Looks like no one added any tags here yet for you.
The postoperative period begins
immediately after surgery and continues until the patient is discharged from medical care or until the patient experiences complete recovery.
After surgery, the primary focus is on
protecting the patient, who has been put in physiological risk during surgery, and preventing complications while the body heals.
Phase I
• Care during the immediate postanaesthesia period
• Focused on the patient’s basic life-sustaining needs
• Constant, vigilant monitoring
Goal: Prepare patient for safe transfer to phase II or inpatient unit
Phase II
• Surgery patient is ambulatory
Goal: Prepare patient for transfer to extended-care environment or home with discharge teaching
Extended Observation
• Ongoing care for patients who will be admitted to the unit and those who require observation or interventions
Goal: Prepare patient for self-care
Airway
• Patency
• Oral or nasal airway
• Laryngeal mask airway
• Endotracheal tube with ventilator settings
Breathing
• Respiratory rate and quality
• Auscultated breath sounds
• Pulse oximetry
• Capnography or other technology-supported monitoring if indicated
• Supplemental O2
Circulation
• ECG monitoring: rate and rhythm
• BP: noninvasive or arterial line
• Hemodynamic pressure readings (if applicable)
• Temperature
• Capillary refill
• Color, temperature, moisture of skin
• Apical and peripheral pulses
Neurological
• Level of consciousness
• Orientation
• Sensory and motor status
• Pupil size and reaction
Surgical Site
• Dressings and visible incisions
• Drains: type, patency, and drainage
• IV assessment: location and condition of sites, solutions infusing
Genitourinary
• Urine output
Gastrointestinal
• Nausea, vomiting
• Intake (fluids, irrigations)
• Output (vomitus)
• Bowel sounds
Pain
• Incision or other
Patient Safety Needs
• Patient position
• Fall risk assessment
Clinical Manifestations of Inadequate Oxygenation
Central Nervous System
• Restlessness
• Agitation
• Muscle twitching
• Seizures
• Coma
Cardiovascular System• Hypertension• Hypotension• Tachycardia• Bradycardia• Dysrhythmias
Integumentary System
• Cyanosis
• Prolonged capillary refill
• Flushed and moist skin
Respiratory System
• Alterations ranging from increased to absent respiratory effort
• Use of accessory muscles
• Abnormal breath sounds
• Abnormal arterial blood gases
Renal System
• Urine output 30 mL/hour
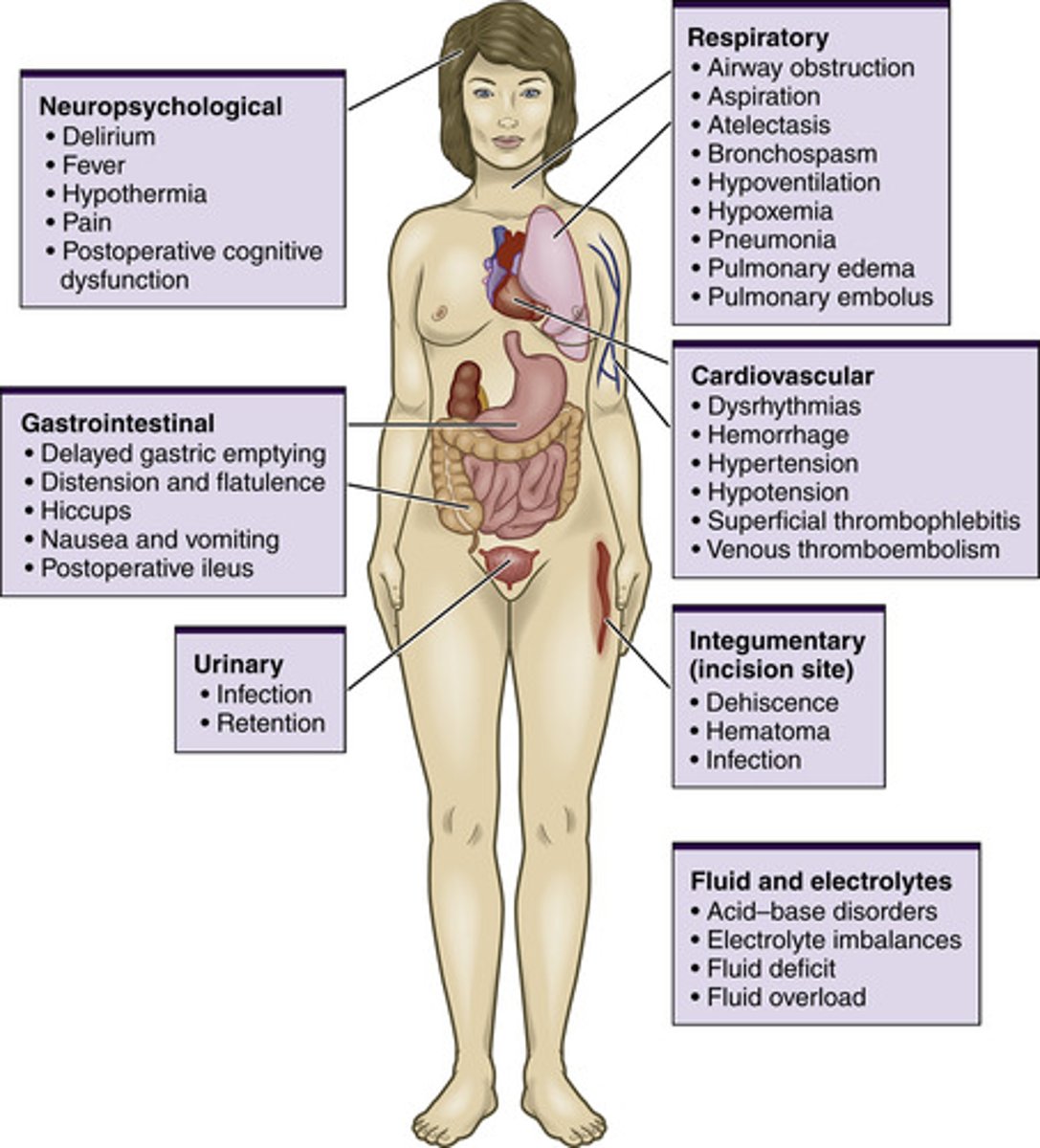
Post Op Complications
See image
Safety Alert
The unconscious patient can be placed in a lateral "recovery" position (see Figure 22.3) to keep the airway open and reduce the risk for aspiration if vomiting occurs, unless contraindicated related to the type of surgery (Rothrock, 2019).
The anaesthesiologist or surgeon should be notified if any of the following occur:
1. Systolic BP is less than 90 mm Hg or greater than 160 mm Hg.
2. Pulse rate is less than 60 beats per minute (bpm) or greater than 120 bpm.
3. Pulse pressure (difference between systolic and diastolic pressures) narrows.
4. BP gradually decreases during several consecutive readings.
5. An irregular cardiac rhythm develops.
6. There is a significant variation from preoperative readings.
Emergence delirium
Disorientation that occurs during anesthetic recovery as consciousness returns. May be characterized by vocalization, aggression, thrashing, and locomotor activity
. Contributing factors include the following:
• Hypoxia
• Anaesthetic agents
• Bladder distension
• Sensory and cognitive impairments
• Inadequate pain control
• Electrolyte abnormalities
• State of anxiety before surgery
Delayed Awakening
Longer than expected duration of postoperative unconsciousness usually caused by prolonged drug action and rarely, by neurological injury.
Significance Of Postoperative Temperature Changes
≤12 hours
Hypothermia to 35°C
Effects of anaesthesia
Body heat loss in surgical exposure
First 24-48 hours
Elevation to 38°C
Inflammatory response to surgical stress
>38°C
Lung congestion, atelectasis
Third day and later
Elevation above 37.7°C
Wound infection
Urinary infection
Respiratory infection
Phlebitis
Postoperative Diets
Clear Fluids
Broth, gelatin, water, tea, black coffee
Fluids
Milk, coffee with cream, cream soups
Soft Diet
Fish, cottage cheese, pasta, eggs, mousse, pudding
Full Diet
Regular diet
Patients can also be placed on special diets, such as diabetic or low sodium.
Postoperative ileus (POI) is a
delay in the return of the GI system's normal peristalsis, specifically after GI surgery. It is characterized by abdominal distension and tenderness or pain. Stomach motility returns in 1 to 2 days, and bowel motility in 3 to 5 days.
Abdominal distension during this time may require insertion of a nasogastric tube for symptomatic relief and the lowering of opioid doses or provision of pain relief with NSAIDs to reduce inflammation
Paralytic ileus is
impairment of intestinal motility (ileus that persists for more than 2 to 3 days) postoperatively. It can be associated with the large and small intestine and resolves with treatment; it is not a mechanical obstruction. Peristalsis stops and the patient has abdominal pain, distension, nausea, vomiting, and poor appetite.
Nursing care on the postoperative unit consists of measuring the patient's abdominal girth for distension and auscultating the abdomen in all four quadrants to determine presence, frequency, and characteristics of bowel sounds.
does not resolve spontaneously, the patient may require diagnostic tests to rule out mechanical blockage that would require surgical intervention.
An SSI is an
infection that occurs within 30 days of surgery or up to 1 year after implant surgery.
• Purulent discharge
• Isolation of organisms from wound fluid or tissue
• Pain, tenderness, local edema, warmth
• Health care provider diagnosis
Wound dehiscence
(separation and disruption of previously joined wound edges) may be preceded by a sudden discharge of brown, pink, or clear drainage.
Wound evisceration
(protrusion of the visceral organs though a wound opening) can occur after surgery and is considered a medical emergency. If evisceration occurs, the nurse needs to place sterile, saline-soaked towels over any extruding tissue, keep the patient on NPO status, observe the patient for signs and symptoms of shock, and call the surgeon immediately.
Delirium tremens is a reaction characterized by
restlessness, insomnia, nightmares, tachycardia, apprehension, confusion and disorientation, irritability, and auditory or visual hallucinations.
Expected Drainage From Tubes And Catheters
Urine∗
500–700mL, 1–2 days postoperative; 1500–2500mL thereafter (output = 0.5–1mL/kg/hr)
Clear, yellow
Ammonia
Watery
Gastric contents
≤1500mL/day
Pale, yellow–green, brown
Bloody following gastrointestinal surgery
Sour
Watery
Wound drainage
Variable with procedure
Variable with procedure
Usually serosanguineous
Same as wound dressing
Variable
Bile
500mL
Bright yellow to dark green
Acid
Thick
Postanaesthesia Discharge Criteria
• Patient awake (or baseline)
• Vital signs stable
• No excess bleeding or drainage
• No respiratory depression
• Oxygen saturation >90%
• Report given
Ambulatory Surgery Discharge Criteria
• All PACU discharge criteria met
• No IV opioids for last 30 minutes
• Minimal nausea and vomiting
• Voided (if appropriate to surgical procedure or orders)
• Able to ambulate if age appropriate and not contraindicated
• Responsible adult present to accompany patient
• Written discharge instructions given and understood
1. When a client is admitted to the PACU, what are the priority interventions the nurse performs?
a. Assess the surgical site, noting presence and character of drainage.
b. Assess the amount of urine output and the presence of bladder distension.
c. Assess for airway patency and quality of respirations and obtain vital signs.
d. Review results of intraoperative laboratory values and medications received.
c. Assess for airway patency and quality of respirations and obtain vital signs.
2. A client is admitted to the PACU after major abdominal surgery. During the initial assessment, the client states, “I am going to throw up.” What would be the priority nursing intervention?
a. Increase the rate of the IV fluids.
b. Obtain vital signs, including O2 saturation.
c. Position client in lateral recovery position.
d. Administer antiemetic medication as ordered.
c. Position client in lateral recovery position.
3. After admission of the postoperative client to the clinical unit, which assessment data require the most immediate attention?
a. O2 saturation of 85%
b. Respiratory rate of 13/min
c. Temperature of 38°C
d. Blood pressure of 90/60 mm Hg
a. O2 saturation of 85%
4. A 70-kg postoperative client has an average urine output of 25 mL/hr during the first 8 hours. Given this assessment, what would the priority nursing intervention(s) be?
a. Perform a straight catheterization to measure the amount of urine in the bladder.
b. Notify the physician and anticipate obtaining blood work to evaluate renal function.
c. Continue to monitor the client because this is a normal finding during this time period.
d. Evaluate the client’s fluid volume status since surgery and obtain a bladder ultrasound.
d. Evaluate the client's fluid volume status since surgery and obtain a bladder ultrasound.
5. The nurse on the postoperative unit is caring for a client who had a laparoscopic partial colectomy. On postoperative day 2, the client reports abdominal distension and discomfort. Which of the following interventions may be appropriate for this client? (Select all that apply.)
a. Increase the dose of opioids for pain relief.
b. Insert a nasogastric tube.
c. Reassure the client that this complication should subside in a day or two.
d. Monitor the client’s abdominal girth by measuring for distension and auscultate the abdomen in all four quadrants.
b. Insert a nasogastric tube.
c. Reassure the client that this complication should subside in a day or two.
d. Monitor the client's abdominal girth by measuring for distension and auscultate the abdomen in all four quadrants.
6. Discharge criteria for the phase II client include which of the following? (Select all that apply.)
a. No nausea or vomiting
b. Ability to drive themselves home
c. No respiratory depression
d. Written discharge instructions understood
e. Opioid pain medication given 45 minutes ago
c. No respiratory depression
d. Written discharge instructions understood
e. Opioid pain medication given 45 minutes ago