Pediatric cancers
1/77
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
78 Terms
What is the leading disease-related cause of death in peds?
Cancer
Clinical trials for pediatric patients occur under what company?
Children’s Oncology Group (COG)
What percentage of pediatric patients are enrolled in clinical trials and why?
50% due to complicated nature of childhood cancers
What is the most common pediatric cancer overall?
Leukemia
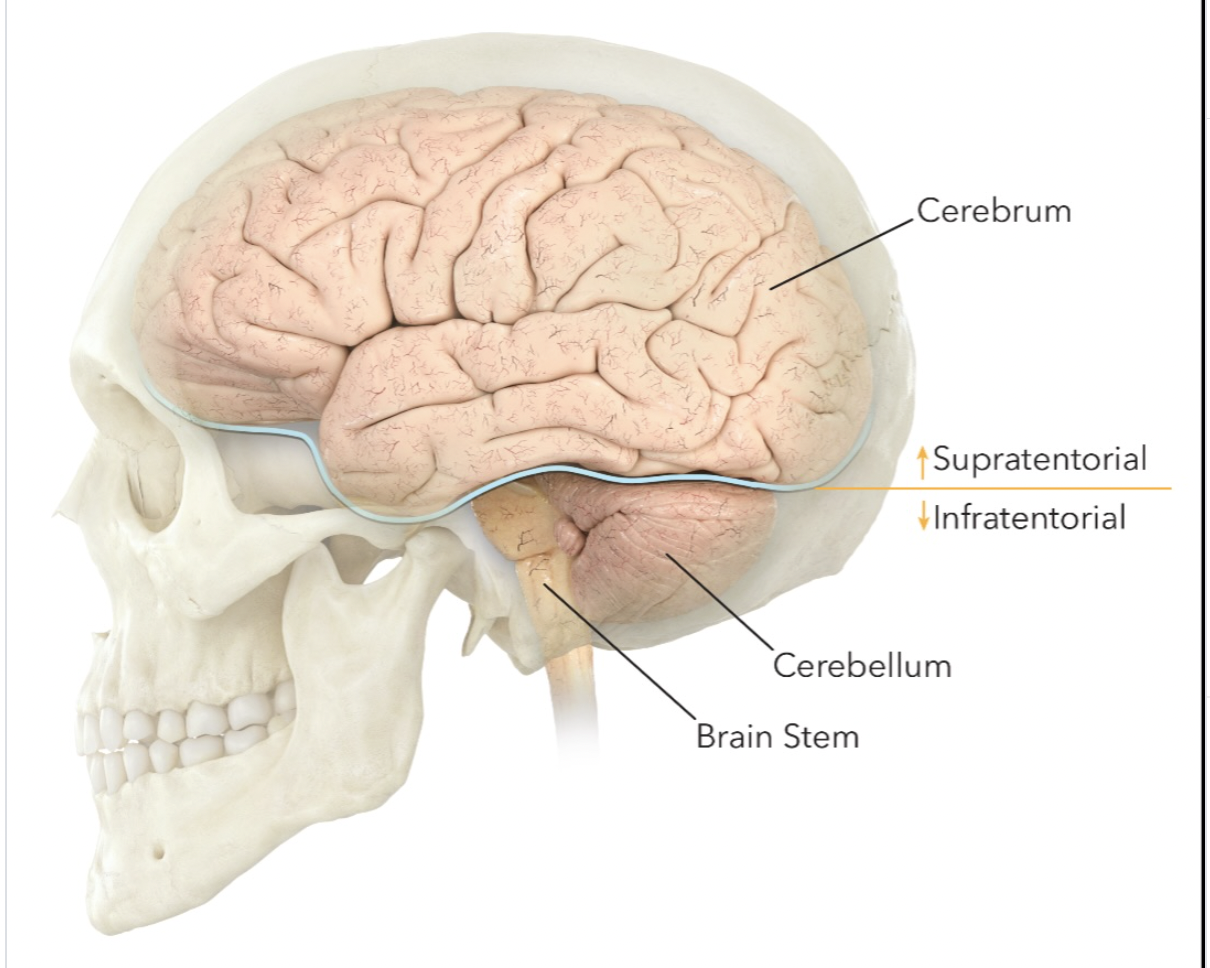
What is the most common solid pediatric cancer and site
CNS- brain being the most common site
Etiology agents for pediatric cancers
few know, mostly random or underlying genetic abnormalities
Main lines of treatment for pediatric cancers
Surgery first (if accessible), followed by chemo in very young patients to delay radiation
What is the biggest concern with radiation therapy for pediatric patients?
late side effects-especially secondary malignancy
3 Differences between pediatric and adult cancers
children are diagnosed with low grade vs high grade tumors located infratentorial (cerebellum & brainstem)
late side effects are a major concern that’s why radiation is delayed
surgery + chemo is the main treatments for peds; adults is surgery + radiation
8 Other childhood cancers not addressed in detail
Germ cell (gonads)
liver
leukemia
hodgkins lymphoma
nasopharynx
thyroid
keloid
Kaposi sarcoma
Pediatric brain tumors are most commonly located where?
infratentorially (cerebellum & brainstem)
What grade are pediatric brain tumors?
mostly are low grade, but can have high grade tumors
What are Astrocytoma?
star-shaped glial cells called astrocytes, arising from supporting cells in the CNS.
Glioblastoma multiforme is what stage of astrocytoma?
Stage IV astrocytoma (high grade)
6 Characteristics of low grade (I-II) tumors
slow, relentless growth
frequently in the cerebellum
present with long history of non-specific symptoms (headaches, seizures, visual/coordination issues, decreased school performance)
well circumcised and solid, often with a cystic component
treatment includes complete surgical resection and chemo; possible radiation
good prognosis
7 Characteristics of high grade (III-IV) tumors
highly malignant and aggressive
grow rapidly, invade, and destroy adjacent brain tissue
can spread through the CNS or distantly
rapidly progressing neurologic symptoms
irregular borders with areas of necrosis and surrounding edema
treatment include steroids to reduce symptoms, surgery, chemo, and RT
poor prognosis
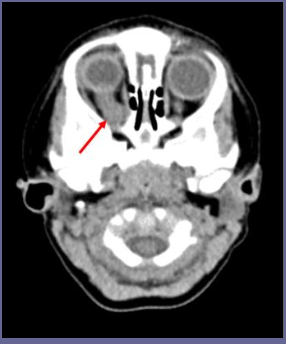
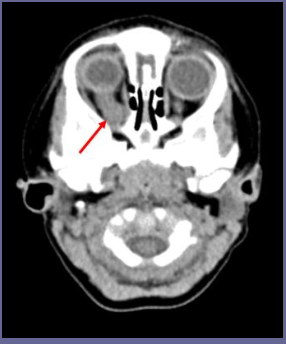
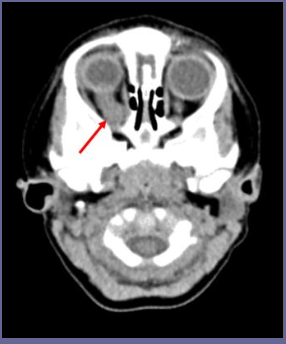
What is Optic glioma?
A low-grade and indolent (slow-growing/no symptoms) tumor of the optic nerve
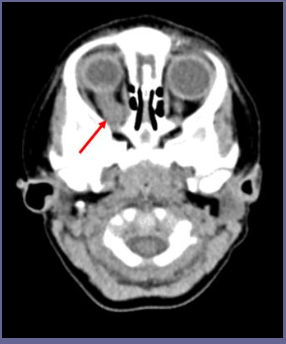
What is the most common presenting symptom for optic glioma?
visual disturbance
What is a significant risk of optic glioma?
neurofibromatosis (NF) genetic disorder
Treatments for optic glioma?
May watch and wait since it’s slow growing
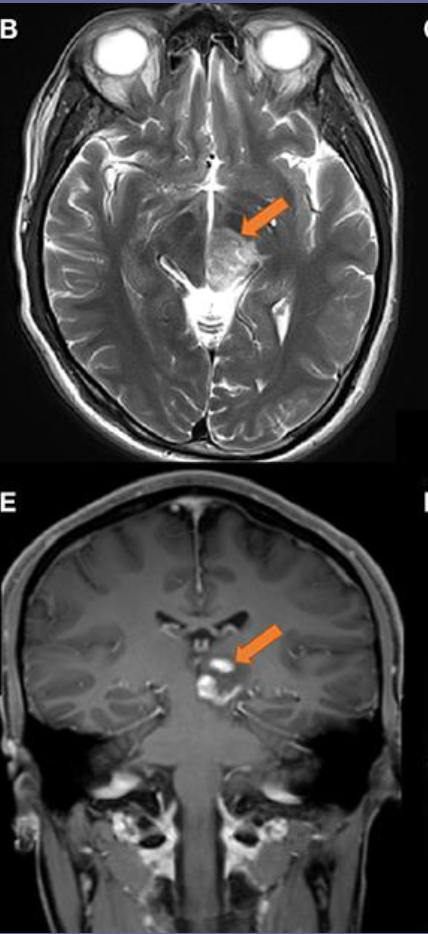
What is Ependymoma?
tumor that arises from cells that line the ventricles in the brain
Ependymoma is most commonly located where?
posterior fossa of brain
If cerebral spinal fluid (CSF) seeding occurs with Ependymoma , what treatment is necessary?
Craniospinal irradiation
What is medulloblastoma?
tumor that arises from primitive (highly undifferentiated) cells in the cerebellum (midline)
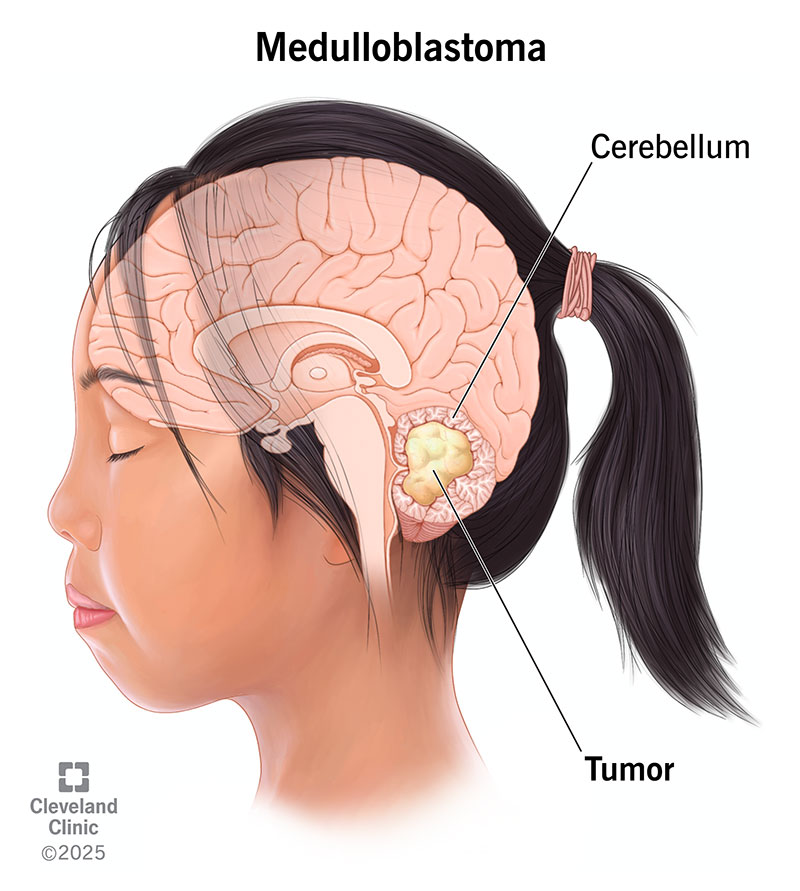
How does medulloblastoma grow?
fast-growing/malignant
4 Signs and symptoms of medulloblastoma?
speech difficulties
balance issues
hydrocephalus
early morning vomitting
What is hydrocephalus?
excessive CSF in ventricles, causing pressure and headaches
In Medulloblastoma, can CSF seeding occur?
Yes! its more common than other brain tumors
Where does medulloblastoma spread to (mets)?
bone
How is Medulloblastoma treated?
Surgery and adjuvant radiation therapy (CSI and boost to posterior fossa)
For Craniospinal irradiation, why may patients need to be anesthetized?
due to technical intricacies of treatment
Fields used for Craniospinal Irradiation?
opposed lateral whole brain fields that abut to 1 or 2 PA spine fields
Describe matching fields for Craniospinal Irradiation (3)
couch/collimator angled to create a straight edge of adjacent beams
skin gap: between spinal fields or brain/upper spine field to account for divergence
feathering technique
What is the feathering technique?
Technique in CSI that shifts the match line each day to eliminate overdosing to the spinal cord (hot spots) where both the divergent beams overlap
How is the patient positioned in CSI treatments?
Prone with chin extended (Aquaplast)
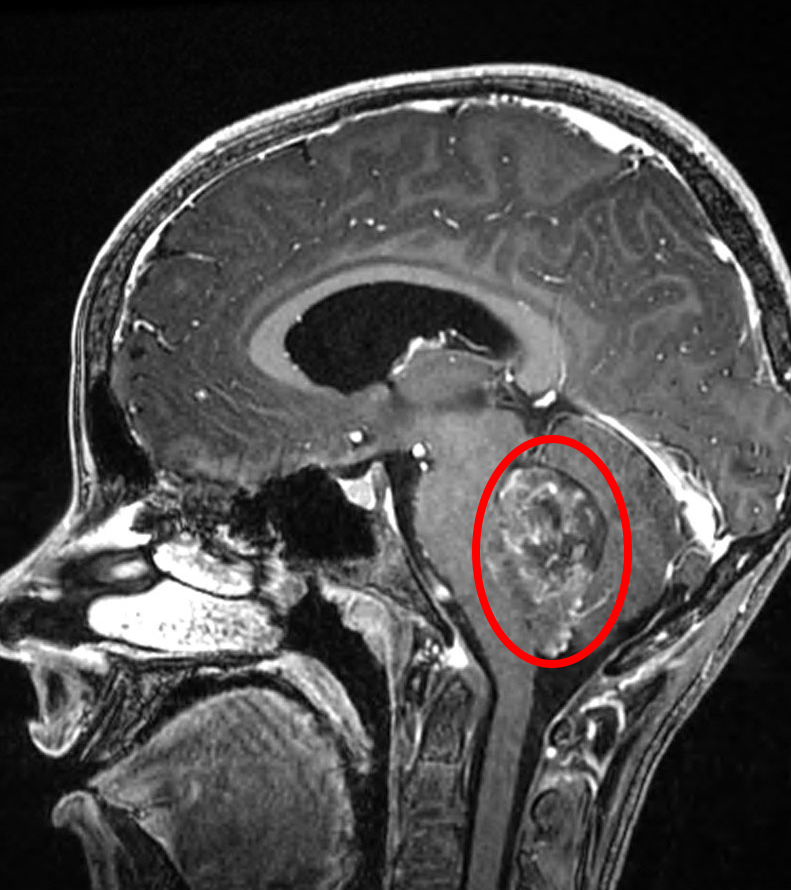
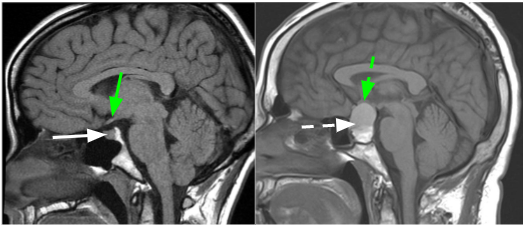
What is Brainstem Glioma and common location?
tumor that arises form glial cells in brainstem, typically pons
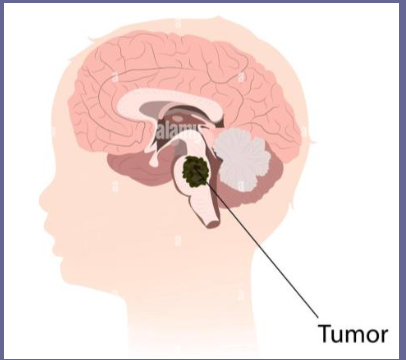
Brainstem Glioma cause what?
cranial nerve injury that affects:
vision
facial function
swallowing
What is the mortality rate and prognosis for Brainstem Glioma?
high mortality rate (90%)
poor prognosis
Mainstay treatment for Brainstem Glioma?
Radiation Therapy (surgery not indicated)
What are CNS germ cell tumors?
tumors that develop from embryonic nests of tissue in the midline brain
What is the most common histology for CNS germ cell tumors and its radiosentivity?
Germinomas
Very radiosensitive
What histology of CNS germ cell tumors is least radiosensitive?
nongerminomas
Treatment for CNS germ cell tumors?
CSI and primary tumor boost
4 Benign brain tumors
Pituitary adenoma
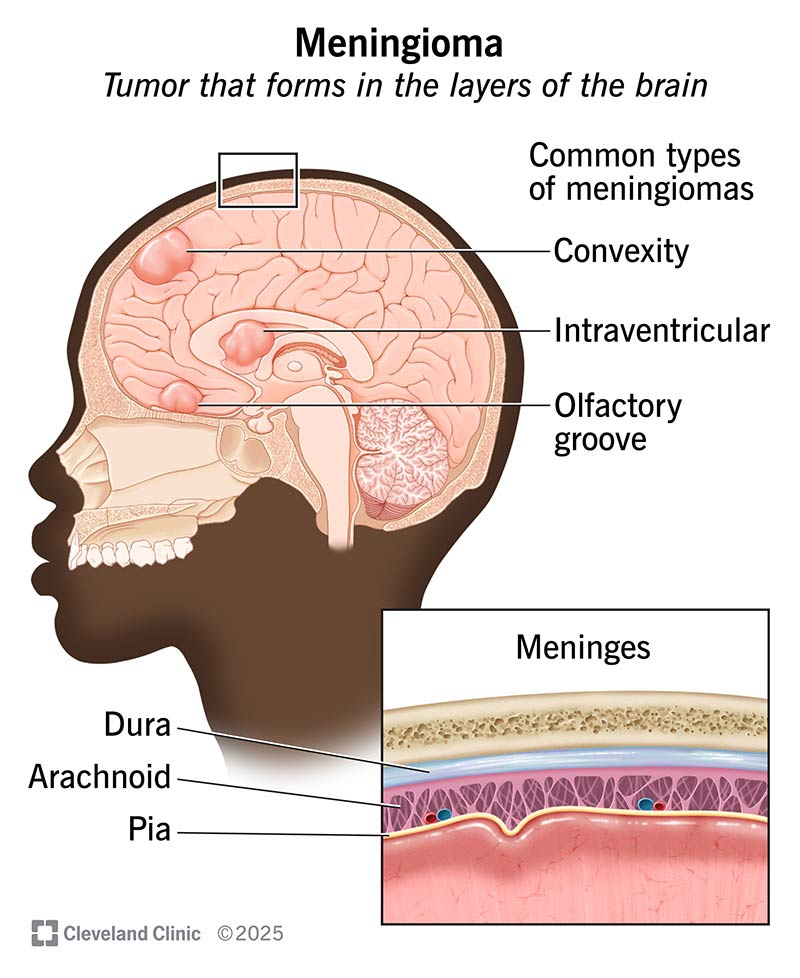
Meningioma
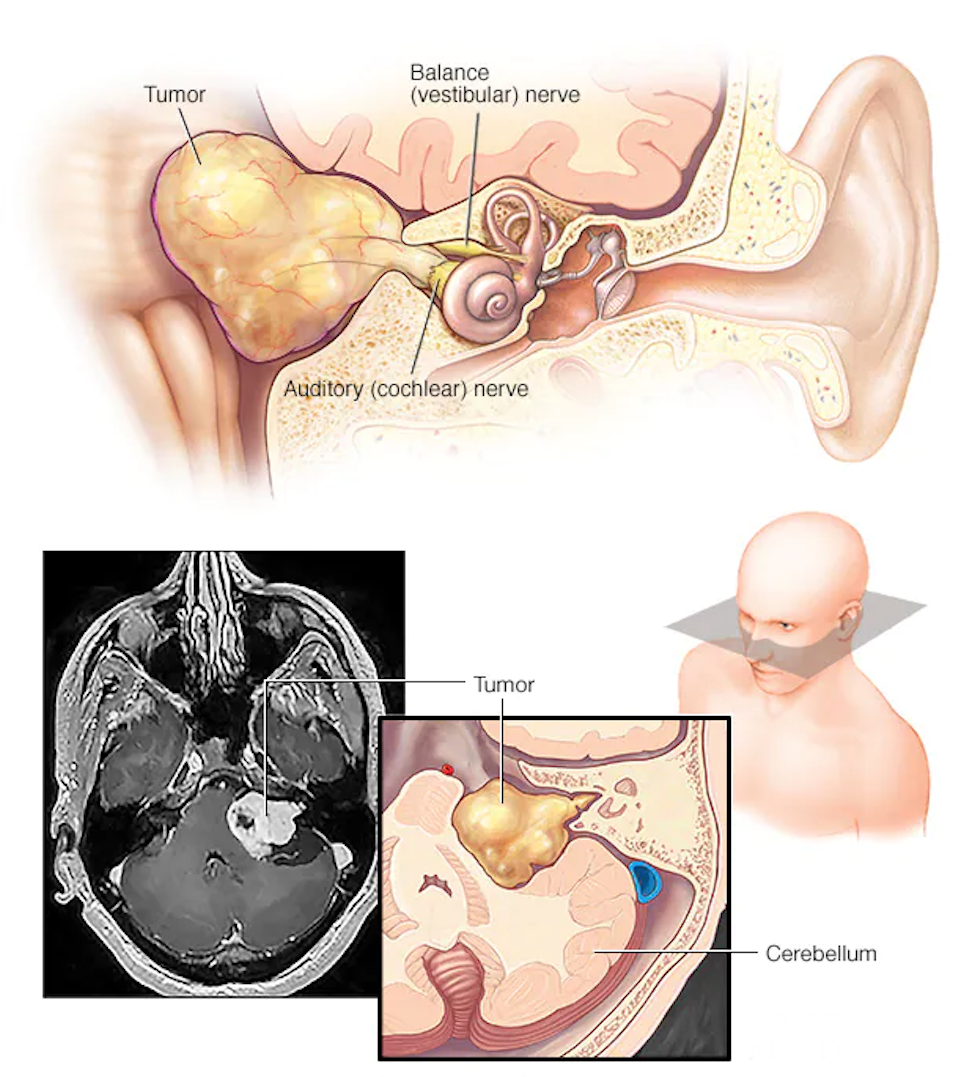
Acoustic neuroma
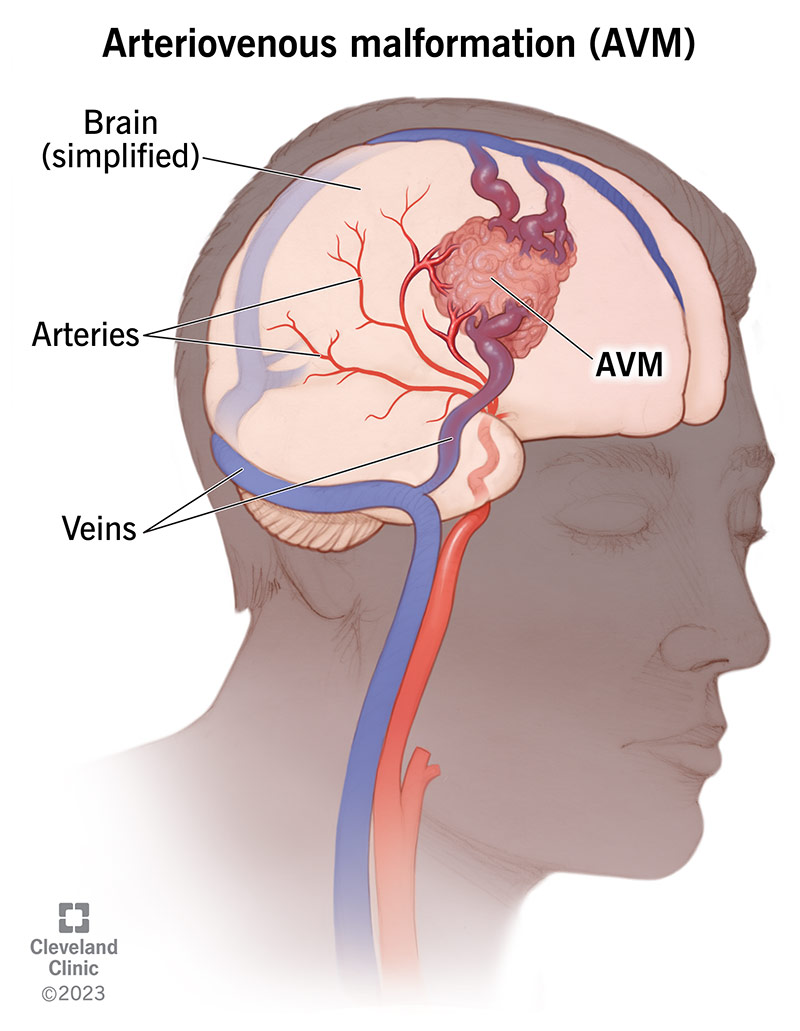
Arteriovenous malformation (AVM)
What does Pituitary adenoma cause?
excessive hormone production
What is Meningioma?
benign tumor of the meninges
What is Acoustic neuroma?
benign tumor of the main nerve from the inner ear to the brain
What is Arteriovenous malformation (AVM)?
tangled blood vessels in the brain
What is Retinoblastoma (2)?
primitive neuroectodermal tumor (PNET) that develops in the retina
recessive genetic defect; both alleles of the RBI gene must be mutated
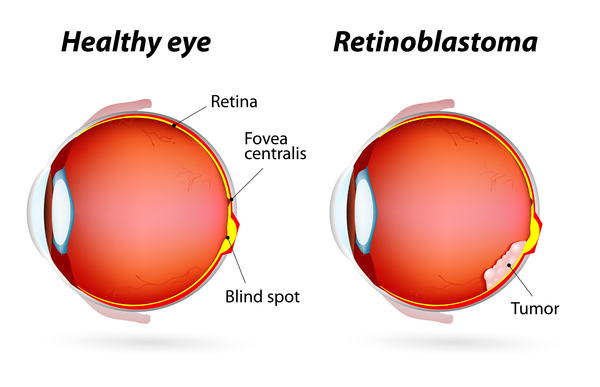
What is the “ cat’s eye reflex” associated with Retinoblastoma?
a reflex where the pupil of the eye appears white instead of red in photographs, with camera flash or light, due to the tumor reflecting from the retina.

Treatment for Retinoblastoma
if bilateral/inoperable, radiation is indicated (organ sparing) to preserve vision
Retinoblastoma is associated with what cure rate?
High cure rate
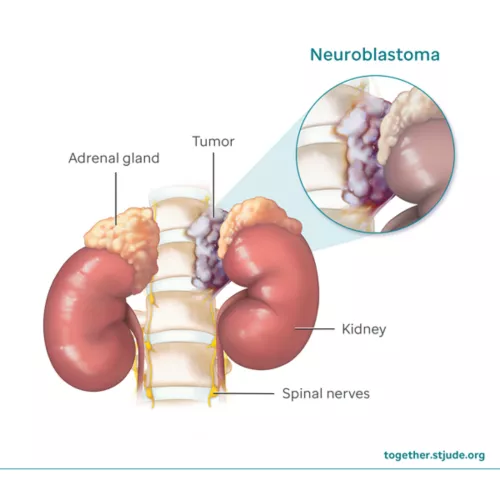
What is Neuroblastoma and where is it located?
cancer of neuroblasts (immature nerve cells)
can be found anywhere, but typically in the adrenal glands
Neuroblastoma is associated with what?
spontaneous regression
What is spontaneous regression?
where the cancer becomes benign (which is why the # of cases are low)
What population does Neuroblastoma occur in?
very young peds (infants)
Neuroblastoma is associated with what type of genetic mutation?
N-myc gene mutation (oncogene)
2 Signs and symptoms associated with Neuroblastoma?
abdominal mass
very ill looking (most have mets @ diagnosis)
Staging system for Neuroblastoma
International neuroblastoma staging system (INSS)
In Neuroblastoma, most patients fall into what catergory?
“high-risk” category associated with poor prognosis
What is Wilms tumor?
malignant tumor of the kidney (one/both)
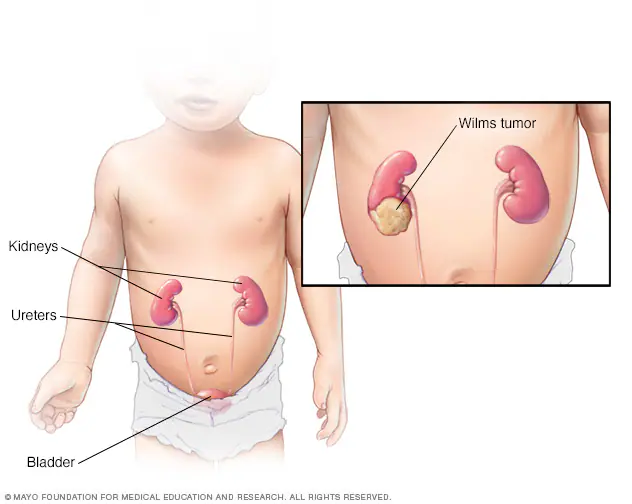
What is another name for Wilms tumor?
nephroblastoma
Median age of occurance for Wilms tumor?
ages 3-4 years old
Signs and symptoms of Wilms tumor?
typically painless abdominal mass
patients typically don’t appear ill looking
How does Wilms tumor grow?
grows rapidly and tends to rupture into abdomen
Common site for mets with Wilms tumor?
Lung
3 Unfavorable histologies for Wilms tumor?
Anaplastic
Clear cell sarcoma
Rhabdoid tumor (poor prognosis)
*excellent prognosis for other histologies*
Staging system for Wilms tumor?
National Wilms Tumor Study Group (NWTS) staging system
3 Treatments for Wilms tumor
nephrectomy
chemo
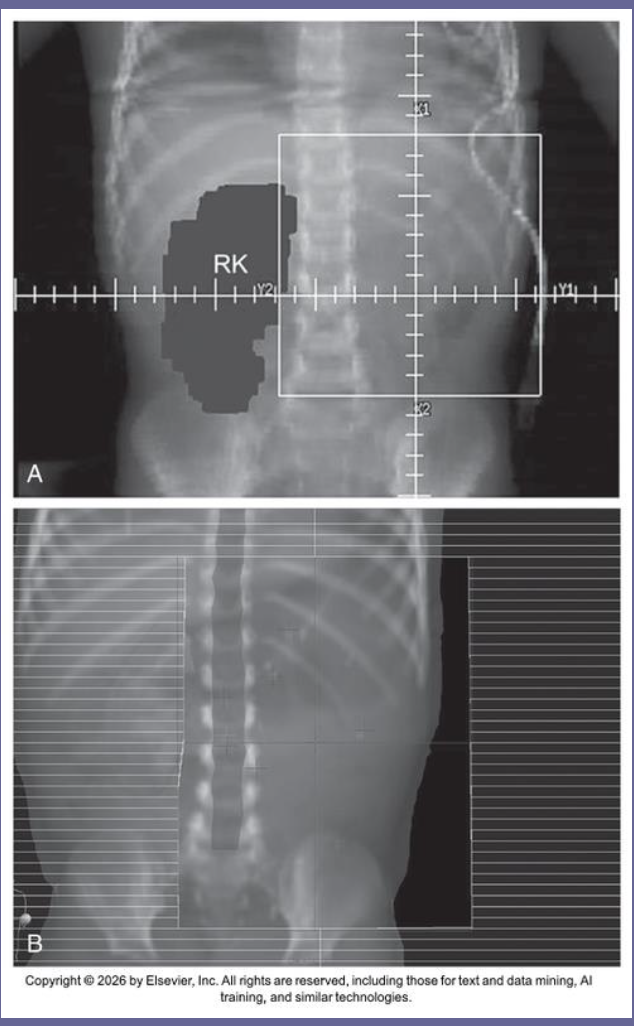
radiation (3D conformal with MLCs to block healthy kidney)
What are Soft Tissue Sarcomas?
tumors arising from mesenchymal (connective) tissue with WIDE variety of histologies

Most common histology for Soft Tissue Sarcomas?
Rhabdomyosarcoma
What is Rhabdomyosarcoma?
cancer of striated muscle, typically affecting the orbit of the eye

Most common presenting symptom of Soft Tissue Sarcomas
painless lump or swelling in tissues of the body
2 Treatments for Soft Tissue Sarcomas?
Chemo
radiation (not typically surgery)
Prognosis for Soft Tissue Sarcomas
Excellent if there’s no metastatic disease
2 Staging systems for Soft Tissue Sarcomas
Rhabdomyosarcoma study group (IRSG)
tumor, grade, node, histologies, metastasis (TGNM)
5 ways that a Radiation therapist must modify workflow with pediatric patients
Therapists have to be understanding of the patient’s needs and work with the patient’s caregivers.
can modify the workflow to accommodate the patient's needs, including scheduling longer appointments if necessary.
Therapists have to work with the anesthesia team to sedate the patient before they can be positioned.
Documentation of treatment setups, daily doses, and quality assurance needs to be done precisely
Adhere to protocol guidelines, especially for clinical trials
9 Late effects of radiation therapy
fibrosis of irradiated tissues
decreased bone development/asymmetric growth
impaired function of critical organs (lung, liver, kidney etc)
musculoskeletal abnormalities (pain, stiffness, reduced mobility)
impaired breast development (irradiation to chest in females)
cognitive (IQ)/behavioral deficits
endocrine dysfunction (stunted growth)
permanent hair loss
secondary malignancies