CNS Infections (meningitis & encephalitis)
1/31
Earn XP
Description and Tags
2 lecture hours - includes classification of bugs that cause meningitis as FYI
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
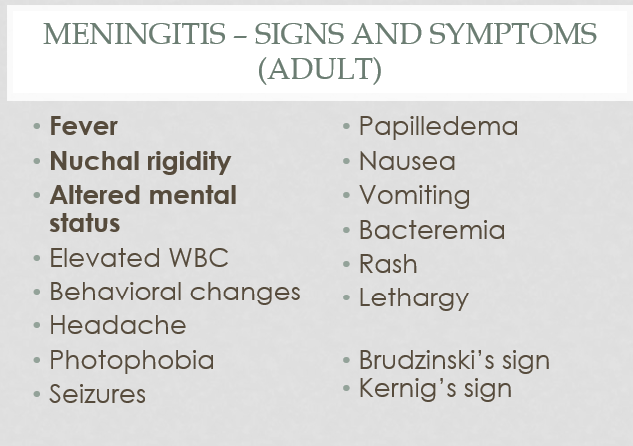
What are the big three s/s of meningitis in adults?
Fever
Nuchal rigidity
Altered mental status
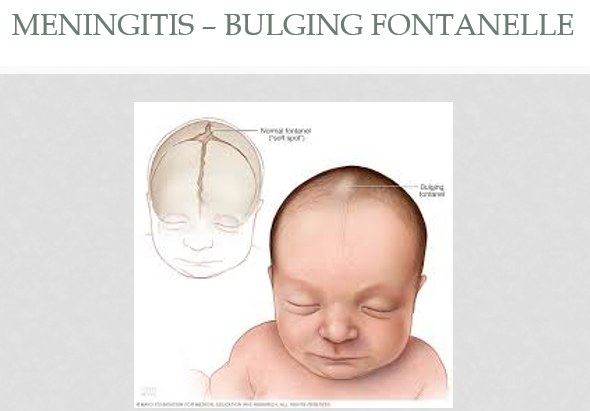
What are 3 major s/s of meningitis in pediatrics?
feeding intolerance
apnea
bulging fontanelle
What pathogen is most common for community acquired meningitis in the following age groups?
<1 month
1 month to <18 years
18-50 years
>50 years
<1 month - Group B Streptococcus
1 month to <18 years - S. pneumoniae
18-50 years - N. meningitidis
>50 years - N. meningitidis
What is the recommended empiric IV therapy for community-acquired meningitis in neonates?
ampicillin + cefotaxime
or
ampicillin + aminoglycoside
FYI - (ampicillin would cover the gram positives… GBS & listeria)
(cefoxatime or aminoglycoside would cover the gram (-)s = e.coli, klebsiella, and enterobacter)

What is the recommended empiric IV therapy for community-acquired meningitis in >1 month and older? (also for the one patient group that is different)
vanco + 3rd gen cephalosporin (ceftraixone)
vanco + 3rd gen cephalosporin + ampicillin as well in > 50 y/o
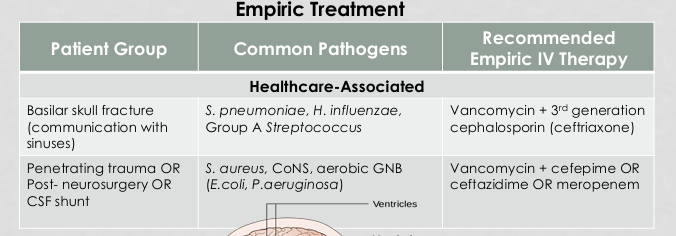
What is the recommended empiric IV therapy used for healthcare-associated meningitis in the patient group of a basilar skull fracture?
vanco + 3rd gen cephalosporin (ceftriaxone)
Bug that accounts for 58% of community-acquired meningitis
streptococcus pneumoniae
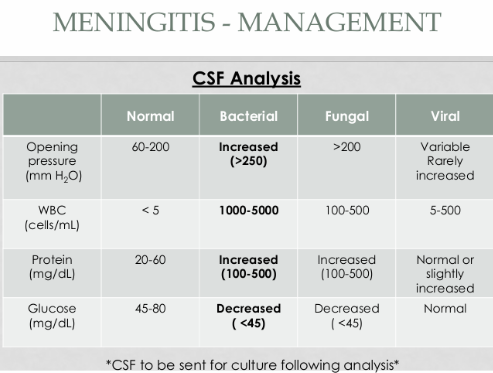
CSF findings change depending on the cause of meningitis (e.g., fungal, viral, bacterial).
Give the parameters for the following that are indicative of bacterial meningitis:
Opening pressure (mm H2O) (pressure where LP needle enters spinal canal)
WBC
Protein
Glucose
Opening pressure - increased (>250)
WBC - 1-5 x 10³
Protein - increased (100-500)
Glucose - decreased (<45)
-might be sufficient for exam to just know increased or decreased?
most important diagnostic test for meningitis and other CNS infections.
lumbar puncture
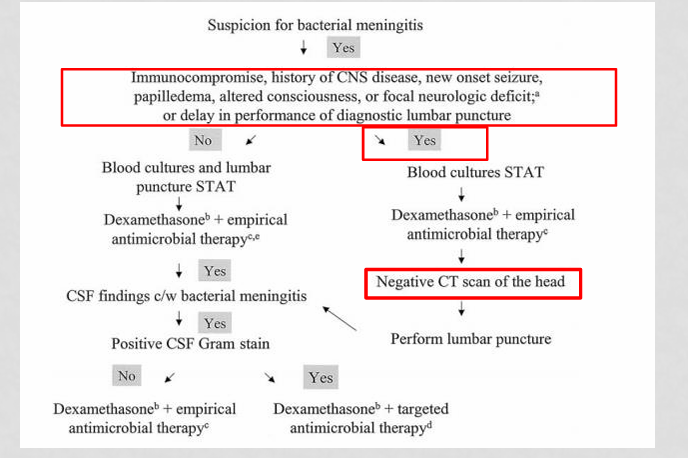
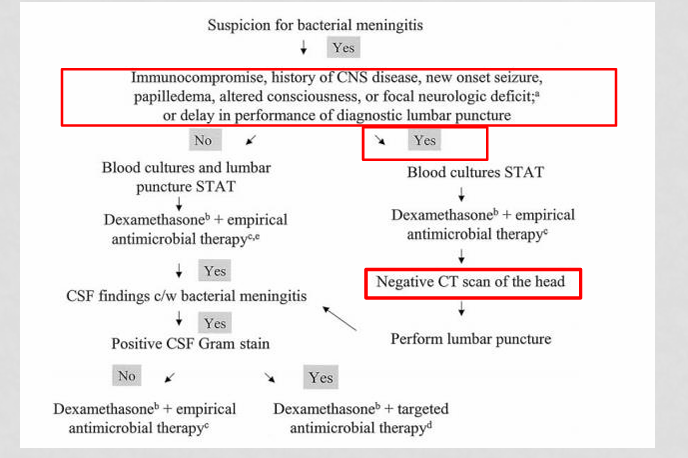
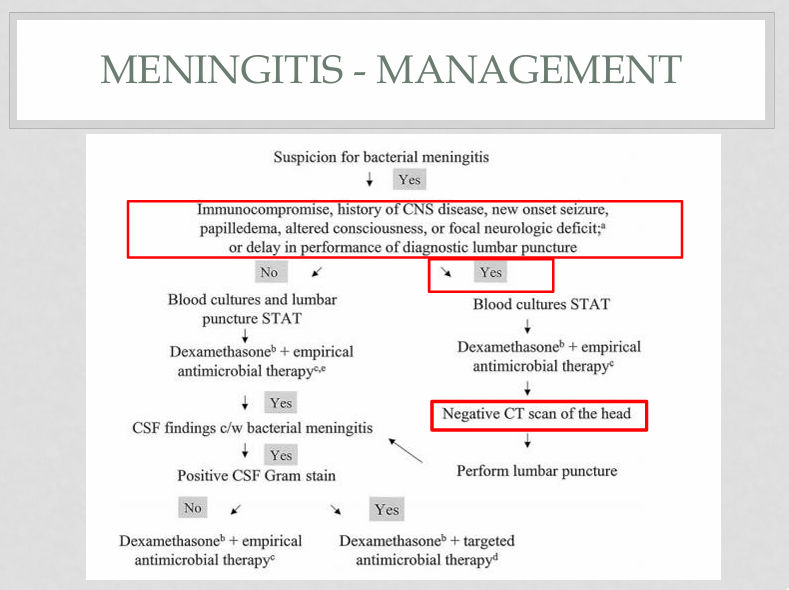
When a patient is admitted with a suspicion for bacterial meningitis:
First step when bacterial meningitis is suspected?
Determine if patient has risk factors requiring CT before lumbar puncture.
When a patient is admitted with a suspicion for bacterial meningitis:
Which patients require CT scan before lumbar puncture in suspected meningitis? List at least 2.
Immunocompromised
History of CNS disease
New onset seizure
Papilledema
Altered consciousness
Focal neurologic deficit
Delay in performing LP
When a patient is admitted with a suspicion for bacterial meningitis:
If NO CT risk factors are present in suspected meningitis, what should be done?
Blood cultures + lumbar puncture STAT
Then start dexamethasone & empiric antibiotics
When a patient is admitted with a suspicion for bacterial meningitis:
If CT risk factors ARE present in suspected meningitis, what is the next step?
Blood cultures THEN start dexamethasone + empiric antibiotics THEN Obtain CT scan
When do you perform CT before lumbar puncture in suspected meningitis?
if any of the risk factors… if not then blood cultures + LP ASAP
What are some of the pros and cons of adjunctive dexamethasone in the management of meningitits?
CONS - immunosuppression, decreased abx penetration into BBB, may mask WBC signs of abx response + normal steroid complications
PROS - image
The IDSA recommends dexamethasone 0.15mg/kg (up to 10mg) IV Q6H for up to 96 hours. When should it be administered?
Should be administered 10-20 minutes prior to, or concomitant with first dose of antimicrobial therapy
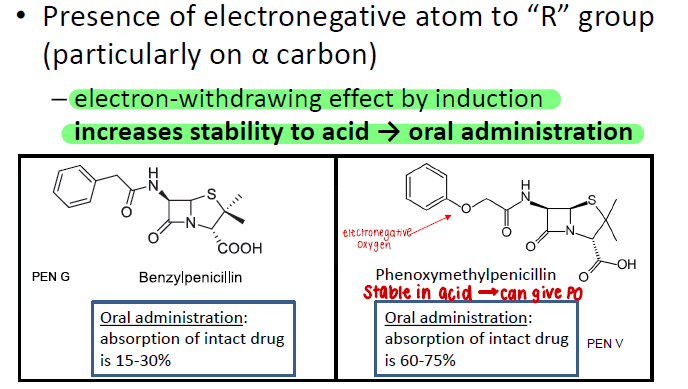
(FYI - from E2) What is the coverage of the natural penicillins? (Pen V and Pen G)
streptococci
meningococci (n. meningiditis)
syphilis
clostridium
(narrow)
(FYI - from E2) What is the coverage of the 3rd gen cephalosporins?
resistant streptococci (like s. pneumoniae and viridans)
staph
gram positive anaerobes
resistant strains of HNPEK (HNPEK = h. influenzae, neisseria spp., proteus, e. coli, klebsiella)

(FYI - from E2) - List some of the (more common) 3rd generation cephalosporins:
two groups -
gp 1 - ceftriaxone (IV/IM), cefoxatime (IV/IM), cefdinir (PO), cefixime (PO)
gp 2 - ceftazidime, which lacks gram (+) activity but covers pseudomonas

Bacterial classification of Neisseria (n. meningitidis & gonorrhoeae)
(gram + or - ? Oxygen? Catalase/Oxidase?)
gram-negative diplococcus; aerobic; catalase and oxidase postitive
So if you’re treating - FYI but know logic of attachment

bacterial classification of listeria
gram positive non-spore forming rod
*remember that cephalosporins don’t cover listeria
-meningitis in neonates and >50 y/o’s (underlined in slides)

Classify pseudomonas aeruginosa
(gram + or - ? Oxygen? Catalase/Oxidase?)
gram (-) rod that is aerobic, oxidase positive & non-fermenting
List at least 2 drugs that BOTH cross the BBB and cover pseudomonas
ceftazidime (crosses BBB even when meninges inflamed)
cefipime
meropenem
Less preferred and alternative in bacterial meningitis:
aztreonam
FQ
meropenem
^^ doubt she will get this granular
(FYI - E2) Classify H. influenzae
(oxygen?)
gram negative coccobacillus that is a facultative anaerobe

(FYI - E2) What is the coverage of the aminopenicillins? (amp & amox)
Gram +
Strep & enterococcus
Enterococcus
Listeria
Gram −
H. influenzae
E. coli
Proteus mirabilis
Salmonella
Shigella
HEPSS + SEL
*most s.aureus is resistant if no B-lactamase inhibitor added

What is encephalitis?
inflammation of the brain
What is the most common cause of encephalitis?
HSV-1&2
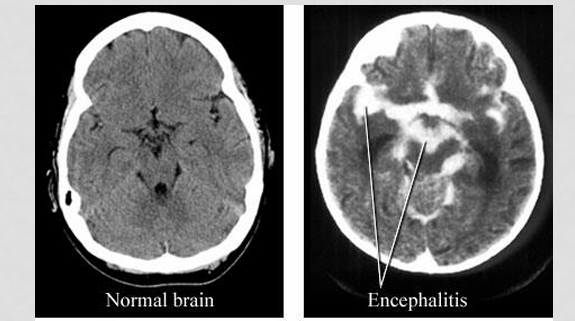
When encephalitis is suspected we usually do a lumbar puncture, viral testing, and radiologic imaging. What are some of the hallmark findings on an MRI that point towards a diagosis?
significant edema and hemorrhage within the temporal lobes
CSF findings change depending on the cause of meningitis (e.g., fungal, viral, bacterial).
Give the parameters for the following that are indicative of encephalitis:
Opening pressure (mm H2O) (pressure where LP needle enters spinal canal)
WBC
Protein
Glucose
Opening pressure - variable but rarely increased
WBC - 5-500
Protein - normal or slight increase
Glucose - normal
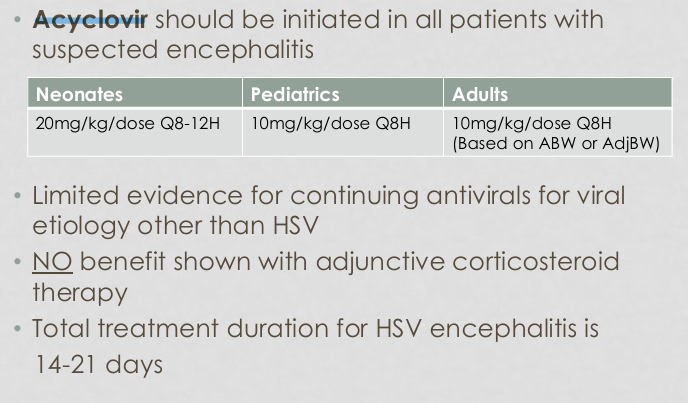
Which drug should be initiated in all patients with suspected encephalitis?
acyclovir
What are some of the ADRs on acyclovir? List at least three:
N/V
inc. LFTs
inc. BUN/SCr
neurotoxicity
injection site rxns
What are the warnings on acyclovir?
neurotoxicity and renal failure