ANHB2212 - Respiratory System Development
1/125
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
126 Terms
When does the larynx, trachea and lungs arise and from what?
week 4 from an outgrowth of foregut
What does endoderm give rise to in the respiratory system?
mucosal lining of larynx, trachea and bronchi
epithelial cells of alveoli (simple squamous)
What does mesoderm give rise to in the respiratory system?
• smooth muscle and cartilage supporting larynx, trachea & bronchi (lateral plate mesoderm)
• visceral pleura covering the lung (splanchnic mesoderm)
• parietal pleura covering the thoracic cavity: costal, mediastinal & diaphragmatic regions (somatic mesoderm)
• Vasculature
When does development of the respiratory system begin?
day 22
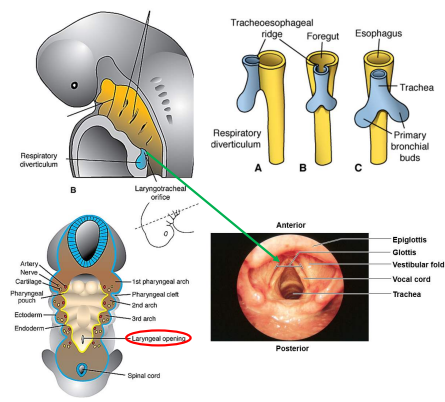
Describe the development of the primary bronchi, trachea and esophagus.
respiratory diverticulum (RD) forms as a ventral outpouching of the endodermal foregut
RD grows ventro-caudally through the splanchnic mesenchyme surrounding the foregut
RD splits into right and left primary bronchi in a process called bifurcation at days 26-28
proximal end of RD forms trachea and larynx
larynx opens into pharynx via glottis
as primary bronchi form, the stem of the RD separates from the overlying portion of pharynx to become the esophagus
When does first bifurcation occur?
day 26-28
What is the original point of evagination of the diverticulum?
glottis
What is the pattern of branching of the lung endoderm regulated by?
signaling from the surrounding splanchnic mesenchyme
What are the muscles of the larynx innervated by?
vagus nerve
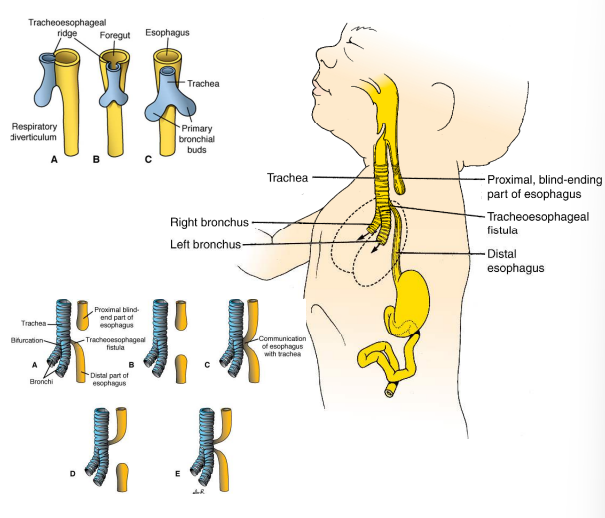
What happens when the foregut fails to separate into the trachea and esophagus 1) from birth 2) before birth?
fluid (milk) can enter lungs = infection and death
blind-ending esophagus prevents swallowing amniotic fluid which is usually returned to the mother via placenta circulation = excess amniotic fluid and distention of the uterus
Summarise the anatomy of the lung tubes (bronchi and bronchioles)
primary bronchi enter lungs at hilum
lobar bronchi enter at lobes
tertiary bronchi enter at bronchopulmonary segments
bronchioles
terminal bronchioles
respiratory bronchioles
alveolar ducts
alveoli
Describe branching of the bronchi.
Late week 4 - two primary bronchi
Early week 5 - secondary bronchi (3 right, 2 left)
Late week 5 - tertiary bronchi (10 right, 8 left) in bronchopulmonary segments, lungs assume a more caudal position
Week 5 to 24 - terminal bronchioles give rise to respiratory bronchioles that give rise to 3-6 alveolar ducts that end in primitive alveoli. Respiratory membrane starts to form as type 1 alveolar cells and capillaries become closer together and type 1 cells become thinner.
Week 24 - type 2 alveolar cells develop to produce surfactant
At the end of the 6th gestational month how many generations of subdivisions have occurred?
17 generations (postnatally 6 more occur)
Surfactant
A substance produced by type 2 alveolar cells that prevent alveolar collapsing during respiration.
When do fetal breathing movements occur?
weeks 10-12
Why do fetal breathing movements occur?
stimulate lung development
condition respiratory muscles
What happens at birth regarding amniotic fluid and surfactant?
amniotic fluid is absorbed whilst surfactant is not.
Pleura
A single layer of squamous cells (mesothelium) that lines the pleural cavity that is subdivided into visceral (covers lungs) and parietal pleura (covers thoracic cavity).
What is pleural (parietal and visceral) developed from?
parietal - somatic lateral plate mesoderm
visceral = splanchnic lateral plate mesoderm
Where is pleural fluid produced?
Mesothelium
What is the purpose of pleural fluid?
• allows for parietal and visceral pleura to slide over each other when the thoracic wall moves (reduces friction)
• combination of parietal pleura, visceral pleura & pleural fluid keep the lungs attached to the costal, diaphragmatic & mediastinal surfaces of the thoracic cavity
• when thorax moves lungs volume changes because visceral pleura is “stuck” to thoracic cavity surfaces via parietal pleura
What are the 3 types of parietal pleura?
costal
mediastinal
diaphragmatic
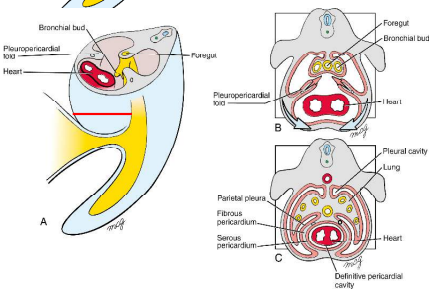
Describe the development of the pleural and pericardial cavities
pericardio-peritoneal canals become too small as lung buds expand caudolaterally within them, causing lungs to expand dorsally, laterally and ventrally into body wall mesenchyme
in early week 5, 2 pleuro-pericardial folds develop from the lateral body walls and project into the undivided thoracic cavity
these folds grow medially towards each other between the heart and lungs, eventually fusing at the end of week 5 with the foregut mesenchyme
the primitive pericardial cavity is divided into 2 dorsolateral pleural cavities and 1 ventral definitive pericardial cavity
What are the pleural and pericardial cavities lined by?
mesothelium
What is the function of the fluid secreted by mesothelium?
reduce friction during movement
pleural fluid keeps lungs stuck to thoracic surfaces
Where do phrenic nerves arise from?
joined branches of cervical roots 3, 4, and 5
Describe the innervation of the diaphragm.
Phrenic nerves follow the diaphragm as it descends into the lower thoracic vertebrae through the fibrous pericardium.
Describe the motor and sensory innervation of phrenic nerves.
motor = diaphragm muscles
sensory = fibrous & parietal serous pericardium, mediastinal & diaphragmatic pleura, peritoneum covering inferior surface of diaphragm
What organisms have a diaphragm?
mammals only
What are the 2 functions of the diaphragm?
drive inspiration
barrier between thorax and abdomen
What 3 major tubes pass between thorax and abdomen and how?
• Inferior vena cava (IVC) - through the central tendon (T8)
• Esophagus – through diaphragm muscle (T10)
• Aorta – behind the crura (muscle) (T12)
What happens to the inferior vena cava, esophagus and aorta when the diaphragm contracts?
inferior vena cava - Venous return to heart via IVC increases due to increased abdominal pressure & decreased thoracic pressure
esophagus - Muscle surrounding the esophagus reinforces the cardiac sphincter of the stomach
aorta - unaffected because it passes behind the crura
What 4 regions of the intraembryonic coelom does the septum transversum create?
• Large pericardial cavity
• Large peritoneal cavity
• 2 x Pericardio-peritoneal canals
Pericardio-peritoneal canals
short channels located dorsal to the ST & lateral to the proximal part of future esophagus
spaces into which lungs first start to grow
pleuro-peritoneal folds
2 x pyramidal shaped structures between thoracic & abdominal cavities
Originate in the cervical region
Describe the development of the diaphragm.
pleuro-peritoneal folds (PPFs) expand dorsally and ventrally across the septum transversum.
PPFs give rise to diaphragm muscle connective tissue.
first muscle progenitors emigrate from cervical somites (C3-5) to PPFs. Axons of the phrenic nerve follow the developing muscle and project into PPFs.
Once the muscle progenitors are encased by PPF connective tissue, the PPFs, diaphragm muscle, developing heart, lungs & liver start to descend from cervical levels to final location in thorax.
some muscle develops in the central tendon but this muscle fails at it matures due to lack of innervation
What regulates diaphragm muscle development?
Pleuro-peritoneal folds
True Ribs
Ribs 1-7
Directly connected to the sternum by costal cartilage
False Ribs
Ribs 8-10
do not articulate directly with the sternum but are connected to it via fusing with the costal cartilages of the rib above to rib 7
Floating Ribs
ribs 11-12
no connection to the sternum
What are the symphyses of the thoracic cavity?
intervertebral discs
manubriosternal joint
What are the synchondroses of the thoracic cavity?
costochondral junction (where the ribs meet hyaline cartilage)
sternocostal junction of rib 1
xiphisternal joint
What are the synovial joints of the thoracic cavity?
costovertebral
costotransverse
sternocostal junctions of ribs 2-7
interchondral joints of ribs 7-10
Describe the vertebral body facets of the thoracic vertebrae
T2-9 = demi-facets
T1, T10-12 = full facets
Describe the transverse process facets of the thoracic vertebrae.
T1-7 = rounded facet
T8-10 = flat facet
T11-T12 = no facet
Describe the zygapophyseal joint facet orientation of the thoracic vertebrae.
T1-T11 = typical orientation
T12 = superior and inferior facets have different orientation
Describe the head of each rib.
R2-9 = 2 articular facets
R1, R10-R12 = 1 articular facet
Describe the tubercle, neck and angle of the ribs.
R1-10 = present
R11, R12 = absent
External intercostal muscles
from tubercles of the ribs to costal cartilages
most active in inspiration
oriented distally towards the sternum (\)
external intercostal membrane present (thin layer of connective tissue)
Internal Intercostal Muscles
from parasternal regions to angles of ribs
oriented opposite to the external intercostal muscles
most active in expiration
Innermost Intercostal Muscles
same orientation as internal intercostals (opposite external)
most obvious in lateral thoracic wall
What are the 3 types of chest wall movements?
bucket handle
pump-handle
calliper
Bucket Handle Movement
True ribs (1-7) elevate, swinging laterally.
Pump Handle Movement
- rib 1 lifts manubrium & carries sternum forwards
- manubriosternal joint ‘bends’ (symphysis) reducing the sternal angle
- rib 1 moves sternum, therefore, all true and false ribs move = movement of sternocostal joints 2-7 and costovertebral & costotransverse joints
Calliper Movement
- False ribs (8-10) act on the costal margin, not sternum
- The lower thorax widens laterally to become ‘broader
What are the functions of the floating ribs?
Support diaphragm & spread (‘lengthen’) thorax (supero-inferiorly)
Torque
force applied over a distance (lever arm = rib) causing rotation about a fulcrum (axis of rotation = spine)
= force x distance from axis
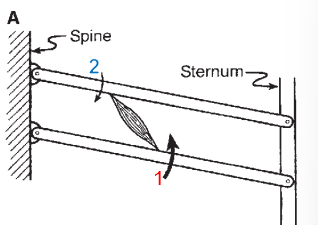
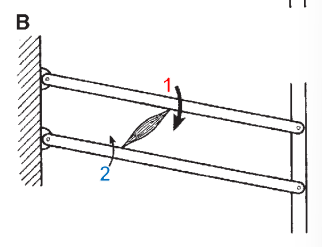
Describe what happens in this scenario regarding movement. What is this modelling?
External intercostals:
• muscle insertion point 1 is further away from the axis compared insertion point 2
• assuming equal amount of force, when the muscle contracts, torque is greater at insertion point 1 compared to point 2
• so movement will occur in an upwards and forward direction (rib elevation)
Describe what happens in this scenario regarding movement. What is this modelling?
Internal intercostals:
• muscle insertion point 1 is further away from the axis compared insertion point 2
• assuming equal amount of force, when the muscle contracts torque is greater at insertion point 1 compared to point 2
• so movement will occur in a downwards direction (rib depression)
Describe pleural pressure
Having lungs stuck to the pleural cavity means they are very stretched at rest The resulting tension force means the lungs are always pulling on the body wall so pleural pressure is always negative
What are recesses between visceral and parietal pleura? What are the 3 types?
spaces where lungs or pleural fluid can move to or accumulate that are important for accommodating changes in lung volume during breathing.
costomediastinal
costovertebral
costodiaphragmatic
Costamediastinal Recess
Pleural fluid recess either side of the sternum, between body wall and pericardium
Costovertebral Recess
Pleural fluid recess that extends to rib 12 where the lungs do not
Costodiaphragmatic Process
Pleural fluid process between the inferior margin of the lungs and inferior margin of the pleural cavities. At the mid axillary line lungs extend to rib 8 and pleura extends to rib 10. Safe place to take pleural fluid sample.
What is the largest pleural recess?
costodiaphragmatic recesses
Describe the sloping of ribs in adults and how it impacts intrathoracic volume.
In adults at rest, ribs slope downward ventrally Elevation of ribs, therefore, increases intrathoracic volume
Describe the sloping of ribs in newborns and how it impacts intrathoracic volume.
In newborns, ribs are oriented more horizontally As the ribs are already elevated, further elevation has little impact on intrathoracic volume.
Compare the adult and newborn diaphragm.
the newborn is very reliant on the diaphragm during ventilation BUT the neonatal diaphragm is much flatter compared to the adult. This results in a proportionally smaller range of displacement of air when the diaphragm moves
Why do babies breathe rapidly?
the neonatal diaphragm is much flatter compared to the adult This results in a proportionally smaller range of displacement of air when the diaphragm moves
What 2 arteries do the lungs receive blood from?
bronchial arteries
pulmonary arteries
Bronchial arteries
bronchial arteries (2%): responsible for lung physiology: supply bronchi, bronchioles, CT, visceral pleura & the larger pulmonary BVs
Pulmonary arteries
pulmonary arteries (98%): whole body physiology & supply alveoli
Describe the breasts
Breasts are modified sweat glands
They consist of mammary glands, superficial fascia, and overlying skin
The breast is related to the thoracic wall and associated upper limb structures - therefore, vascular supply and drainage can occur by multiple routes
How are the breasts (and nipple) innervated?
Anterior and lateral cutaneous branches of the 2nd to 6th intercostal nerves
Nipple is innervated by the fourth intercostal nerve
Sternal Foramen
An anatomical variant of the sternum that occurs due to incomplete fusion of the sternal ossification centre.
What ligaments hold the rib to the vertebrae?
radiate ligament of head of rib (to body)
superior costotransverse ligament (to transverse process)
Describe the attachment of the diaphragm
the back of the sternum, along the costal arch to the tip of the 12th rib then arise on each side of L2 from lumbar fascia.
Where is the breast located?
Above the level of the 2nd rib to the 6th rib. It extends from the edge of the sternum to midaxillary line.
Axillary Tail
The prolongation of the breast from the midaxillary line posteriorly.
What structures are associated with the costal groove
Intercostal vein, artery & nerve.
What bones form the boundary of the thoracic inlet?
T1 vertebrae, manubrium, first rib
What bones form the boundary of the thoracic outlet?
T12 vertebrae, tip of rib 12, tip of rib 11, costal margin (ribs 7-10ish),
xiphoid process of sternum
What structure closes off the thoracic outlet?
diaphragm
The costal cartilage of which rib articulates with the manubriosternal joint?
rib 2
Describe the contribution of upper ribs to the mechanism by which the volume of the thoracic cavity is increased during filling of the lungs
Bucket handle pivots ribs up, overall thoracic circumference increases
Describe the contribution of lower ribs to the mechanism by which the volume of the thoracic cavity is increased during filling of the lungs
Calliper action widens the transverse dimension of lower thorax
Describe the contribution of the manubrium to the mechanism by which the volume of the thoracic cavity is increased during filling of the lungs
No angle change with rib 1, but the angle with sternal body increases
on the anterior / ventral body surface due to movement of rib 1.
Describe the contribution of the sternal body to the mechanism by which the volume of the thoracic cavity is increased during filling of the lungs
Angle of the manubriosternal joint changes as described above, body
of sternum moves out and up to increase antero-posterior thoracic
diameter.
where do the crura attach to the vertebral column?
left = L1-2
right = L1-2
Why is it advantageous for the diaphragm to pierce the muscle of the diaphragm?
If the oesophagus was not surrounded by muscle, food would be forced up from
the stomach because each contraction of the diaphragm increases abdominal
pressure. The oesophagus being surrounded by muscle prevents this reflux
What embryological structure develops into the central tendon?
The region of the pleuro-peritoneal folds where muscle cells fail to develop
Explain the reason for the difference in sound above and below the right dome of the diaphragm.
Below the line, the solid liver in the abdomen deadens percussion, causing a muffled sound.
Above the line, the thorax sounds hollow because of the air spaces in the lung.
Which layers of the intercostal muscles do the neurovascular bundles run between?
Internal and Innermost intercostals
Function of the scales during breathing
active during breathing to attach to ribs 1 and 2 to elevate the ribcage.
Function of the sternocleidomastoid during breathing
active during deep\laboured breathing to elevate the sternum
Function of the serratus posterior superior during breathing
active during deep/laboured breathing to elevate ribs 2-5
Function of the serratus posterior inferior and quadratus lumborum during breathing
active during deep/laboured breathing to depress the lower ribs
obstructive respiration
Obstructive respiration occurs during lung disorders such as Chronic Obstructive
Pulmonary Disease (COPD), which is a group of lung diseases that impede normal airflow.
Function of the rectus abdominus and oblique abdominus during breathing.
active in forced exhalation to pushes the abdominal contents up against the diaphragm to decrease thoracic volume
Function of the pectoralis major during breathing
used during obstructive respiration: If the arms are fixed, e.g. by holding on
to a chair, pectoralis major expands the ribcage anteriorly