Exam 2 pt 1
1/72
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
73 Terms
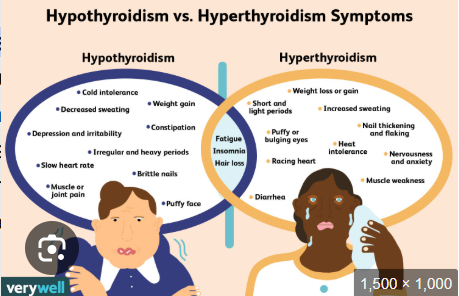
hyper vs hypo thyroidism and both
Muscle weakness
Cold intolerance
Anxiety and nervousness
Puffy face
Tachycardia
Brittle nails
Weight gain
Diarrhea
Insomnia
Hair loss
Short and light periods
Decreased sweating
Bulging eyes
Constipation
Heat intolerance
Depression and irritability
Fatigue
Increased sweating
Nail thickening and flaking
Bradycardia
Irregular and heavy periods
Muscle/joint pain
Weight loss
HYPOTHYROIDISM
define
etilogy/cause (3)
prevention?
Reduced or absent hormone secretion from thyroid gland, results in decreased metabolism
Etiology: Hashimoto’s, thyroid surgery, Radioactive iodine (RAI) therapy treatment
No prevention, key is early detection
think: body SLOWS DOWN

HYPOTHYROIDISM: recognize cues
s/s
labs (3)
what can it cause and interventions (3)
what to report (1)
at risk for (1)
TX (1)
• Decreased metabolism
• Sleepy, weakness, anorexia, muscle aches, paresthesia
• Constipation, cold intolerance, low libido
• Labs: Reduced T3, T4, TSH high
Decreased gas exchange
- Monitor oxygenation
Reduced perfusion
- Monitor BP, HR/rhythm
- Report chest pain
Risk for myxedema coma: medical emergency
- TX: Lifelong thyroid replacement
MYXEDEMA COMA
hypothyroidism or hyperthyroidism
what is it
s/s (6)
hypothyroidism
Serious, rare complication
Dangerously reduced cardiopulmonary and neurologic function
Reduced LOC, cognition
Respiratory failure
Hypotension
Hyponatremia
Hypothermia
Bradycardia
Emergent treatment
HYPOTHYROIDISM: CARE COORDINATION AND TRANSITION MANAGEMENT
what medication is used to treat hypothyroidism? (1)
Home care management
Self-management education
Hormone replacement therapy and side effects
Levothyroxine (Synthroid): lee - vow - thigh - rocks - in
Monitor and SE
Health care resources
HYPERTHYROIDISM
define
etiology/causes (3)
Excessive thyroid hormone secretion from thyroid gland, results in hypermetabolism and increased Sympathetic nervous system (SNS) activity (fight or flight) (increased: bp,hr, rr)
Etiology: Graves’, Toxic multinodular goiter, excess thyroid hormone replacement
HYPERTHYROIDISM: recognize cues
s/s
conditions (3)
labs (4)
diagnostics (3)
• Weight loss, increased appetite, heat intolerance, vision changes
• Exopthalamos (buldging eyes), eyelid retractions, goiter
• Labs: High T3, T4, low TSH, TRAb Thyrotropin Receptor Antibody (TRAb): used to diagnose Graves' disease (positive if high)
• Diagnostics: high: RAIU (radioactive iodine uptake), US (ultrasound, enlarged thyroid), ECG
HYPERTHYROIDISM:
medical management (3)
surgical management (1)
Medical management:
• Drug therapy
• Methimazole: meh - thin - ah -zole
• Iodine
• RAI therapy
Surgical management:
partial or total thyroidectomy
SURGICAL PRIORITIES: THYROID
preoperative (2)
Thionamide
postoperative: interventions (2) risks (4)
Preoperative
• Thionamide (thigh-oh-mide) drug to regulate thyroid
• Iodine prep
• Normal pre-op priorities
Postoperative
• Avoid neck extension, monitor ABCs
• Risks: hemorrhage, compromised airway, parathyroid injury (low Ca), laryngeal nerve damage
ACUTE THYROTOXICOSIS (THYROID STORM)
hypo or hyperthyroidism
define
results from (1)
s/s (10)
management (3)
hyperthyroidism
Excessive amounts hormones released
• Life-threatening emergency
• Results from stressors
Manifestations:
• Severe tachycardia, HF
• Shock
• Hyperthermia
• Agitation, seizures, coma
• N/V/D
Management:
• Aggressive treatment w/ meds
• Monitor for dysthymias
• ABCs
THYROID CANCER
types (4) FAMP
• Papillary
• Follicular
• Medullary
• Anaplastic
HYPOPARATHYROIDISM
define
when can it occur
monitor
tx
Decreased function of parathyroid gland; serum calcium levels cannot be maintained (LOW CALCIUM LEVELS) (normal range: 8.5 and 10.5 mg/dL)
Occurs post-surgically after thyroid or parathyroid removal, or after surgery for head and neck cancer
Monitor
calcium
Treatment
high-dose calcium supplements,
HYPERPARATHYROIDISM
define
causes what (2)
monitor: (3)
tx: (3)
Increase in parathyroid hormone; hypercalcemia ( > 10.5); hypophosphatemia (normal: 2.5 and 4.5 mg/dL)
monitor for:
Kidney stones, calcium deposits, bone lesions
Treatment
Drug therapy via cinacalcet (sin- uh-kal-set), bisphosphonates, Parathyroidectomy
A 42-year-old female seeing her primary health care
provider. She reports being tired all the time, and
muscle aches and pains. Assessment reveals a heart
rate of 54/min and a BP of 94/60. The nurse notes non-
pitting facial edema especially around the eyes, and in
the hands and feet. The client’s health history includes
radioactive iodine (RAI) for hyperthyroidism.
1. Which condition does the nurse anticipate this client
has?
hypothyroidism
The primary health care provider orders laboratory work that includes thyroid function tests.
2. Which results does the nurse anticipate?
A. Normal T3 and T4 levels
B. Decreased TSH level
C. Increased T3 and T4 levels
D. Decreased T3 and T4 levels
D
4. Which teaching points will the nurse include about this condition? (Select all that apply.)
A. “Eat a low-fiber diet and drink plenty of fluids.”
B. “Keep a record of how many hours you sleep in a 24-hour period.”
C. “Report any difficulty with orientation to time, place, or person.”
D. “Take your medication every day at the same time.”
E. “Call the provider if you develop an unsteady gait or hand tremors.”
BCDE
The nurse has provided teaching about hypothyroidism.
Which client statement indicates that further nursing
teaching is needed?
A. “I will check my heart rate and BP every day.”
B. “I will include fiber in my diet and drink plenty of water.”
C. “I will call my provider if I notice any changes in level of consciousness.”
D. “I will no longer need to take medication when I feel better in a few months.”
D
What are the priority nursing interventions for
Maria during the acute phase?
Why is temperature monitoring critical in
hyperthyroidism management?
What complications should the nurse monitor for
if Maria requires thyroid surgery?
What patient teaching is essential before RAI
therapy?
How would you address Maria's concerns about
her eye changes?
What are the priority nursing interventions for Maria during the acute phase?
Monitor vital signs
Why is temperature monitoring critical in hyperthyroidism management?
If overheated it can trigger a thyroid strom
What complications should the nurse monitor for if Maria requires thyroid surgery?
Bleeding/hemorrhage , compromised airway, nerve damage, ABCs , infection
What patient teaching is essential before RAI therapy?
Chemo precautions
How would you address Maria's concerns about her eye changes?
Discuss that hey hyperthyroidism has caused it and go over graves disease and that there are surgical options available for her. Tell her to use artificial tears

hypocalcemia s/s (6)
tingling or numbness (especially in lips, fingers, feet)
muscle cramps or spasms
fatigue or lethargy
mood changes like irritability or confusion
positive Chvostek (sh-vos-tec) sign
positive trousseau (True- sew) sign
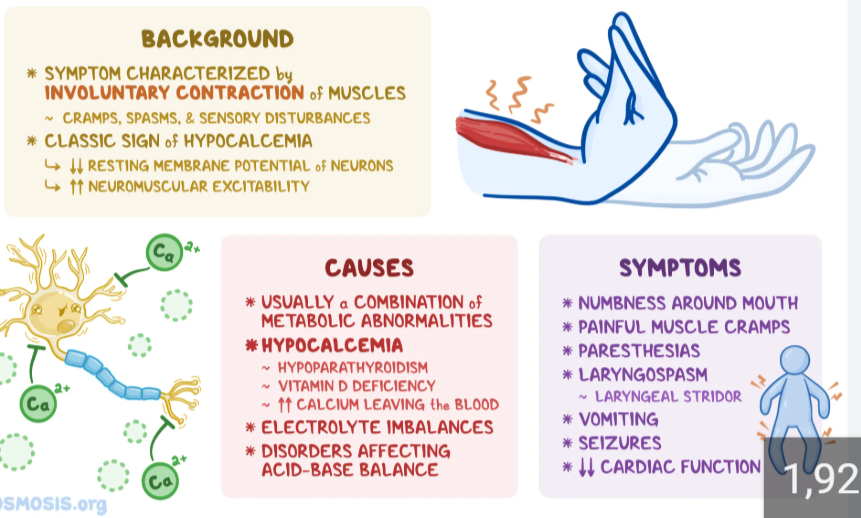
what meds can you give for low calcium
tums ( calcium carbonate)
IV calcium
Diabetes: pathophysiological review
glucose: how is it absorbed, what does it stimulate
insulin: how’s it stimulated, what does it do
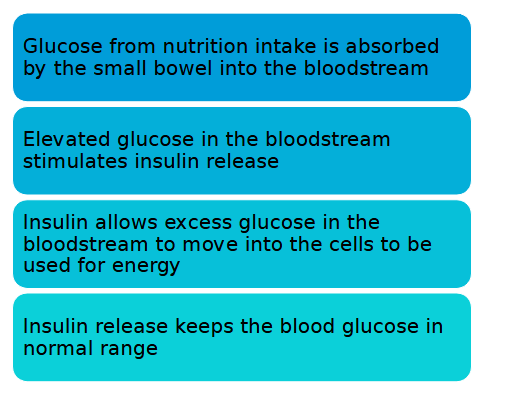
normal insulin metabolism
action of insulin
expected glucose range
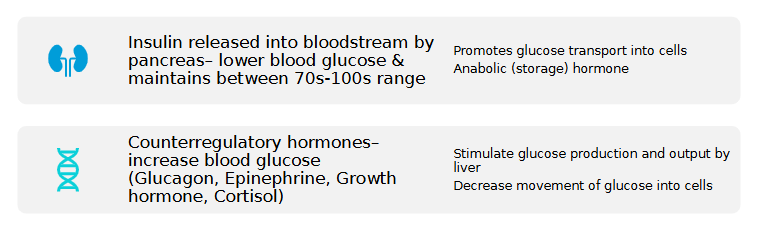
action of counterregulatory (bodily agents that oppose insulin ) hormones and examples (4)
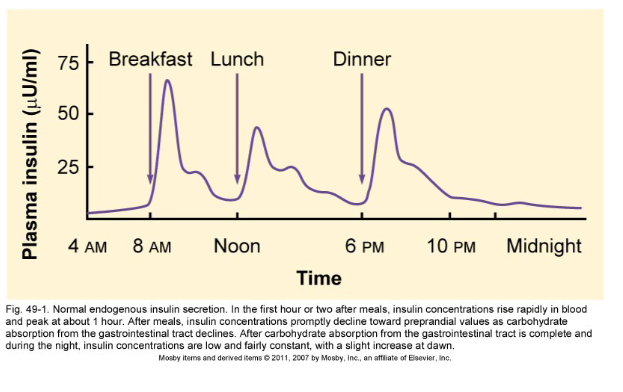
when does insulin rise rapidly in blood
when does it peak
when does it decline
Insulin raises rapidly in blood in the first hour or two after eating a meal
Insulin peaks at about 1 hour
Insulin declines after eating a meal
Diabetes Mellitus
define
causes (2)
increases risk of what (2)
DM: Chronic multisystem disease characterized by hyperglycemia
• Abnormal insulin production
• Impaired insulin use
Risks: Increased risk of heart disease and stroke for patients with DM
Diabetes types:
Type 1
Type 2
• Latent Autoimmune Diabetes of Adulthood (LADA)
• Maturity-Onset Diabetes of the Young (MODY)
• Gestational DM
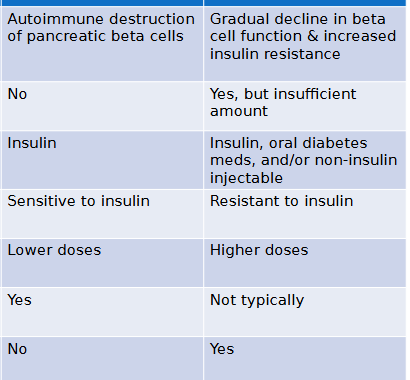
Type 1 Diabetes
An autoimmune condition where the pancreas produces little to no insulin because the immune system attacks and destroys insulin-producing beta cells. It typically requires lifelong exogenous insulin administration.
Type 2 Diabetes
A metabolic disorder characterized by insulin resistance, where the body’s cells do not respond effectively to insulin. Over time, the pancreas may also fail to produce enough insulin to maintain normal glucose levels.
Latent Autoimmune Diabetes of Adulthood (LADA)
Often called "Type 1.5," this is a slow-progressing form of autoimmune diabetes that occurs in adults. It is frequently misdiagnosed as Type 2 initially, but it eventually requires insulin as beta cell function declines.
Maturity-Onset Diabetes of the Young (MODY)
A rare form of diabetes caused by a mutation in a single gene (monogenic). It usually presents before age 25 and is inherited through families, affecting how the body produces or uses insulin without the presence of autoimmunity or obesity.
Gestational DM
High blood glucose levels that are first recognized during pregnancy. It occurs when placental hormones cause insulin resistance that the mother's pancreas cannot overcome, typically resolving after childbirth but increasing future risk for Type 2.
Type 1 (insulin dependent)
define
what’s required
what absent
s/s: 6
without treatment can lead to what
• Autoimmune body’s own T cells attack & destroy β cells
(source of insulin)
• β cells continue to be destroyed (80-90% reduction) until make NO insulin!
• Insulin REQUIRED for all humans! →Exogenous insulin
• NO ENDOGENOUS INSULIN!!- Pancreas makes NO insulin!
• Genetic predisposition/exposure to virus
• Usually affects people under 40 yrs.
• S/S: polydipsia, polyuria, polyphagia, fatigue, wt. loss, blurred vision
• Without treatment DKA
Type 2 (non-insulin dependent)
describe
what’s present
whats needed
#1 risk factor
s/s the three P’s + 5
onset
4 metabolic abnormalities
Insulin insufficient to meet needs or cells resistant to action of insulin, or both
ENDOGENOUS INSULIN PRESENT! (main difference from Type I)
• Exogenous insulin needed to supplement
Usually affects people >35yrs, but more Kids lately
#1 Risk factor= Obesity
The "3 P's" of diabetes—Polyuria (frequent urination), Polydipsia (excessive thirst), and Polyphagia (extreme hunger)
S/S: fatigue, recurrent infections, prolonged wd. healing, visual changes (blurred vision), numbness or tingling in hands or feet
onset: gradual! But progressive
4 metabolic abnormalities:
• Insulin resistance
• Decreased insulin production (pancreas)
• Inappropriate glucose production (liver)
• Adipokines alter glucose & fat metabolism
type 1 (5-10% of diabetes) vs type 2 (90-95% of diabetes)
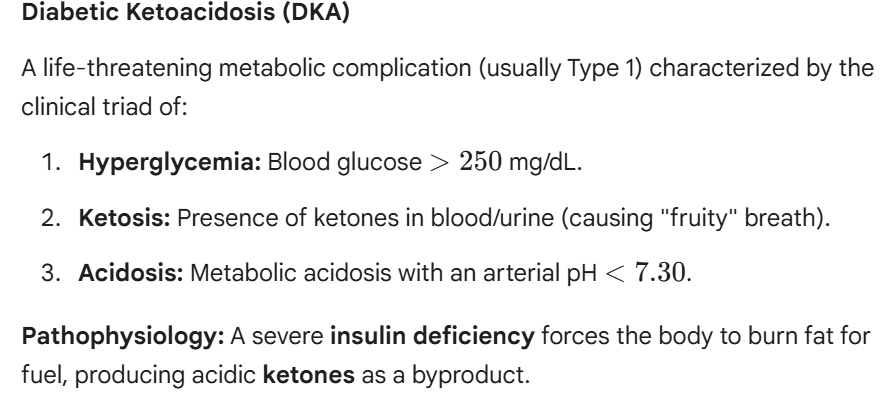
DKA: Diabetic Ketoacidosis
associated with what type of diabetes
define
s/s (3)
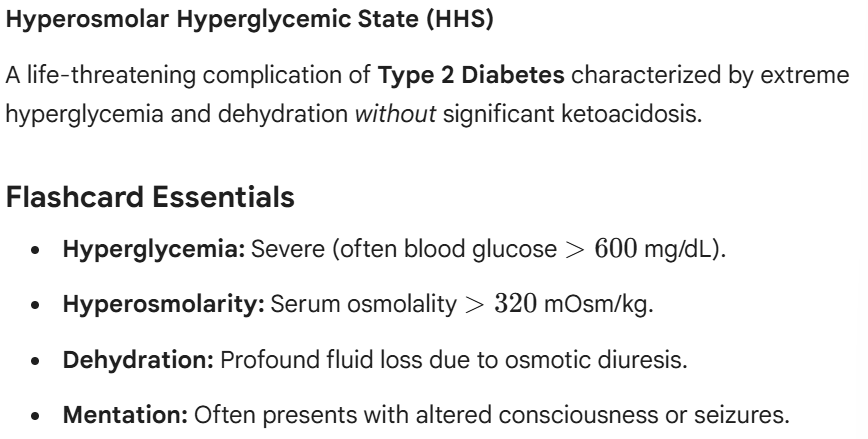
HHS: Hyperosmolar Hyperglycemic State
define
associated with what type of diabetes
s/s (4)
big difference from DKA
Unlike DKA, there is enough circulating insulin to prevent the breakdown of fats into ketones, so acidosis is absent (pH stays > 7.30)
Latent Autoimmune Diabetes of Adulthood (LADA)
define (2)
also referred to as
when is it DX
Slow, progressive form of autoimmune diabetes
Sometimes referred to as Type 1.5
Varying degrees of insulin resistance
Diagnosed >30 years of age
Maturity – Onset Diabetes of the Youth (MODY)
define
chacteristics
it is not what
when is it DX
Inherited mutation in one of at least six known genes that results in loss of insulin function and hyperglycemia
Usually diagnosed in younger adults but can be found at any time in adulthood
Resembles T1DM with insulin requirements and potential for diabetic ketoacidosis (DKA)
It is NOT an autoimmune condition
Gestational Diabetes
when does it develop
high risk factors (3)
complications (3)
1st line tx
risks
Develops during Pregnancy, 2nd or 3rd trimester
High Risk (screen at 1st visit): obesity, advanced maternal age, strong family history of DM2
Complications: C-section, perinatal death, neonatal complications
1st line: Nutrition Therapy, then move to insulin if needed
Risk of developing DM 2 increases (50%) as well as future pregnancies
Diabetes: cues: assessment
HX
Labs
labs also include glucose tolerance test
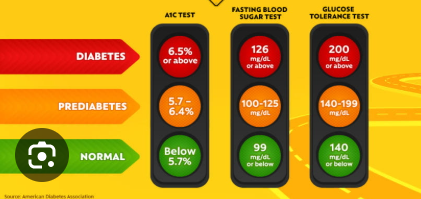
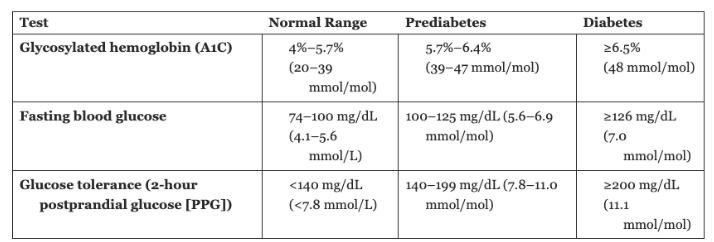
Lab Assessment: Normal range, prediabetes, diabetes
Glycosylated hemoglobin (A1C)
fasting blood glucose
glucose tolerance (2-hour postprandial glucose (PPG))
diabetes: ongoing assessment (3)
Glycosylated hemoglobin (A1C),
Continuous glucose monitoring (CGM)
Blood glucose monitoring (BGM)
A patient with type 1 diabetes mellitus is learning about blood glucose monitoring. The nurse teaches the patient to check blood glucose before meals. What is the recommended preprandial glucose target range?
A. 50 to 100 mg/dL (2.8–5.6 mmol/L)
B. 80 to 130 mg/dL (4.4–7.2 mmol/L)
C. 100 to 180 mg/dL (5.6–10.0 mmol/L)
D. 140 to 200 mg/dL (7.8–11.1 mmol/L)
B
diabetes: analyze cues and prioritize hypotheses: analysis
priority collaborative problems for pts with DM (5)
• Potential for injury due to hyperglycemia
• Potential for surgical complications due to health complexities with DM
• Potential for injury due to peripheral neuropathy
• Potential for kidney disease due to reduced kidney perfusion
• Potential for acute complications associated with glucose related emergencies: DKA or HHS
Metabolic syndrome
factors (4)
• Simultaneous presence of metabolic factors that increase risk for type 2 DM
• Abdominal obesity
• Hyperglycemia
• Hypertension
• Hyperlipidemia
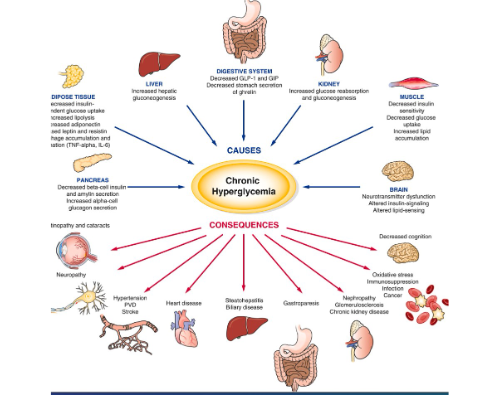
chronic hyperglycemia
causes
consequences
negativly effects all aspects of body
Diabetes: Generate Solutions & Take Action: Planning and Implementation (5)
• Preventing injury from hyperglycemia
• Enhancing surgical recovery
• Preventing injury from peripheral neuropathy
• Reducing the risk for kidney disease
• Preventing complications
diabetes: planning & implementing
non pharmacologic (5)
drug therapy (6)
NON PHARMACOLOGIC
• Pt & Caregiver Teaching
• Follow up programs
• Nutrition therapy
• Exercise therapy
• Self-monitoring of blood glucose (SMBG)
DRUG THERAPY
• Insulin
• Oral agents
• Enteric-coated Aspirin
• ACE inhibitors
• ARBs
• Antihyperlipidemic drugs
diabetes: pharmacological interventions things to think about
• Medication selection
• Cost
• Patient’s ability to manage multiple medications
• Side effects
• Patient’s body in response to the medication
• Polypharmacy
diabetes: pharmacological interventions: classifications, suffix and meds. MATCH
Classes:
biguanides
incretin Mimetics (GLP-1 agonists)
sodium-glucose cotransporter 2 (SSGLT2) inhibitors
DPP-4 inhibitors
insulin stimulators (secretagogues) (2)
insulin sensitizers
alpha-glucosidase inhibitors (2)
amylin analogs
MEDS:
Sulfonylureas
Ending in –tides
Metformin
Miglitol
Thiazolidinediones
Ending in -flozin
Pramlintide
Meglitinide (Glinides)
Ending in –gliptin
Acarbose
• Biguanides
• Metformin
• Incretin Mimetics (GLP-1 Agonists)
• Ending in –tides
• Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors
• Ending in -flozin
• DPP-4 Inhibitors
• Ending in –gliptin
• Insulin Stimulators (Secretagogues)
• Sulfonylureas
• Meglitinide (Glinides)
• Insulin Sensitizers
• Thiazolidinediones
• Alpha-Glucosidase Inhibitors
• Acarbose
• Miglitol
• Amylin Analogs
• Pramlintide
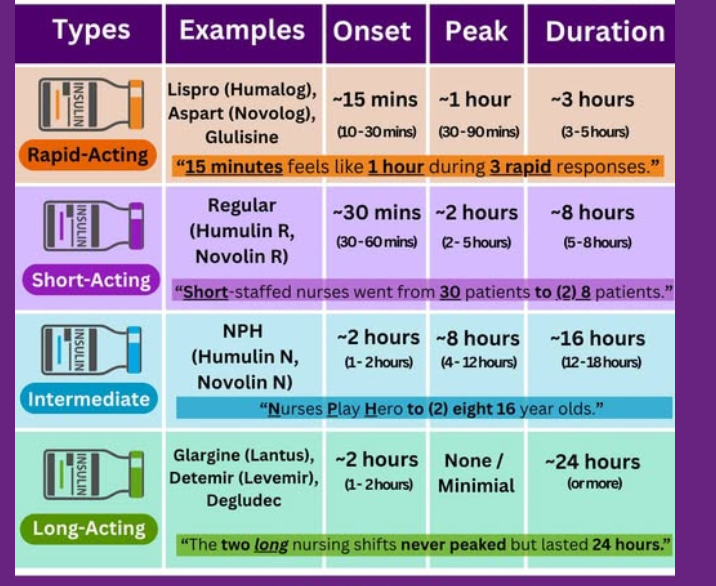
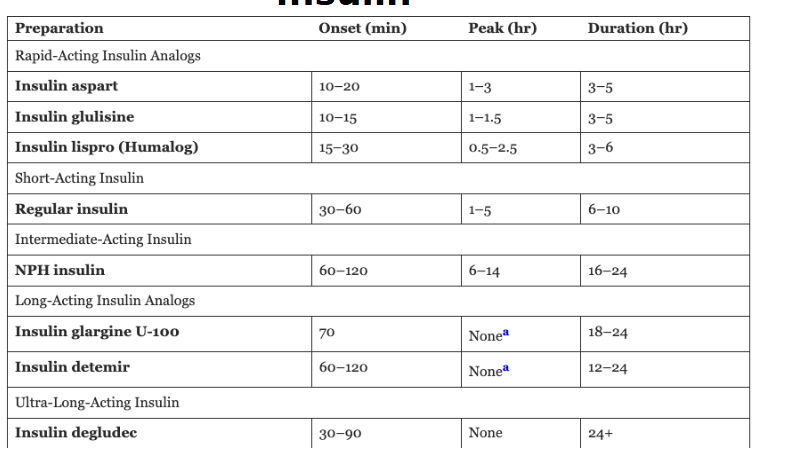
insulin:
put meds in categories:
insulin detemir
insulin aspart
regular insulin
insulin degludec
insulin glulisine
NPH insulin
insulin lispro (Humalog)
insulin glargine U-100
Type: Onset (min), Peak (hr), Duration (hr)
rapid acting (3)
short acting
intermediate acting
long acting (2)
ultra long acting
nutritional therapy
what to watch
diabetes: physical activity
what can it help with (2)
education (2)
• Can decrease insulin requirements
• Can improve cardiovascular disease
• Depending on severity of diabetes some
patients may need to alter exercises
• Educate patients to check glucose levels
before exercise
Health Promotion/Disease Diabetes Prevention (3)

Care of Patients with Hematologic (blood) Conditions
priority concepts (2)
the interrelated concepts in this chapter are (5)
The priority concepts:
• Perfusion
• Immunity
• The interrelated concepts in this chapter are
• Cellular Regulation
• Clotting!!!
• Gas exchange
• Infection!!!
• Pain!!!
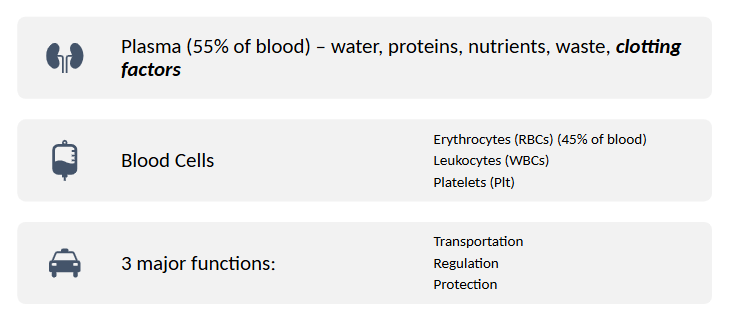
Blood
plasma %
other components (5)
blood cells & % (3)
3 major functions
Thrombocytopenia
define
leads to (3)
risk (1)
inherited or acquired?
Types: (4)
pt education (4)
Define: Thrombocytopenia: abnormally low platelet levels (< 150,000/uL) in the blood
leading to impaired clotting, easy bruising, and excessive bleeding. BLEEDING RISKS
can be inherited or acquired
Types:
• Immune thrombocytopenic purpura (ITP)
• Thrombotic thrombocytopenic purpura (TTP)
• Heparin-induced thrombocytopenia (HIT+)
• Acquired thrombocytopenia from decreased platelet production
Education: Bleeding precautions: avoiding contact sports, using soft toothbrushes, electric razors, and wearing protective footwear.
Normal platelet count
154,000-450,000
IMMUNE Thrombocytopenia Purpura (ITP)
platelets are coated with what
what does the body do in response
treatment (3)
what to avoid and why (1)
what do Romiplostim (Nplate) & eltrombopag (Promacta) do?
• Platelets are coated with antibodies.
• Body recognizes this and DESTROYS them. (ITP)
• Treatment –
• Steroids
• IV IgG
• Splenectomy
Avoid IM injections- to help prevent bleeding!!!
*Romiplostim (Nplate) & eltrombopag (Promacta) increase production of platelets
Heparin Induced Thrombocytopenia (HIT+)
define
leads to (2)
Treatment (2)
alternatives to heparin (3)
define: Immune mediated adverse drug reaction caused by the emergence of antibodies that activate platelets in the presence of heparin
Leads to: Platelet count plummets, micro clots occur
Treatment:
stop heparin
send a HIT test
alternatives to heparin:
Anticoagulate with IV lepirudin or argatroban (LA)
Plus warfarin for a few weeks
Neutropenia
define
primary risk
what to monitor, how to calculate (steps 1-4), normal, when to be concerned, when is it severe
neutropenic precautions
patient education
define: low neutrophils (WBC) (<1000cells/uL)
primary risk infection
Monitor: Absolute Neutrophil Count (ANC)
How to monitor ANC:
1. Find the WBC, the polys and bands on your CBC.
WBC 2.0
Polys 14.8%
Bands 5%
2. Add the polys and bands.
(14.8 + 5 = 19.8)
3. Multiply the sum of the polys and bands by the WBC.
19.8 x 2.0 = 39.6
4. Multiply the product by 10.
- 39.6 x 10 = 396
The normal range for the ANC = 1.5 to
8.0 (1,500 to 8,000/mm3).
ANC: CONCERN when <1,000, severe when <500
Neutropenic precautions:
wash hands often
no flowers
avoid flossing
use electric razor
avoid crowds or sick people
no fresh fruits of veggies
take temp often (emergency > 100.4)
Patent education:
• Limit Visitors
• Diet – fruits/veg?
• Monitoring temp frequently
• Mask, crowds
• T>100.5 = CALL, draw blood cultures
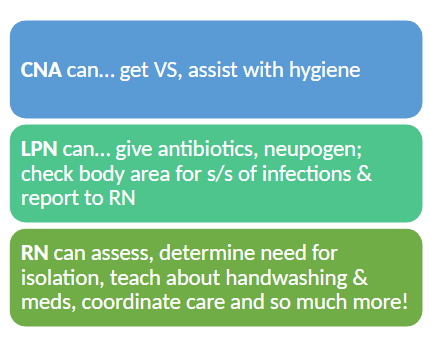
Delegation in Neutropenia:
CNA
LPNRN
Hemophilia and von willebrand’s disease
what are they
risks (1)
interventions (1)
supportive care (3)
patient education (4)
Disorders that cause defective or deficiency in clotting factors. (effect clotting cascade)
High bleed risk, take preventative measures.
If they do bleed, replace missing Factors, can do preventatively.
Supportive care (transfuse, oxygen, IV fluids, etc.)
Teach them same as Thrombocytopenia (bleeding risks what to avoid):
avoiding contact sports, using soft toothbrushes, electric razors, and wearing protective footwear.
Von Willebrand Disease
effects what percent of population
define
treatment (4)
• 1% of population
• Missing von Willebrand Factor for clotting (glycoprotein)
• Treatment:
• DDAVP (desmopressin) makes the body release more vWF
• Factor VIII (8)
• Birth control pills – estrogen ^VWF & FVIII release
• Pain meds?
Hemophilia
define
• The Royal Disease (Queen Victoria)
• X-linked recessive gene – Mom-> son
• Missing Factor VIII (8) or IX (9)
BLOOD CANCERS
new section
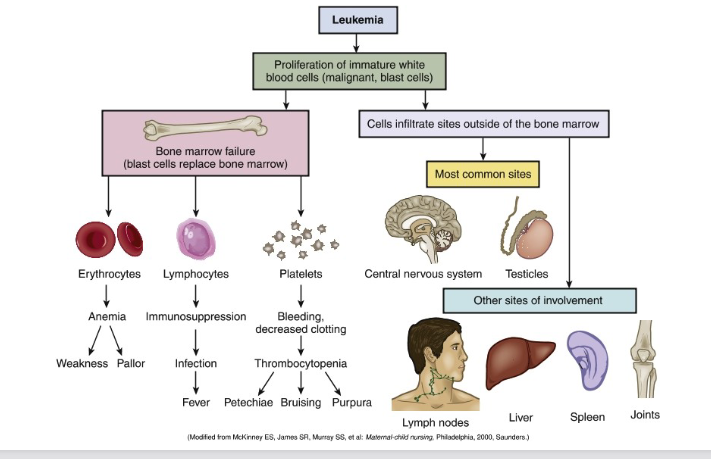
Leukemia (Myelodysplastic Synd (MDS)
define
leads to (3)
Bone marrow cranks out immature abnormal leukocytes
causes: Abnormal WBC accumulate (don’t have normal cell cycle) - become overcrowded
Abnormal WBCs clog spleen, liver, lymph, bone, etc. Even develop solid masses
no single cause: Can be genetic and environmental radiation, chemicals, viral infxn
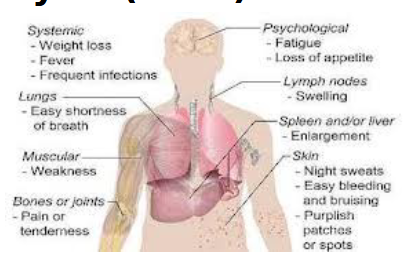
Leukemia
define
caused by
leads to
most common sites
other sites involved
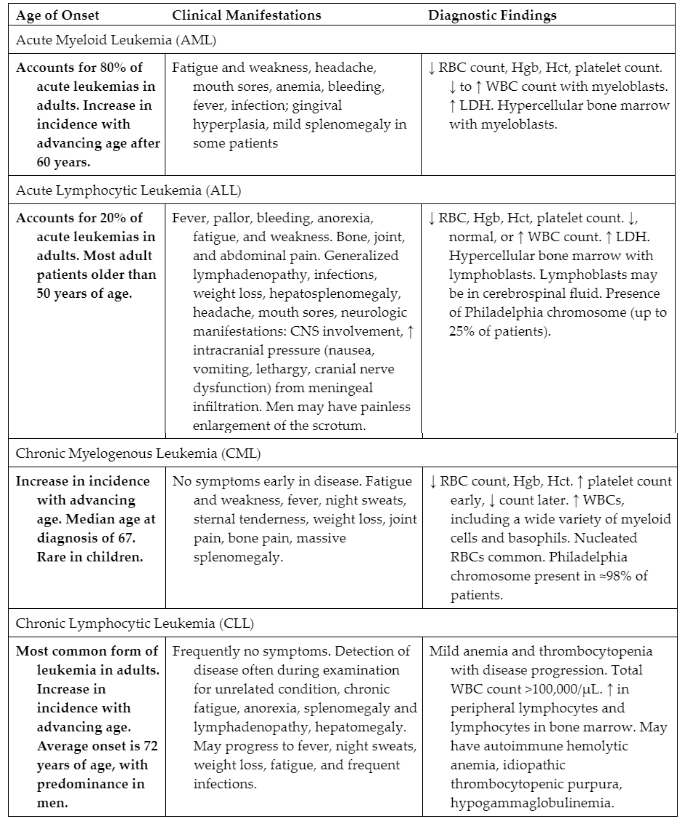
Leukemia Classifications
four types of leukemia cancers
based on what (5)
• Based on onset, clinical manifestations and clinical findings
• Acute or Chronic
• Myelogenous (RBC) or Lymphocytic (WBC)
• Four types of leukemia cancers:
• 1/3 acute myeloid leukemia AML (immature cells) – Allogeneic hematopoietic stem cell transplant (HSCT), INDUCTION sends 70% into remission
• ¼ acute lymphocytic leukemia ALL
• chronic myelogenous leukemia CML
• chronic lymphocytic leukemia CLL
Types of leukemia
chronic or acute
type of bone marrow cells that are affected
lymphocytes
myeloid cells
• Chronic or Acute - Are the cells mature
(look like normal white blood cells) or
immature (look more like stem cells)?
• Type of bone marrow cells that are affected
• Lymphocytes, it is called lymphocytic leukemia
• Early forms of myeloid cells -- white
blood cells (other than lymphocytes), red
blood cells, or platelet-making cells
(megakaryocytes) -- are myeloid
leukemias (also known as myelocytic,
myelogenous, or non-lymphocytic
leukemias)
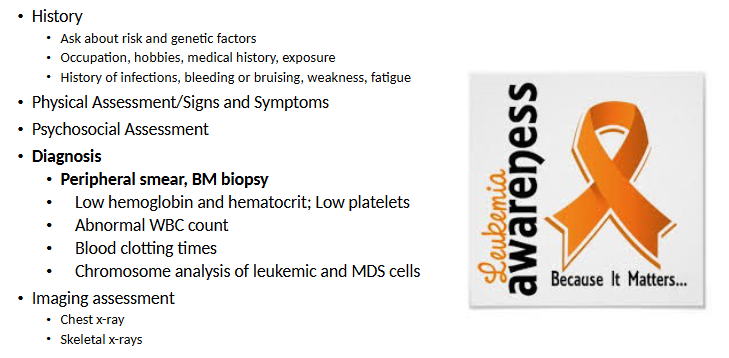
LEUKEMIA: Recognize Cues
hx
assessment and s/s
psyche assessment
how to dx
imaging assessment
LEUKEMIA: Analyze Cues & Prioritize Hypotheses
• Potential for infection due to reduced Immunity and chemotherapy
• Potential for injury due to poor clotting from thrombocytopenia and
chemotherapy
• Fatigue due to reduced gas exchange and increased energy demands
LEUKEMIA: Generate Solutions & Take Action:
Planning & Implementing
• Preventing infection and promoting immunity
• Minimizing injury
• Conserving energy
Malignant Lymphomas – 5% of Cancers Recognize Cues: Assessment
originate in what
describe
s/s
interventions: early, limited advanced stage
• Originate in BM & lymph
• Large, painless lymph node(s)
• Fevers, night sweats, unplanned weight loss
• Some have no symptoms at time of diagnosis
Malignant Lymphomas Take Action: Interventions
• Early stage with favorable prognostic features: short duration of ABVD chemotherapy (usually two cycles including doxorubicin, bleomycin, vinblastine, and dacarbazine) followed by restricted involved-field radiation therapy (IFRT)
• Limited stage with unfavorable features: longer course of ABVD chemo (4-6 cycles) then, higher dose of IFRT
• Advanced stage: ABVD chemo without radiation
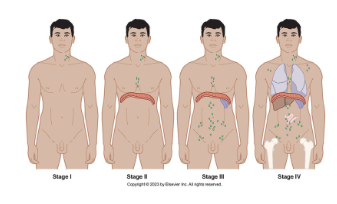
Hodgkin's Lymphoma (10% of lymphomas)
caused by
risk factors
describe
what gets destroyed
Multiple Myeloma
define
risk factors
assessments
treatment
Polycythemia Vera
define
assessment
interventions
Cancer of the RBCs
• Massive production of RBCs
• Excessive leukocyte production
• Excessive platelet production
• Recognizing Cues: Assessment
• Facial skin is flushed, warm
• Intense itching
• Hypertension!!!
• Poor gas exchange
• Bleeding problems
Interventions
• Fatal if untreated
• Therapeutic phlebotomy!!!
• Apheresis
• Increase hydration!!!
• Promote venous return
• Anticoagulants, other drug therapy!!!
A client with polycythemia vera is admitted with
shortness of breath, hypertension, and weak pulses in
the right foot. Which nursing intervention is the
priority?
A. Assess hydration status.
B. Evaluate blood pressure
C. Elevate lower extremities on pillows
D. Use soft-bristle toothbrush to prevent bleeding
A
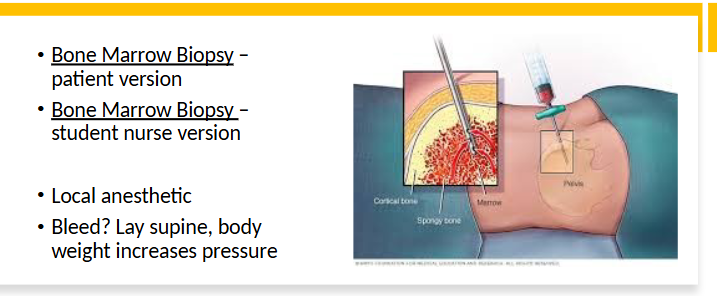
Bone Marrow Biopsy
pt position
med used
risk