Pharm content before finals
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
Antibiotics examples
sulfanamides, penicilins, cephalosporins, mecrolideas, tetracyclines,
microbial infection
microorganisms exist in external and internal environments, can be helpful or harmful,
host defences
physical barriers- skin, gastric acid
immune factors- antibodies,
phagocytic cells- macrophages and neutrophils
major microbe classes
bacteria, viruses, fungi and protazoa
bacteria
bacteria grouped by morphology- take different shapes, or gram stain- positive or negative
difference in gram stain influences choice of antibiotic
gram positive
thick cell wall with a thick outer capsule
gram negative
complex cell wall with a thin outer capsule and 2 cell membranes, more difficult to treat
infection
when host defences are compromised- person becomes susceptible to infection, microorganisms invade and multiply overwhelming body’s defences,
s+s : fever, chills, sweating, redness, pain, swelling, fatigue, weight loss, increased WBC, pus
types of infection
community acquired infection vs healthcare associated infection
HAIs
more than 48hrs after admission, top 10 causes of death in Canada (70% are preventable), more difficult to treat as microorganisms are more drug resistant and virulent, ex- MRSA and VRE
disinfectant
kills organisms, used on non living objects (bleach, hydrogen peroxide based cleaners, disinfecting sprays)
antiseptics
inhibits growth of microorganisms on living tissues (hydrogen peroxide, chlorhexidine, ABHR, iodine, alcohol)
principles of antibiotic therapy
clinical judgement and knowledge of microbial and pharmaceutical factors
therapeutic response- signs and symptoms of infection improve
subtherapeutic response- signs and symptoms of infection do not improve
superinfection- can occur when antibiotics reduce or eliminate normal bacterial flora needed for normal function, when good bacteria is killed, other bacteria may take over and cause infection (C.diff, yeast infection)
3 general uses of antibiotics
empiric therapy, definitive therapy, prophylactic or preventative therapy
empiric therapy
for life threatening or sever complication is high and best kills the microorganisms known to be most common causes of infection, broad spectrum- before administering, specimens are obtained from suspected areas of infection to be cultured and specific causitive organism is identified
definitive therapy
once blood culture returns, antibiotic choice tailored to treat specific organism that grew
prophylactic therapy
prior to procedure when likelihood of microbial contamination is high
factors influencing prescription of antibiotics
resistance over use- over prescribing of antibiotics
food-drug and drug-drug interactions
host factors
age
allergies
kidney and liver functions
pregnancy
genetics
sit of infection
host defences
antibiotics classifictation
sulfanamides, penicilins, cephalosporins, carbapenems, macroliodes, quinolines, aminoglycosides, and tetracyclines
characteristics of antibiotics
antibacterial spectrum, mechanism of action, potency, toxicity and pharmacokinetic properties
mechanism of actions of antibiotics
interference with bacterial cell wall synthesis
interference with protein synthesis
interference with DNA and RNA replication
disrupts metabolic reactions within bacterial cells
bacteriacidal
kills bacteria
bacteriostatic
inhibits growth of susceptible bacteria, instead of immediate killing- leads to bacterial death
sulfanomids
often combined with another antibiotics, ex- sulfamethoxazole (often combined with trimethoprim as Bactrin, Septra)
MOA- bacteriostatic- preventing bacterial synthesis of folic acid
Indications- resp tract infections, prophylaxis and treatment of pneumonia associated with HIV, UTIs and MRSA
C- allergy, chem related drugs, pregnancy or nursing, children less than 2 months
AE- hematologica: agranulocytosis, aplastic anemia, thrombocytopenia
—- GI: nausea, vomiting, diarrhea, pancreatitis, hepatotoxicity
—- Integ: toxic epidermal necrolysis, exfoliative dermatitis, stevens- johnson sydrome, photosensitivity
— other: convulsions, crystalluria, toxic nephrosis, headache, peripheral neuritis, urticaria
Interactions- may potentiate the hypoglycemic effects in diabetes, toxic effects of phenytoin, anticoagulant effects of warfarin sodium and cyclosporine-induced nephrotoxicity
Beta-lactam antibiotics
broad spectrum, share common structure and MOA, 4 major subclasses:
penicillin
cephalosporins
carbapenams
monobactams
Penicillins (beta lactam antibiotic)
bacteriacidal, kills gram positive and negative (broad spectrum)
MOA- penicillin molecules slide through bacterial cell walls and death results from lysis of bacterial cells
Indications- prevention and treatment of infections caused by susceptible bacteria, pneumonia, intra abdominal infections, sepsis (piperacillin/tazobactam)
C- allergy (not all names end in cillin), many med errors when drugs are called by trade names
AE- CNS: lethargy, anxiety, depression, seizures
— GI: nausea, vomiting, diarrhea, taste elterations, oral candidasis
— Hematological: anemia, bone marrow depression, granulocytopenia
— metabolic: hyperkalemia, hypernatremia, alkalosis
— other: pruritus, hives, rash
interaction: aminoglycosides, methotrexate, NSAIDs, oral contraceptives, probenecid, rifampin, warfarin sodium
cephalosporins (beta lactam antibiotic)
first, second, third, fourth and fifth (not availble in canada) generations
AE- diarrhea, abdominal cramps, rash, pruritus, redness, edema, cross sensitivity with penicilins if allergy exists
*most cephalosporins start with cef, ceph or kef, ex: cefazolin (Ancef), cephalexin (keflex), cefuroxime, ceftriaxone
Carbapenems (beta lactam antibiotic)
bacteriacidal, broadest antibacterial action of any antibiotics, acutely ill- compicated body cavity and connective tissue, must be infused over 60 minutes, may cause drug induced seuzure activity, reduced risk by proper dosing management
ex- imipenem, meropenem, ertapenem
Macrolides
3 types: azithromycin, clarithromycin, erythromycin
MOA- bacteriostatic until high enough conc., wide range of infections (upper and lower resp tract, skin and soft tissues
Indications- strep infections, mild to moderate upper and lower resp tract infections (haemophilus influenza), spirochetal infections treated with erthyromycin and other macrolides (syphilis, lyme disease), gonorrhea, clamydia, mycoplasma
AE- cardiovascular: palpations, chest pain, QT prolongation
— CNS: headache, dizziness, vertigo
— GI: nausea, hepatotoxicity, heartburn, vomiting, diarrhea, flatulency, cholestatic jaundice, anorexia, abdonmal taste
— Integ: rash, uritcaria, phlebitis at IV site
other: hearing loss, tinnitus
Interactiosn- highly protein bound and are metabolised in liver- delayed metabolic clearance of interacting drugs and/or cause toxic drug effect, reduces efficacy of oral contraceptives, prolong QT interval
Tetracyclines
bacteriostatic (inhibits protein synthesis), natural and semisynthetic- effective against many resistant bacteria, ex- tetracycline, doxycycline, minocycline
MOA- inhibit growth and kill wide range of Riskettsia, Chlamydia and Mycoplasma organisms as well as a variety of gram negativs and positive bacteria
indications- complicated infection, intraabdominal infection and community acquired pneumona (more listed)
C- allergy, pregnant or nursing, children under 8
AE- discoloured teeth and tooth enamel in fetus and children, stunt fetal skelaton development, photosensitivity, diarrhea or vaginal candidiasis, reversible bulging fontanelles, thrombocytopenia, coagulation irregularieis, hemolytic anemia, excasberation of systemic lupus erthematosus, gi upset, enterocolitis and maculopapular rash
interactions- if taken with antacids, antidiarrheals, dairy, calcium, enteral feedings or iron preperations- reduces absorption of tetracylcine, potentiate effects of oral anticoagulants, antagonise effects of bacterial antibiotics and oral contraceptives, increased BUN (blood urea nitrogen)
nursing process for antibiotics
thorough pt history, age, weight, baseline vitals, lab tests, cultures before antibiotic therapy, medication list, check name of med, take antibiotics as prescribed and right time for right length, watch of signs and symptoms of superinfections, common AE with antibiotics: nausea, vomiting, diarrhea
aminoglycosides define + types
gentamicin, tobramycin, amikacin (first three are most common) streptomycin sulfate, paramomycin sulfate, neomycin sulfate
group of natural and semisynthetic drugs, not given orally bc of poor absorption, potent, serious toxicities, bacteriacidal- prevents protien synthesis (bind to ribosome), kill mostly gram neg and some gram pos, given with beta lactams for peak effect (beta lactams go first)
aminoglycosides- therapeutic drug monitoring
treatment of systemic infections, serum levels monitored, maximise drug efficacy/minimise risk of toxicity, toxicities: nephrotoxicity and ototoxicity, dosing adjusted to kidney function (creatine clearance)
MIC- mean inhibitory concentration, measure of lowest conc of a drug needed to kill a standard amt of bacteria
Peak- highest drug level (once daily regime usually for this drug) (measured 30 minutes after drug given)
Trough- lowest drug level to ensure adequate renal clearance of drug to avoid toxicity (30 mins before next dose)
***therapeutic goal is trough conc at or below 1mcg/mL - considered undetectable, trough levels above 2mcg/mL is associated with greater nephro/oto toxicity
aminoglycosides indications
gram neg bacteria- pseudomonas spp, escherichia coli, proteus spp, klebsiella spp, serratia spp, often used with other antibiotics for synergistic effects, gram pos infections resistant to other antibiotics- enterococcus spp, S aureus and bacterial endocarditis (streptococcal)
aminoglycosides contraindications, AE, interactions
contraindications: allergy, pregnancy (cross placenta and can cause deafness), pass in breastmilk, caution in neonates bc of immaturity of kidneys in newborns can cause greater risk for toxicities
Adverse effects: nephrotoxicity (reversible) or ototoxicity (not reversible, also effects balance), headache, parathesia, vertigo, skin rash, fever, overgrowth of non susceptible organisms, neuromuscular paralysis (very rare and reversible), hypersensitivity reactions
interactions: use in caution with other nephrotoxic drugs, use with loop diuretics may increase risk of ototoxicity, kills normal flora that produces vitamin k- increased bleeding time with warfarin
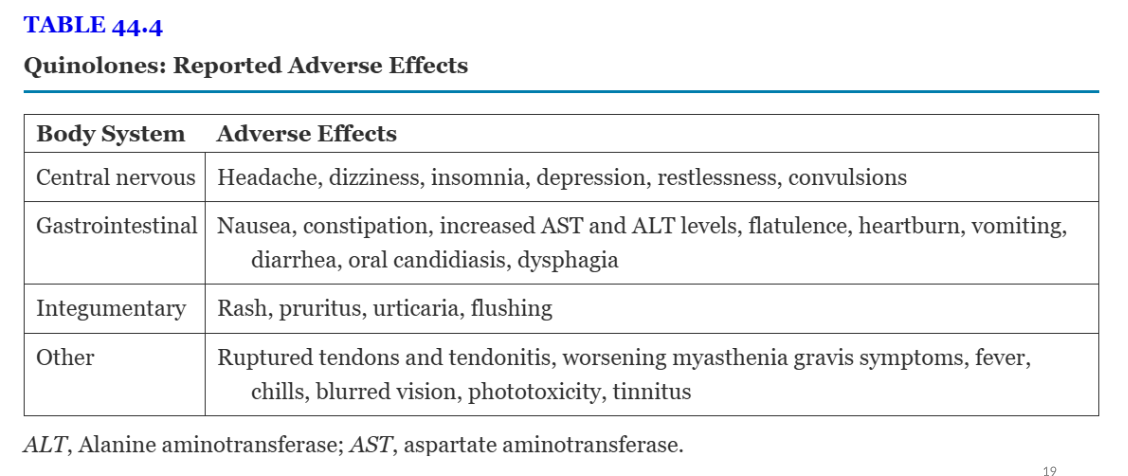
quinolones define + examples
norfloxacin hydrochloride, ciproflaxacin, levoflaxacin (most common), moxifloxacin hydrochloride
also called fluoroquinolones, excellent oral absorption except for norflaxacin, effective against most gram neg and some gram pos
quinolones mechanism of actions and indications
MOA- bacteriacidal, affects DNA production (NOT human dna), used to treat s aureus, serratia marcescens, and myobacterium fortutinum,
bacterial resistance: pseudomonas aeruginosa, s aureus, pneumococcus spp, enterococcus spp, enterobacterial family
indications- complicated urinary tract, respiratory, bone and joint, GI, skin infections. ciproflacxacin and levoflaxacin are taken oral or injection, norfloxacin has limited oral absorption but oral used in genitourinary infections
quinolones interactions, adverse effects
interactions: decreased absorption of antibiotic- antacids, calcium, magnesium, iron, zin prepartions, sulcrafate, dairy products, enteral tube feedings, nitrofurantoin, increased absorption: probenecid, oral anticoagulants (warfarin) (atleast 1 hours before and 2 hours after all interacting meds)
AE- qt prolongation, label warning- increased risk of tendonitis and tendon rupture, worsening symptoms of muscle weakness and breathing dificulties in pts with myasthenia gravis, seuzures reported, slow infusion to reduce venous irritation
where to check for drug info in hospital before given
IV drug manual
lexicomp
clindamycin
semisynthetic, bacteriacidal OR bacteriostatic, inhibits protein synthesis, neg/pos bacteria and anaerobic bacteria,
indications- chronic bone infections, genitourinary infections, intra abdominal infections, other serious infections, pseudomembranous colitis (C diff), neuromuscular blocking drugs- may enhance neuromuscular drugs (preoperative and critical care)
linezolid
new class: oxazolidinones, works by inhibiting bacterial protein synthesis, excellent oral absorption (for home),
indications: vancomycin resistant enterococci bacteria, pneumonia, complication skin infections, MRSA, gram pos infants and children
AE: headache, nausea, diarrhea, vomiting, decrease platelet count
interactions: strengthens effects of vasorepressive drugs (prohypertensive), antidepressants- selective serotonin reuptake inhibitors, tyramine containing foods
metronidazole
MOA- interferes with microbial DNA synthesis
indications- anaerobic organisms, intra abdominal and gynelogical infections, protozoal infection (trichomoniases, amebiases), treats antibiotic associated colitis (orally), given to children with C diff, not reccomended for first trimester of pregnancy
AE- dizziness, headache, GI discomfort, nasal congestion, reversible neutropenia and thrombocytopenia
Interactions- avoid alcohol for 30 FINISHHHHH
nitrofurantonin
MOA- disrupts bacterial cell wall formation,
indications- primarily used for UTIs (E coli, S aureus, klebsiella spp, enterobacter spp)
AE- gi discomfort, dizziness, headache, skin reactions, blood dyscrasias, ECG changes, possible irreversible peripheral neuropathy and hepatotoxicity (rare but fatal)
FINISH
Vancomycin hydrochloride
MOA- bacterial antibiotic, cell wall synthesis inhibition
indications- gram pos, MRSA, oral vancomycin for c diff, must monitor blood levels to ensure therapeutic levels and prevent toxicity (trough level 10-20 mcg/mL)
AE- ototoxicity and nephrotoxicity, RED MAN syndrome- dlushing, itching of head, nech face, upper trunk, hypotension muscle spasm and dyspnea- caused by rapid infusion (infuse over 60 minutes)
nursing implications for for antibiotics
history of allergies and comorbidity (hepatic, kidney and cardiac function) and drugs, obtain culture before antibiotic therapy, instruct pt to take antibiotics as prescribed, assess of signs and symptoms of superinfection, check for name of med (look alike and sound alike)