioner model?
Healthcare delivery is a collaborative endeavour. Need knowledge of diverse groups. Ability to ascertain patient values and preferences. Respond effectively to patient preferences and values.
What critiques are there of the scientist-practitioner model?
Difficulties in translating medical model. Unclear what is right balance between the 3 skill sets of the model. Not all therapists need to be SPs, especially if applying well established treatments. Practical difficulties of implementing model - time sharing, access to resources and funding.
Inconsistencies in model - DSM-5 is medically oriented rather than individual based - how can this be done in partnership with the biopsychosocial perspective?
What are the 5 steps to EBP that must be followed to provide best care?
Ask → Acquire → Appraise → Apply → Assess
What is the ‘Ask’ step in the 5 steps to EBP?
Make sure to ask patients all questions needed to ensure they are relevant to patient and can be converted into information and evidence to address patient problem.
Convert the need for information into an answerable question with evidence from clinical care research.
What is the ‘Acquire’ step in the 5 steps to EBP?
Search for evidence to answer the questions. Conclude what is answered and the certainty around that answer.
Track down best evidence with which to answer that question.
What is the ‘Appraise’ step of the 5 steps to EBP?
Critical appraisal of the evidence. Is it applicable, clinically significant etc.
What is the ‘Apply’ step of the 5 steps of EBP?
Can you apply the new knowledge from the evidence to develop a care plan for the patient
Integrate critical appraisal with clinical expertise and patient’s preferences.
What is the ‘Assess’ step of the 5 steps to EBP?
Evaluate the process. Make improvements, develop selves.
Evaluate your effectiveness and seek ways to improve your approach.
What are background questions for the ‘Ask’ step of the EBP steps?
Ask for general knowledge about a condition, test or treatment
Can be asked about any disorder/health state/test/treatment/intervention
Must include a root, verb and disorder etc.
What are examples of background questions in the 5 steps to EBP ‘Ask’?
What predicts harmful gambling relapse? How does stress affect failure to conceive?
What are foreground questions in the ‘Ask’ step for the 5 steps to EBP?
Asking for specific knowledge to inform clinical decisions or actions. If define foreground clearly, more likely to get right evidence faster, more accurate. Improves efficiency of step following and easier to critically appraise studies and apply.
How do you select relevant questions for the ‘Ask’ step of the 5 steps to EBP?
Which question is most important to wellbeing, relevant to knowledge needs, feasible to answer within time available, interesting to self or patient, likely to recur in practice.
Why bother formulating questions for the ‘Ask’ step of the 5 steps to EBP?
Helps efficiency, bring in clarity of what is important for patient, bring clarity to gaps in knowledge as professionals, tells you what useful answers should be looking for.
What is the best evidence to use for the ‘Acquire’ step of the 5 steps to EBP?
RCTs - only source of evidence that can say whether intervention works for specific conditions. Not always possible however, therefore observational sometimes has to be used.
What are some ways to develop an effective search strategy?
Structure into concepts according to PICO
Consider different terms for each concept
Consider limits (time, language, design)
Use Boolean operators (AND/OR/NOT)
Keep a search log
What is PICO?
Structured framework in healthcare to formulate specific, answerable questions and guide searches
Patient/population/problem → Intervention → Comparison → Outcome
General searches lead to…
more results, lower relevance
Specific searches lead to…
fewer results, higher relevance
What should be looked at specifically in the ‘Appraise’ step for the 5 steps to EBP?
Validity/impact/importance/applicability. Can you trust results, design, execution. Rates of adherence, biases, how this shaped results. Effect sizes. Risk reduction. Confidence intervals. Generalisability.
What is a CASP checklist for systematic reviews?
Tools to critically evaluate quality, results and relevance of research evidence. Each designed for each type of study, what questions should be asked about certain studies.
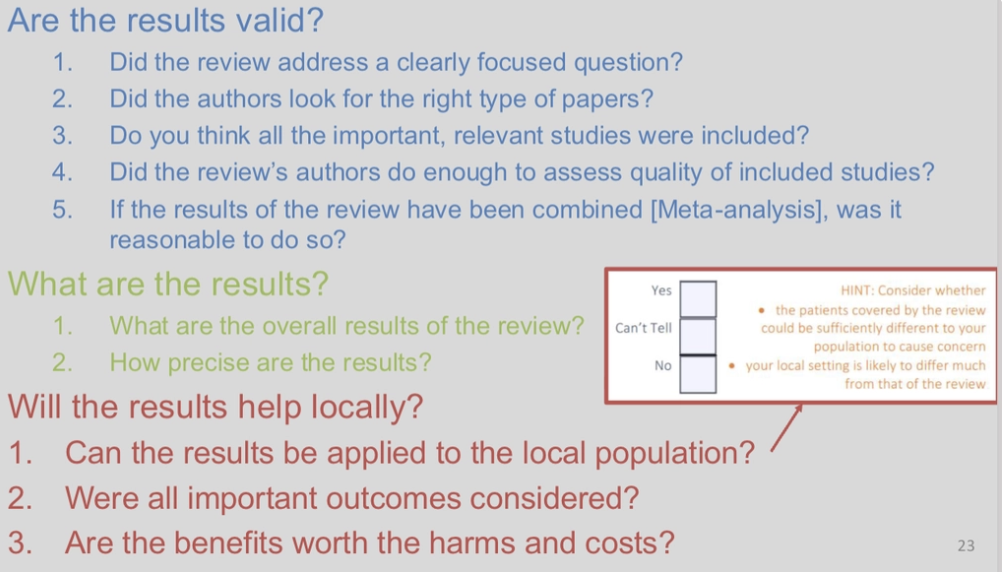
What do you want to be sure of by the end of step 3 ‘Appraise’ in the 5 steps to EBP?
A comprehensive literature search was conducted, and the quality of studies/reports were evaluated.
What are health interventions?
Treatments. therapies, procedures or actions implemented by healthcare professionals to/with/on behalf of patients, in response to a health problem, to improve their condition and achieve beneficial outcomes.
Interventions can be…
Simple, small or large, complex, multidisciplinary
What are the elements and domains of interventions?
Goals, specific elements, non specific elements, node of delivery, dose, interventionists, protocol, individual patient care, organisational/service modification, health professional, population level.
Why are the elements and domains of interventions important?
The more clarity of these elements allows better theorisation and implementation of the intervention.
What are goals for interventions?
Overall aim, what it sets to achieve, outcomes to change and for who, outcomes need to be directly linked to problem identified.
What are specific elements for interventions?
Active components of change e.g. active ingredients in pills directly changing something in body. Want to test that it will cause change.
What are non-specific elements for interventions?
Things surrounding the specific elements e.g. UI on an app, amount of people in a focus group.
What is the dose for interventions?
Frequency of intervention e.g. how many times a day they practice mindfulness
What are interventionists for interventions?
Is there one or is it self administered, are there multiple?
What is the population level domain of interventions?
Policies, only work if vast majority of population partakes such as COVID 19 vaccine delivery
What does intervention research aim to do?
Generate evidence that supports the appropriateness, safety and effectiveness of interventions in producing beneficial outcomes.
What is intervention research evidence used for?
Develop guidelines that inform practice, help direct decision-making about patient care.
What are 2 important things to consider with intervention research/
Causality, and that patients actually want to partake in the intervention.
What are the 5 stages of intervention development?
Theory → Modelling → Exploratory Trial → Definitive RCT → Long Term Implementation
What is a theory in intervention development?
To reach an in depth understanding of the health problem - how it manifests, why and who is vulnerable.
What is modelling in intervention development?
To select the most appropriate strategies to address each aspect of the health problem e.g. nature, dose and mode of delivery.
What is the preclinical phase - theory - of intervention development?
Exploring relevant theory to ensure best choice of intervention and hypothesis and to predict major confounders and strategic design issues.
What theory best explains problem, which theory should inform intervention and whether theory is valid.
What is phase 1 - modelling - of intervention development?
Identify the components of intervention and the underlying mechanisms by which they will influence outcomes to provide guidance you can predict and how they relate to and interact with each other.
Whether activities designed in line with theory, and if they trigger mechanisms for change.