Looks like no one added any tags here yet for you.
Define CAP, HAP, and VAP
Community acquired pneumonia (CAP): Pneumonia acquired outside of the hospital setting
Hospital acquired pneumonia (HAP): Pneumonia occurring ≥48 hours after admission
Ventilator-acquired pneumonia (VAP): Pneumonia arising >48-72 hours after endotracheal intubation
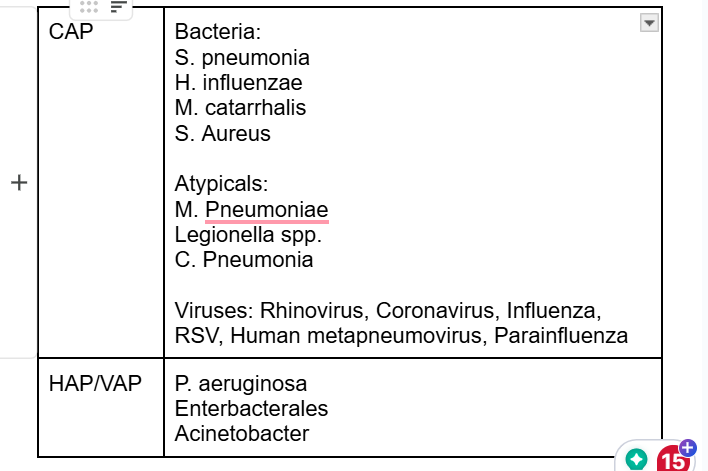
What are the most common pathogens causing CAP? What about HAP/VAP?
Why don’t we get sputum cultures on all pneumonia patients?
Difficult to obtain, and difficult to interpert (often contaminated)
Can we use sputum gram stains to modify therapy?
for VAP
How should MRSA nares be utilized?
used to RULE OUT MRSA
if a patient doesn't require MRSA therapy, DONT order the lab- dont use MRSA test to add MRSA coverage
How should Procalcitonin be utilized?
Inflammatory marker specfic to bacterial infections- often used to rule out bacterial source of infection
Know how to use the CURB-65 score to determine where a patient with CAP should be treated
Scoring Criteria (1 point for each factor):
Confusion (disorientation to person, place, or time)
Uremia (>20 mg/dL)
Respiratory rate (>30 breaths per minute)
Blood pressure (SBP <90 mmHg or DBP <60 mmHg)
Age ≥ 65 years
Interpreting the Score and Treatment Recommendations:
CURB-65 Score | Risk of Mortality | Recommended Site of Care |
|---|---|---|
0-1 | Low | Outpatient (home treatment) |
2 | Intermediate | Supervised treatment or hospitalization (consider admission based on clinical judgment) |
≥3 | High | Inpatient hospitalization (ICU may be needed for severe cases) |
When does a CAP patient require ICU admission?
Major Criteria (Only one needed for ICU admission):
Hypotension requiring vasopressors
Respiratory failure requiring mechanical ventilation
Minor Criteria (Need at least three for ICU admission):
Respiratory rate ≥30 breaths/min
PaO₂/FiO₂ ratio ≤250 (indicating poor oxygenation)
Multilobar infiltrates on imaging
Confusion or disorientation (to person, place, or time)
Uremia (BUN ≥20 mg/dL)
Leukopenia (WBC <4,000 cells/mm³)
Thrombocytopenia (platelet count <100,000 cells/mm³)
Hypothermia (core temperature <36°C)
Hypotension requiring aggressive fluid resuscitation
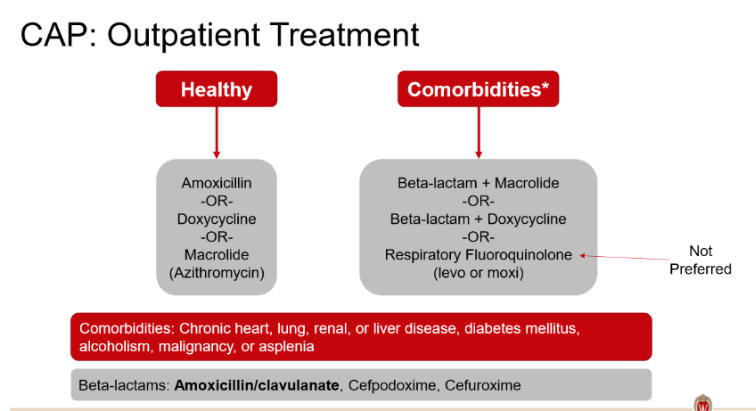
What antibiotics can be used to treat a patient with CAP who is being managed in the outpatient setting? How does this change if they have comorbidities?
*amox doesnt cover atypicals but its ok cuz it proven to work
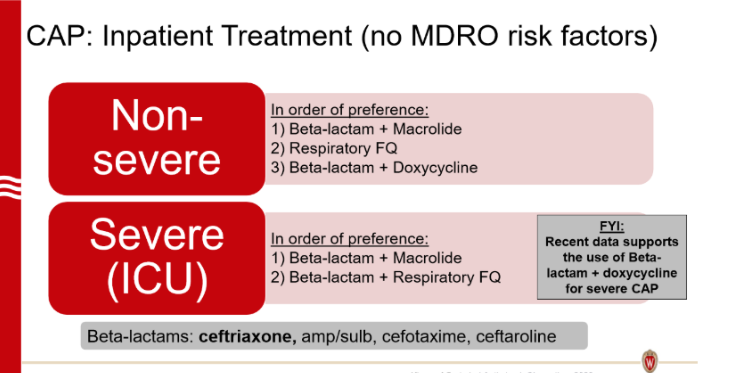
What antibiotics can be used to treat a patient with CAP who is being admitted to the hospital? What about if they are in the ICU?
Which patients require empiric MRSA coverage for CAP? What antibiotics do you use to cover MRSA?
History of MRSA cultured in last year—> add coverage to all inpatients
Hospitilization with IV antibiotics given in last 90 days—> add coverage only if pt is in ICU
Add vanco or linezolid
Which patients require empiric pseudomonas coverage for CAP? What antibiotics do you use to cover pseudomonas?
History of pseudomonas cultured in last year—> add coverage to all inpatients
Hospitalization with IV antibiotics given in last 90 days—> add coverage only if pt is in ICU
Replace beta-lactam with: Pip/tazo, cefepime, ceftazidime, aztreonam, meropenem, imipenem
How long should patients with CAP be treated? Why might a patient require longer treatment?
Minimum duration: 5 days
To stop antibiotics after 5 days, the patient must:
Be afebrile for 48-72 hours
Have ≤1 sign of clinical instability
*CAP due to MRSA or Pseudomonas is 7 days tx
Criteria for Clinical Stability:
✔Temperature ≤ 37.8°C
✔ Heart rate ≤ 100 beats/min
✔ Respiratory rate ≤ 24 breaths/min
✔ Systolic blood pressure ≥ 90 mmHg
✔ Arterial oxygen saturation ≥ 90% or PaO₂ ≥ 60 mmHg on room air
✔ Ability to maintain oral intake
✔ Normal mental status