CHP 19 HEART
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
The two divisions of the circulatory system
1) Pulmonary Circuit
right side of heart, smaller
carries blood TO the LUNGS
2) Systemic Circuit
left side of heart
oxygenated blood TO the TISSUES of the body
Simplistic flow of blood w/ left and right sides:
RIGHT SIDE
-oxygen poor blood arrives from inferior + superior venue cavae
-blood sent to lungs via pulmonary trunk
LEFT SIDE
-full oxygenated blood arrives from lungs via pulmonary veins (the one exception to vein/artery rule)
-blood sent to all organs via aorta
Blood Flow Through the Chambers (PROCESS)
1) Deoxygenated blood enters right atrium from superior + inferior venae cavae
2) through right atrioventricular valve into right ventricle
3) right ventricle contracts = pulmonary valve open
4) blood flows through pulmonary valve into pulmonary trunk
5) distributed by right + left pulmonary arteries to the lungs (LOAD UP O2)
6) blood returns from lungs via pulmonary veins to the left atrium
7) flows through left atrioventricular valve into left ventricle
8) left ventricle contracts (NOTE: same time as step 3) = aortic valve opens
9) blood flows through aortic valve into aorta
10) goes to every organ in the body (unload O2 LOAD UP CO2)
11) blood returns to right atrium via superior + inferior venae cavae
Ventricles contracting vs relaxing
relaxing = pressure drops, semilunar valves close, blood tries to back up into the ventricles, AV valves open, blood flows from atria to ventricles
Contract = blood tries to flow back into atria but AV valves close, pressure rises in ventricles, semilunar valves open and blood flows into ventricles
*Remember: blood wants to flow from high pressure to low pressure
Angina Pectoris
chest pain from partial obstruction of coronary (heart) blood flow
Myocardial infarction (MI)
sudden death of a patch of myocardium from long term obstruction of coronary circulation
HEART ATTACK
parts of a cardiac muscle
1) Cardiomyocytes = “branching tissue”
2) Intercalated disc = joins cardiomyocytes through junctions (allows for FAST electrical signals)
mechanical junctions = connecting cells through transmembrane proteins
Desmosomes = mechanical linkages that keep cardiomyocytes from being pulled apart from each other
electrical junctions (gap junctions) = allow ion flow between cells
Metabolism of Cardiac Muscle
-dependent on aerobic respiration to make ATP
-fatigue resistant; makes little use of anaerobic fermentation or oxygen debt mechanisms
what is the conduction system
coordinates the heartbeat
internal pacemaker
conduction system (PROCESS)
1) Sinoatrial (SA) node fires; initiates heartbeat and determines heart rate
2) signal spreads throughout atria
3) Atrioventricular (AV) node fires; electrical gateway to ventricles
Fibrous Skeleton; insulator that SLOWS DOWN the signal allowing for ventricles to have low pressure
4) signal spreads down Atrioventricular (AV) bundle (Bundle of His); right + left branches through interventricular septum toward apex
5) Subendothelial conducting networks (purkinje fibers) send signal through ventricular myocardium, then passing from cell to cell through gap junctions
systole
contraction
diastole
relaxation
sinus rhythm
normal heartbeat triggered by the SA node
typically 70-80 bpm
what nerves to what to heart rate
sympathetic nerves increase heart rate
parasympathetic nerves slow heart rate
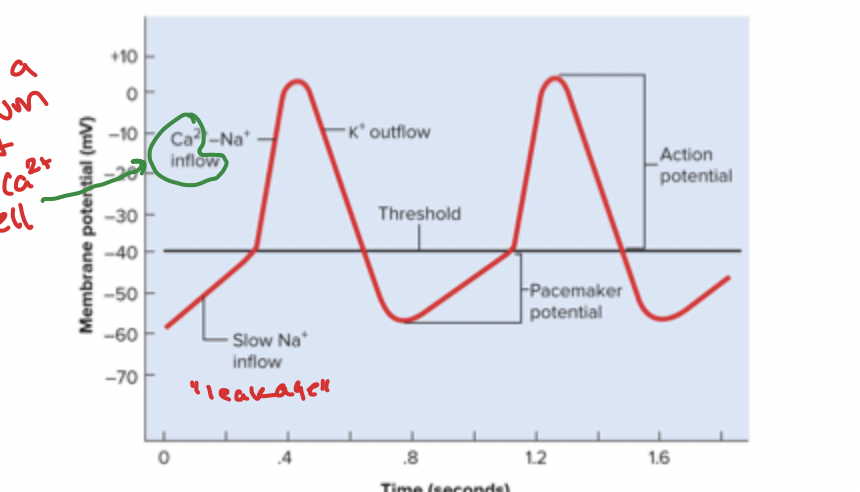
Pacemaker Physiology (PROCESS)
SETTING OFF HEARTBEAT
1) SA node starts negative, slow Na+ inflow = gradual depolarization = pacemaker potential
2)reaches threshold, BOOM, Ca2+ and Na+ channels open, cont. depolarization until 0mv reached
3) K+ channels open, K+ leaves = repolarization, pacemaker potential starts over
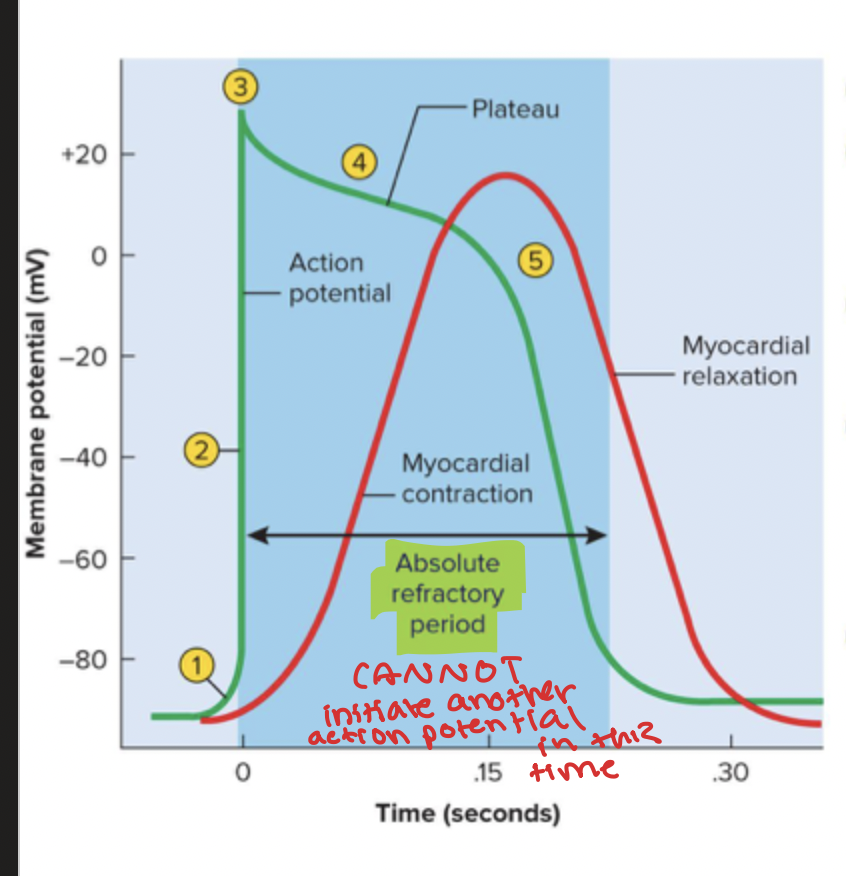
Typical Electrical Behavior of Myocardium (PROCESS)
1) Voltage gated Na+ channels open
2) Na+ inflow = depolarization, positive feedback cycle (RAPID)
3) Na+ channels close and positive voltage peaks
4) Ca2+ entering very slowly through channels creating a plateau, it is slightly down curved due to K+ leakage out
5) Ca2+ channels close, K+ channels open, rapid outflow = polarization back to resting potential
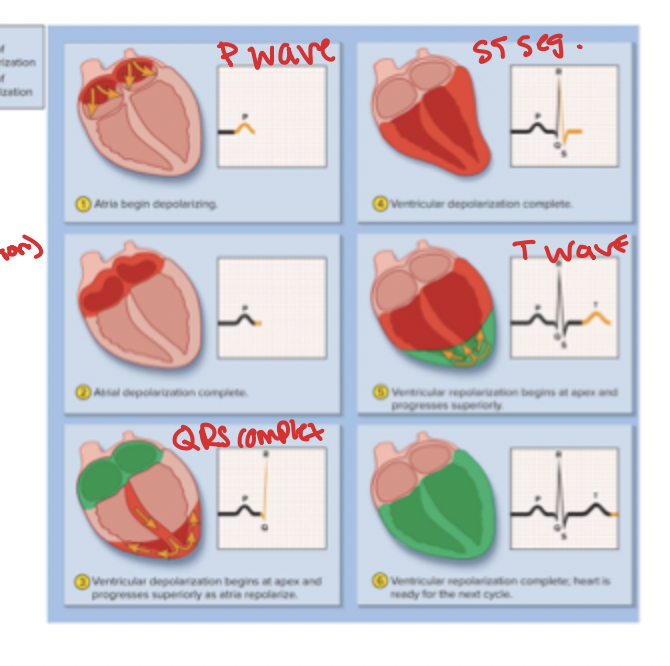
electrocardiogram (ECG or EKG)
composite of ALL action potentials
detected, amplified, and recorded by electrodes
Electrocardiogram (PROCESS)
1) P wave = SA node fires, atria depolarizes and contract cardiomyocytes
2) QRS complex = ventricular depolarization (contraction), spike!
3) ST segment = ventricular systole, the platue in myocardial action potential
4) T Wave = ventricular repolarization (relaxation)
Cardiac cycle
one complete contraction and relaxation of all four chambers of the heart
-only can happen w a pressure gradient (flow from high to low) and resistance
-pressure changes allow for opening and closing of valves
How do we measure blood pressure
sphygmomanometer (blood pressure cuff)
Auscultation
listening to sounds made by the body
The Heart Sounds
S1 = “lubb” louder and longer = closure of AV valves
S2 =”dupp” softer and shaper = closure of semilunar valves
S3 = rarely heard in people over 30 = opening of left AV valve and filling of left ventricle (blood whooshing)
Cardiac Cycle (PHASES)
1) Ventricular filling (during diastole/relaxation) = AV valves open, pressure drops, filling of ventricles from atrias
End-diastolic volume (EDV) = EQUAL blood filling
2) Isovolumetric Contraction (during systole/contraction) = ventricles contract but BLOOD STAYS
3) Ventricular ejection (during systole/contraction) = ventricles contract AND EJECT BLOOD
Stroke Volume (SV) = total amount after ejection (70 ml)
Ejection Fraction = ratio of blood ejected to blood leftover (54%)
End-Systolic Volume (ESV) = blood left over after ejection (EDV - SV)
4) Isovolumetric Relaxation (during diastole/relaxation) = tension goes down and the volume remains the same
Quiescent Period
when all four chambers are in distal (“quite time”)
Congestive Heart Failure
failure of either ventricle to eject blood effectively
Pulmonary Edema
left ventricle failure
fluid accumulates in pulmonary tissue
Systemic Edema
right ventricle failure
fluid accumulates in systemic tissue
Cardiac Output and how to calculate
amount ejected by each ventricle in one minuye
= heart rate * stroke volume (total amount after ejection)
about 4-6 L/min
cardiac reserve
the difference between a persons maximum and resting CO
Pulse
surge of pressure produced by heart beat that can be felt by palpating a superficial artery
smaller organisms have faster bpm
Tachycardia
resting heart rate above 100 bpm
bradycardia
rest heart rate less than 60 bpm
positive vs negative chronotropic agents
positive = raise heart rate
negative = lower heart rate
Cardiostimulatory effect vs cardio inhibitory effect
stim =some neurons in cardiac center transmit signals to the heart by sympathetic pathways
inhib = transmit parasympathetic signals by vagus nerve
Chronotopic effects of the atomic nervous system (PROCESS)
(lowering and rising heart rate)
SYMPATHETIC
1) postganglionic fibers are adrenergic and release norepinephrines
2) bind to B(beta)-adrenergic fibers in the heart
3) activate cAMP second messenger in cardiomyocytes
4) opening of Ca2+ channels in plasma membrane
5) inc Ca2+ inflow accelerates depolarization of SA node
6_ cAMP accelerates uptake of Ca2+, cardiomyocytes relax quicker
7) accelerating contraction and relaxation, heart rate increases as high as 230 bpm
PARASYMPATHETIC
1) vagus nerve has cholinergic inhibitory effects on SA and AV nodes
2_ acetylcholine binds to muscarinic receptors
3) opens K+ gates, inside is more negative = harder to initiate action potential
Vagal Tone
holds heart rate at 70-80 bpm at rest
Proprioceptors
in muscles and joints
sense changes in activity so HR increases before metabolic demands arise
Baroreceptors
sense changes in blood pressure
“lightheadedness” + correcting it
-BP dec = signal rate drops = inc heart rate
-BP inc = signal rate rises = dec heart rate
Chemoreceptors
sense blood pH, CO2, and O2 levels
Hypercapnia = high CO2 levels = inc heart rate for respiratory control
Hypoxemia = oxygen deficiency = slow down heart
Chemicals that affect heart rate
Autonomic neurotransmitters (NE and Ach)
Adrenal hormones (NE and epinephrine)
Nicotine
Thyroid hormone
Caffeine
impacts of electrolytes on heart rate
-K+ greatest chonotropic effect
Hyperkalemia = excess K+, heart rate slows + irregular
Hypokalemia = deficient in K+, needs stimulation
hyper vs hypo calcemia
hyper = excess of Ca+2, decreases heart rate
hypo = deficiency of Ca+2, increases heart rate
Preload
amount of tension in ventricular myocardium before it begins to contract
Frank-starling law of the heart
stroke volume is proportional to end diastolic volume
-more stretch (more blood in there) = harder contraction
Positive Inotropic Agents
-increase contractility
hypercalcemia
catecholamines (inc calcium levels)
glucagon
digitalis
negative inotropic agents
reduce contractility
hypocalcemia
hyperkalemia
vagus nerves (not too significant)
afterload
sum od all forces opposing ejection of blood from ventricle
-blood pressure in the aorta and pulmonary trunk
hypertension
increases afterload and opposes ventricular ejection
cor pulmonale
right ventricular failure due to obstructed pulmonary circulation
inc and dec cardiac output
-exercises increases cardiac output
-proprioceptors signal cardiac center, sympathetic output increases cardiac output
-increasing muscular activity increases preload and cardiac output
Ventricular hypertrophy effects
increases stroke volume, allows heart to beat more slowly at rest
Coronary Artery disease (CAD)
-a constriction of the coronary arteries
-Cause: usually from the degradation of material wall that obstructs the lumen (hole of artery)
-the the degradation becomes atherosclerotic plaques that build up and block the lumen
-risks: cholesterol, neutral fats, LIPIDS IN DA BLOOD
-unavoidable risks: heredity, aging, being male
-avoidable risks: obesity, smoke, lack of excesses
-impacts: angina pectoris, inflammation, artery spasms, artiniosclerrosis (hardening of blood vessel)
-fix it: coronary bypass surgery