Peripheral Vascular Disease
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
Peripheral Vascular Disease
Diseases of the blood vessels (arteries and veins) located outside the heart and brain
Causes of PVD
-Flow problem
-Damage or obstruction
-arteries: thrombus, plaque, trauma, Atherosclerosis most common cause
-Veins: thrombus, incompetent valves
-Pump problems: RHF or LHF
-Lymph problems: Cancer surgery, rafiation
Peripheral Artery Disease: Atherosclerosis
-most common chronic arterial disorder
-Deposit of fat and fibrin obstructs and hardens arteries
-5 P’s: Pulses, pain, pale, paresthesia, paralysis
-Most common cause of amputations
PVD: Risk factors and prevalence
-Risk factors: HTN, family history, metabolic syndrome, DM, african-american, smoking, hyperlipidemia
-Prevalence: older than 70, younger 50-69→ related to smoking
Assessment- Skin appearance
-Mottled appearance
-Dependent rudor
-Weak or no pulses, may need a doppler
-cold or numb toes, brittle nails, necrotic tissues

Assessment- Pain
-Intermittent claudication
-Pain when walking because the muscles need more oxygen, destructed in vessels, ischemia, when they sit down the pain will go away
-Early symptom
Assessment- Blood Flow
-Capillary refill- may be longer
-Pulses: may need doppler to find
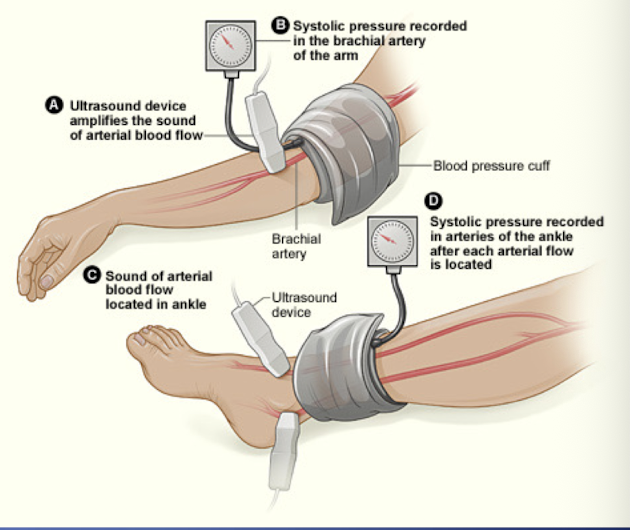
Ankle Brachial index
-Average ankle pressure/ average arm pressure
>1.4: non-compressible calcification of vessel→ refer to vascular specialist
-1.0-1.4: normal, no blockage→ no treatment
-0.9-1.0: borderline→ your ABI is slightly lower than normal but not low enough to diagnose PAD
-0.8-0.99: mild arterial disease→ treat risk factors
-0.5-0.79: moderate blockage→ refer to vascular specialist
-<0.5: severe blockage→ refer to vascular specialist
Peripheral Arterial Disease- management
-Reduce risk factors
-Smoking cessation→ EBP: reduced progression and risk of amputation
-Lipid lowering diet→ EBP: regression, less claudication
-Disease Management program: Diabetes control, HTN control
-Promote circulation/vasodilation
-EBP= walking regimen decreased symptoms greater than angioplasty→ goal: 50 minutes/ 3x week
-EBP= anti-platelet agent: Aspirin (1st choice), Plavix, Pletal, Trental
-Promote circulation to lower extremities→ do not criss legs, position limbs dependently, keep extremities warm
Treatment for PAD
-walking
-Arterial stents
-Bypass vessels
-Amputation
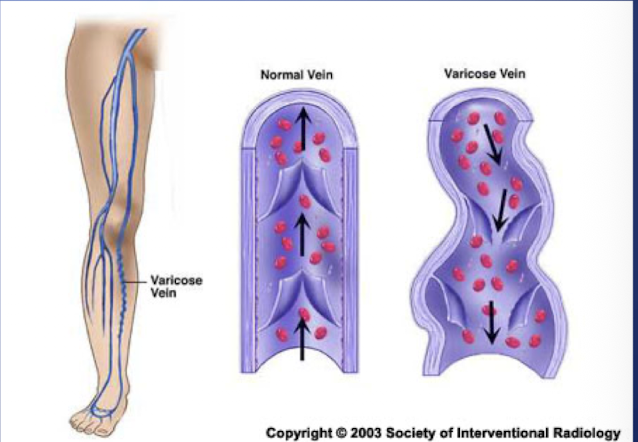
Varicose Veins
-Irregular torturous veins
-Usually effects veins of lower extremities (saphenous veins)
-Caused by long standing increased venous pressure
-Veins valves become incompetent
Varicose Veins- Incidence and risk factors
-Nursings at high risks
-Age
-occupations with long periods of standing
-family history
-Caucasians
-pregnancy
-increase with older adults
Varicose Veins- Manifestations
-Dilated veins
-Aching
-leg fatigue
-itching
-feelings of heat
-thin discolored skin above the ankle
Varicose Vein- treatment
-Conservative
Compression stockings (augment muscle pumping action of legs), leg elevation, exercise
-Ablation therapy
-Sclerotherapy
-Vein stripping
Vein Ablation
-Laser or radio frequency
-Heated catheter creates scare tissue and causes vein to close
-treats varicose veins and chronic venous insufficiency

Chronic Venous Insufficiency
-Inadequate venous return over a period of time
-Valve injury, can’t prevent back flow
Symptoms: pain described as aching or heavy, edema, altered pigmentation, dilated superficial veins, and stasis dermatitis, brownish discoloration of the skin if RBC leaking into tissue surrounding veins
Venous stasis ulcer
-Common complication of CVI
-Comprise 50%-70% of leg ulcers
The lymphatic system
-essential for fluid balance in the body
-Removes macromolecules too large for reabsorption into circulatory system
-Lymphedema occurs when there is damage or destruction of the lymphatic pathway
-Primary Lymphedema
-Secondary Lymphedema
Lymphedema
-Chronic debilitating disease
-Requires lifelong management
-If untreated can progress causing:
Continued proliferation of fibrotic tissue
increase in size of infected limb
chronic infections
-Results in an increase in functional impairment and a decrease in quality of life

Lymphedema- treatment
-Complete decongestive therapy
-Standard treatment for management of lympedema
-Manual lymph drainage
-Bandaging
-Exercise
-Skin and nail care
-Instruction in self care
Lymphedema- Home care to prevent injury
-Inspect daily for problems: changes in temp, appearance, edema
-Wash and moisturize feet daily
-Between toes, mild soap, lukewarm water
-rinse, pat dry versus rub dry
-Apply moisturizer (avoid excess)
-Do not apply moisturizer between toes
-Prevent injury: trim nails, always wear socks and shoes, protect feet from hot and cold, choose well fitting shoes
-Promote circulation: avoid crossing legs, regular walking, stop smoking
-Educate regarding when to contact HCP: any skin breakdown, redness, or pain
Lymphedema- Surgery
-Lymphaticovenular Bypass
-Microscopic surgery
-Lymphatic fluid is redirected to drain through small veins
Deep Vein Thrombosis (DVT)
-The formation of blood clots in the deep veins of an extremity
-Can originate in any extremity
-80% originate in deep veins of calf
-Most common complication of surgery and immobility
Venous Thromboembolism (DVT/PE)
-Increased risk for surgical patient without DVT prophylaxis
-Pulmonary embolism major complication
-Roughly 1 out of 10 hospital deaths are related to blood clots in the lungs
-Blood clots may remain in the vein or dislodge and travel to the lungs causing pulmonary embolism
DVT- Who is at risk
-Hospitalized, immobile
-Surgery→ 20% increase, 50% increase for orthopedic surgery
-Obesity
-Smokers
-Oral contraceptives
-Central venous catheters
DVT assessment
-Symptoms of affected extremity
Dull, aching pain, tenderness, warmth, erythema
Edema (increase in extremity circumference)
-May be asymptomatic
-Pulmonary emboli may be the first sign
DVT- management
-Prophylaxis→ early ambulation, sequential compression devices, compression stockings
-Vast number of RCT prove that primary prophylaxis can reduce the incidence of DVTs
-Medications: LMWH, Heparin
DVT- Diagnosis
-Duplex venous ultrasonography: measure the velocity of flow in veins
-D-Dimer: Lab test, a compound formed after thrombin converts fibrinogen to fibrin, negative result use to rule out presence of a blood clot
Treatment for venous thromboembolism
-Anticoagulants= 1 of 3 most dangerous classes of meds associated with adverse events
-Heparin
-Warfarin (coumadin)
-Complex management during: Prescribing, administering, monitoring, Pt education, reversal and recognition of complications
PTT or Anti-Xa
-Partial Thromboplastin Time
-drawn frequently, every 2-6 hours as per nomogram
-All values are drawn STAT
-pt must achieve 2 consecutive therapeutic PTTs or Anti-Xa to be able to then draw PTT or Anti-Xa once daily
Anti-Xa
-Test that measures anti-thrombin activated factor Xa levels in plasma
-Levels of factor Xa inhibition can help calculate heparin concentration present in blood sample
-Less factors that interfere with Anti-Xa levels compared to PTT
-Therapeutic range: 0.3-0.7 IU/mL
-Therapeutic range can vary according to indication for heparin therapy
Management of IV heparin therapy (DVT)
-Baseline PT/PTT, Anti-Xa, H/H, and Platelet count required before therapy is initiated
-Platelet count and H/H QD
-Assess for HIT (heparin-induced thrombocytopenia)→ report Plt count: <150,000 or a 30-50% reduction
-Assess for signs of bleeding: stool guiac, hematuria
-Reversal agent: Protamine Sulfate
Management of Warfarin (DVT)
-given simultaneously with heparin until Warfarin is therapeutic and then heparin is discontinued
-Should be given same time every day
-Usually on for 3-5 months
-INR monitored frequently, range is 2-3 usually
-Pt education essential → safety
-Dietary instruction
-Reversal agent: Vitamin K
-Do not take any OTC meds or herbal supplements without consulting MD first
-Wear medical alert bracelet
-NO smoking or alcohol
-Obtain blood work as ordered
-Take precautions to avoid bleeding
-Report to ED for episode of bleeding
Factor Xa inhibitors- Anticoagulants
-Rivaroxiban, Apixaban
-Does not effect platelet aggregation
-Short half life so can discontinue 2 days before surgery and resume 6-10 hours post surgery
-Interacts with many meds and OTC herbals
-Contraindicated in renal impairment (CrCl <30ml/min) and hepatic impairment
Surgery for Venous Thromboembolism
-Inferior vena cava filter→ catch blood clots from going into the lungs, done if they can’t take anticoagulant therapy
-Thrombectomy
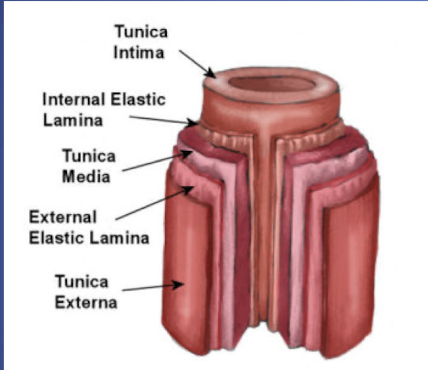
Layers of Artery
-Tunica Intima
-Tunica Media
-Tunica Externa
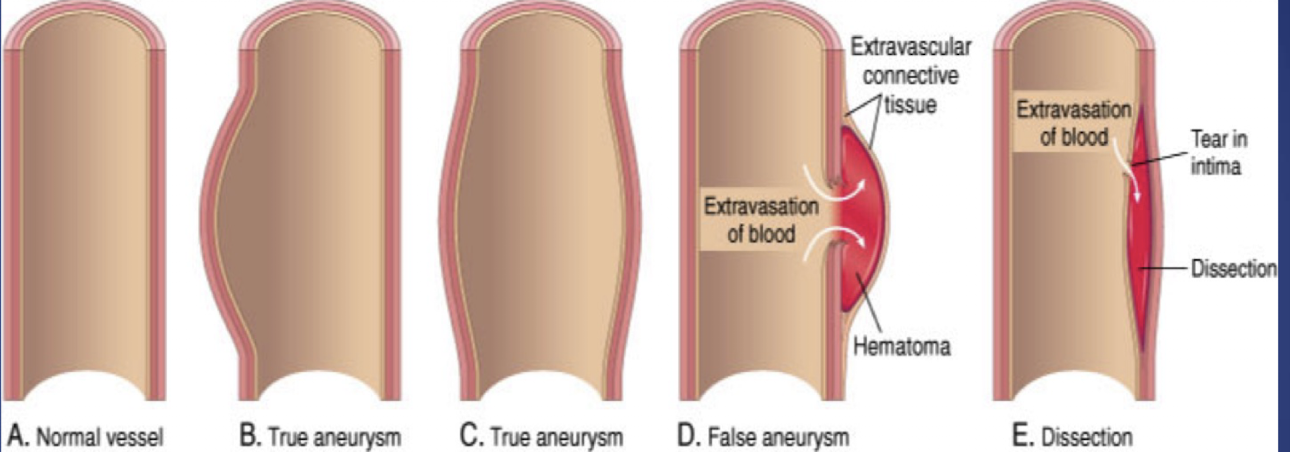
Thoracic and Abdominal Artery Aneurysms
-Localized dilation of aorta
-Common causes: atherosclerosis, HTN
-Types:
-True: saccular, fusiform
-False: dissecting
-Can involve aortic arch, thoracic aorta, and abdominal aorta
Thoracic and Abdominal Aneurysms- At risk
-Male, 6th or 7th decade, increase BP, atherosclerosis, smoker
-Increase in size means increase in risk of rupture
-Subjective data: depends on location, size, growth
Thoracic and Abdominal Aneurysms- diagnosis
-Angiogram
-Chest X-ray
-Echocardiogram
-Computed Tomography (CT)
-Magnetic resonance imaging (MRI)
Abdominal Artery Aneurysms
-If asymptomatic: aggressive BP control, serial imaging, surgery when >= 5.5 cm
-Surgical management
-Two types
-Endovascular grafting (EVSG) or Endovascular Aneurysm repair (EVAR)
-Open approach
-Mortality: Less then 5% for elective and 40% for emergent
Abdominal Artery Aneurysms- Nursing management
-Pt teaching: surveillance
-Unexplained back, chest, flank pain
-Falling BP or hematocrit
-Smoking cessation
Postoperative: monitor vital signs (BP WNL), assess peripheral pulses, assess bleeding, pain, fever; avoid coughing, sneezing, vomiting
-Do not want to put on any increased pressure
Aortic Dissection
-Life-threatening emergency if Type A
-Tear in the tunica intima of the aorta
-Hemorrhage into tunica media
-Splits the vessel wall, forming a blood filled area between the 2 layers
-HTN accounts for 70% of dissections
-Sudden severe excruciating (tearing or ripping) pain located in the back and/or chest
-Other symptoms include: syncope, dyspnea, hypotension, absent peripheral pulses
-If major arteries effected: ischemia or effect to major organs
Type A Aortic Disseciton
-Emergent surgery
-High risk for life threatening complications
-Only contraindication for surgery is if presence of comorbidities impact survival to one year or less
Type B Aortic Dissection
-Surgery reserved for development of complications related to dissection
-If uncomplicated generally manage medically
-More for abdominal aneurisms
-Medical management
-BP control
-Imaging surveillance