Trauma second Quiz (copy)
1/98
Earn XP
Description and Tags
6
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
99 Terms
Trauma alters coordination between what key brain regions?
Amygdala Rapid
Hippocampus
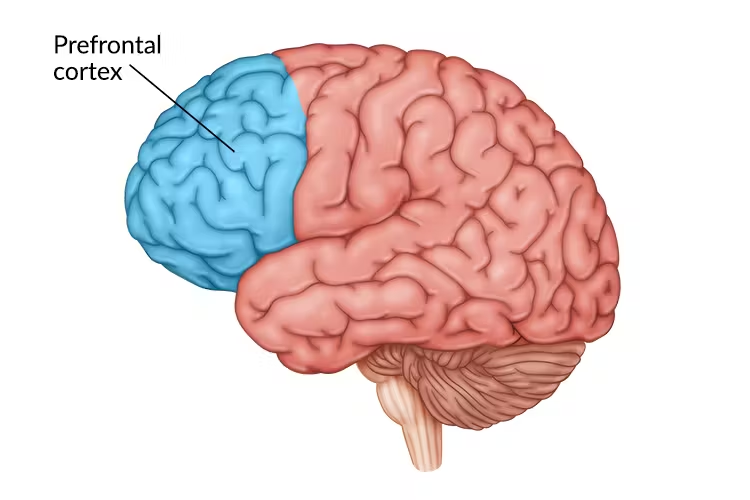
Prefrontal Cortex (mPFC, dlPFC)
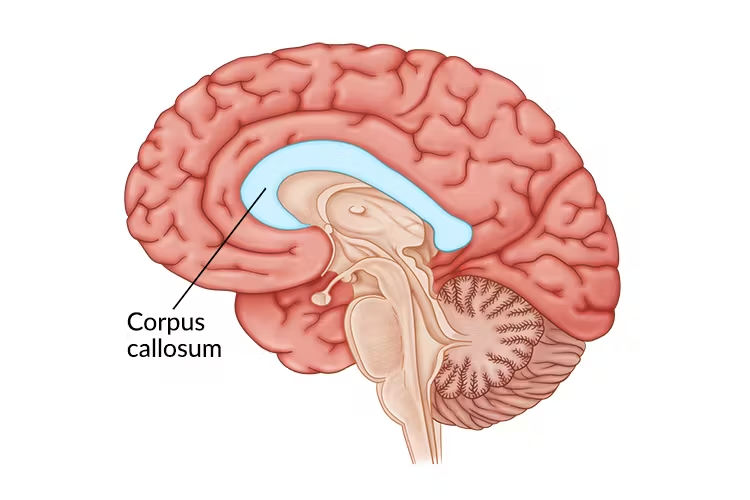
Corpus Callosum
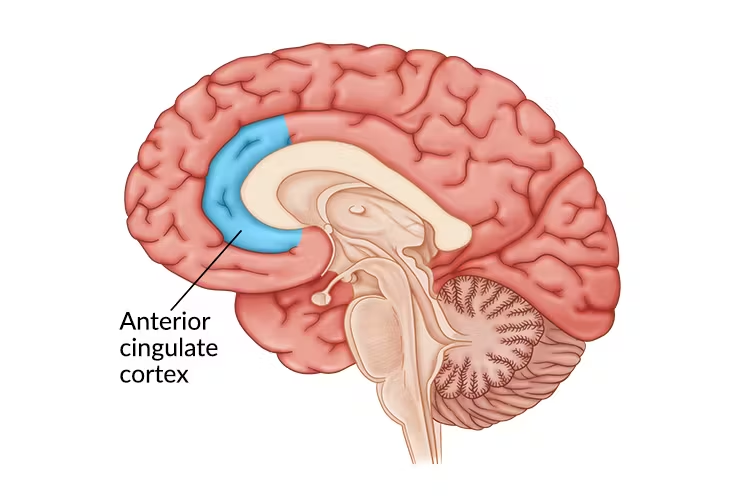
Anterior Cingulate Cortex (ACC)
Amygdala roles
Rapid threat detection
Hyperactivation → persistent fear responses
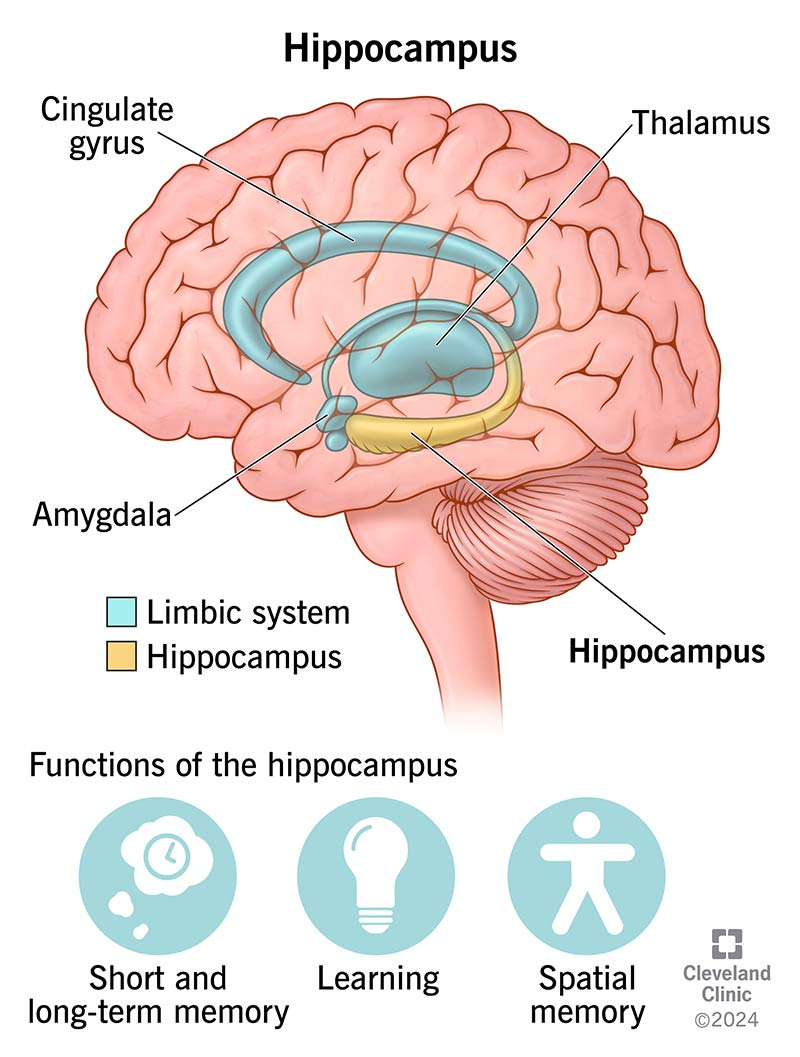
Roles of hippocampus
Contextual and temporal memory integration
Impaired contextualization → fragmented, “timeless” memories

Role of Prefontal Cortex- what happens in trauma
Top-down emotional regulation
Reduced inhibition of limbic activation
Role of Corpus Callosum
Integration between left (verbal/narrative) and right (emotional/sensory) processing
Role of Anterior Cingulate Cortex (ACC)
Conflict monitoring and emotional regulation
Trauma causes damage to single structures- true or false?
False. Trauma involves altered coordination across large-scale brain networks
Brain networks affected by trauma
Salience Network:
○ Detects threat and prioritizes survival-relevant stimuli
○ Associated with hypervigilance and threat biasDefault Mode Network (DMN)
○ Involved in self-referential processing and autobiographical memory
○ Altered functioning linked to rumination and changes in self-conceptExecutive Control Network (ECN)
○ Supports cognitive control and emotional regulation
○ Reduced top-down modulation of limbic reactivity in traum
Clinical Illustration of Sofia, her background and what she experienced
Sofia, a 30-year-old, grew up in an emotionally invalidating environment. Her caregivers were critical, emotionally distant, and unpredictable.
What are two outcomes which are The Body’s Physiological Response to Trauma
Stress Hormones: Cortisol and Adrenaline
○ Activation of the hypothalamic–pituitary–adrenal (HPA) axis during threat.
○ Adrenaline (epinephrine): Rapid mobilization of energy, increased heart rate, and alertness.
○ Cortisol: Sustains the stress response by increasing glucose availability and suppressing non-essential functions.Chronic Dysregulation
○ Prolonged or repeated activation leads to allostatic load.
○ Associated with cardiovascular disease, immune dysregulation, metabolic changes, and mood disturbances
What is The Role of the Autonomic Nervous System?
The Autonomic Nervous System (ANS)
regulates automatic survival responses and
works in close interaction with the HPA axis. It continuously scans for cues of threat and safety.
Two main branches of ANS
Sympathetic Nervous System (SNS):
• Mobilizes the body for action. Associated with fight or flight responses.
• Increases: ○ heart rate
○ blood pressure
○ respiration
○ muscle readiness.Parasympathetic Nervous System (PNS):
• Supports: ○ recovery
○ rest
○ restoration.
• Promotes: ○ digestion
○ immune function
○ energy conservation.
• Enables calming and return to baseline after stress
Two complexes in polyvagal theory
Ventral Vagal Complex (VVC):
• Supports:
○ social engagement,
○ emotional regulation
○ calm states.
• Associated with feelings of:
○ safety
○ connection
○ presence.
Dorsal Vagal Complex (DVC):
• Associated with shutdown and immobilization responses under extreme threat.
• May manifest as:
○ dissociation
○ emotional numbin
○ collapse
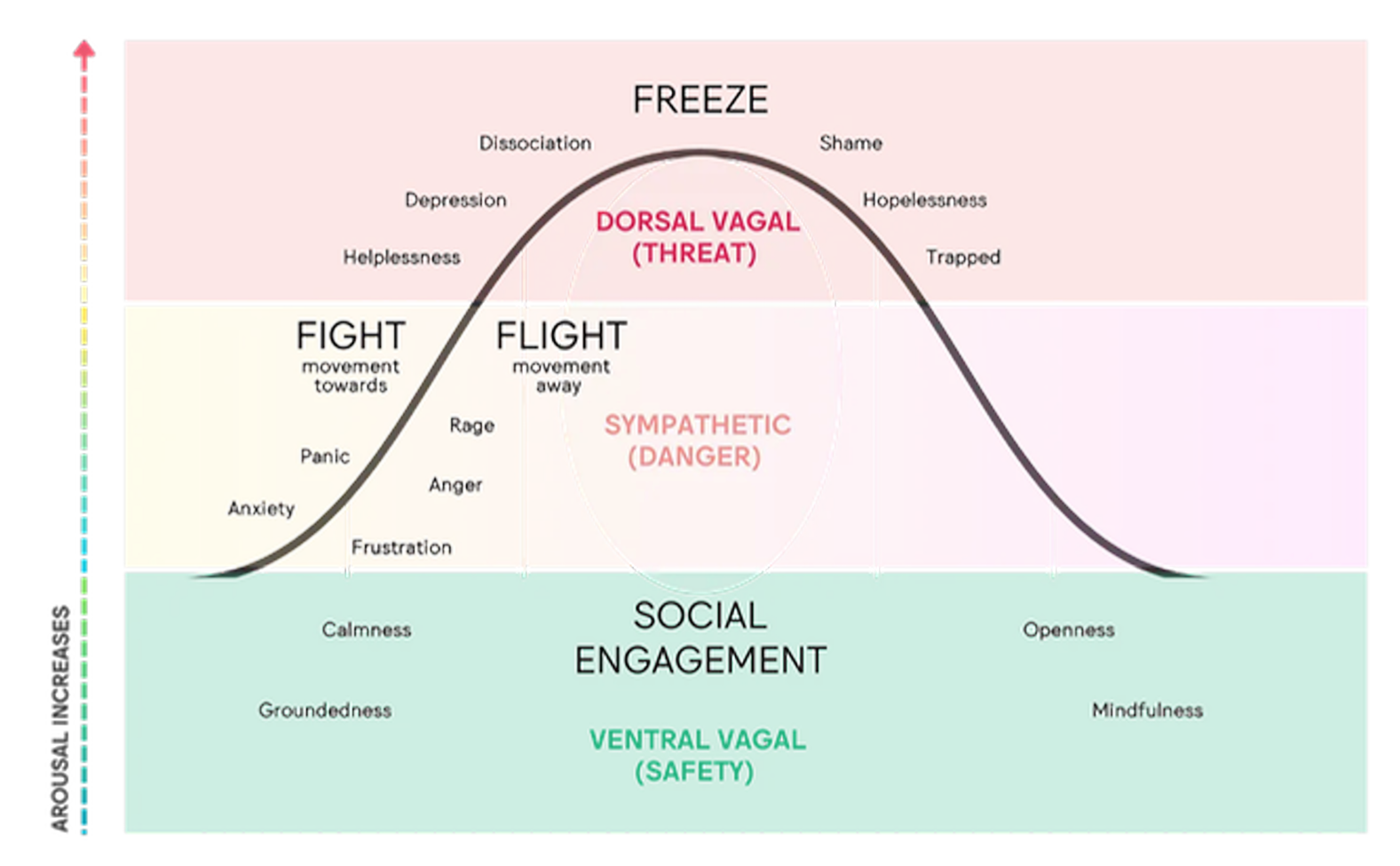
Levels of Polyvagal theory
Ventral Vagal
Sympathetic (danger)
Dorsal vagal (threat)
Definition of resilience
Resilience is the capacity of the nervous system and the person to adapt, regulate, and reorganize after adversity
what does resilience involve?
Autonomic flexibility
Capacity to return to regulation after activation
Integration of difficult experiences
Relational safety and co-regulation
Meaning-making over time
Is resilience= absence of distress?
No. it is the ability to recover and continue functioning despite it
What is the Window of tolerance?
The Window of Tolerance is the emotional zone where a person can function effectively and feel regulated, safe, and in control.
two dysregulated states outside this window of tolerance:
⬆ Hyperarousal – too activated
Anxiety, overwhelm
Fight/flight urges
Physiological activation (shaking, hyperventilating)
⬇ Hypoarousal – too shut down
Numbness, low energy
Disconnection or zoning out
Lack of motivation
Causes for the window of tolerance to shrink/expand
shrink: stress, trauma, poor sleep, illness
expand: self-care, mindfulness, therapy, social support, movement.
who invented the window of tolerance t
Daniel J. Siegel
Working Therapeutically with the Window of Tolerance- Steps
1. Assessment:
Identify triggers of hyperarousal and hypoarousal
Observe autonomic patterns
Map the client’s typical regulatory range
2. Stabilization
Grounding and orientation exercises
Breath regulation
Somatic awareness
Resource installation (EMDR Phase 2)
Co-regulation in the therapeutic relationship
3. Titration
Gradual exposure to traumatic material
Pendulation between activation and safety
Dual attention awareness
4. Expansion of the Window
Repeated successful returns to regulation
Increased tolerance of emotional activation
Strengthened prefrontal–limbic integration
Development of relational safety
What is the Sensorimotor Perspective of Expanding the Window Inspired by?
The work of Pat Ogden. Founder of Sensorimotor Psychotherapy Institute
What does Sensorimotor Psychotherapy emphasize?
Bottom-up processing
Tracking bodily sensations
Working with movement impulses (fight, flight, freeze)
Restoring interrupted defensive responses
Integrating cognition, emotion, and body
What is the Key principle of Sensorimotor Perspective of Expanding the Window:
Change happens through regulated embodied experience, not insight alone
What is a possible exercise to expand the Window o tolerance- through Gratitude and Regulation
writing five things you are truly grateful for today. For example:
A supportive person
A moment of safety
A physical comfort
An opportunity
Something your body allows you to do
After writing, pause and notice:
What happens in your body?
Does your breathing change?
Do you feel any shift in tension or activation?
What is the SMART model? ראשי תיבות
SMART – Sensory Motor Arousal Regulation Treatment
what does SMART emphasize?
Regulation of autonomic arousal before trauma processing
Structured sensory and motor activities
Increasing tolerance for activation within safety
Bottom-up stabilization
Gradual integration of emotional experience
What is the core principle of SMART model?
Resilience develops through repeated experiences of regulation and safety within the body
what is KINTSUGI? what does it represent?
The Japanese art of repairing broken pottery with gold
Our cracks do not define us, but how we fill them, with gold, resilience, and hope, truly does

After Trauma What Do People Need First?
Safety
What needs does Psychological First Aid (PFA) Responds to?
Safety –––> Stabilization –––> Connection
PFA= stabilization
What Does Safety Mean in PFA?
Physical safety
Emotional safety
Informational clarity
Predictability
what is the foundation is the foundation on which all later psychological recovery is built?
Safety
what is Psychological First Aid (PFA)?
A structured, humane response to individuals and communities in the immediate aftermath of a crisis.
Aims of Psychological First Aid (PFA)?
restore safety
reduce acute distress
support stabilization
strengthen connection
link to further help
According to WHO guidelines what are conditions for PFA ?
1.Practical - Safety, Basic needs, Clear information, Human presence.
2.Culturally Sensitive - PFA must adapt to the cultural meaning of crisis.
3.Scalable - It is designed for widespread deployment.
4.Deliverable by Trained Non-Specialists
A Client Walks In. Crying. Shaking. Dissociated. Overwhelmed. What is your first task?
to stabilize him
definition of crisis
temporary collapse of coping capacity
Crisis intervention definition and what it does
Crisis intervention is a time-limited, stabilization-focused response.
Designed to:
• restore emotional regulation
• reduce hyperarousal or dissociation
• re-establish safety and orientation
• mobilize immediate support systems
Crisis intervention is not, and what it is
It is not trauma processing.
It is not psychotherapy.
It is containment and stabilization
In crisis work, what comes first?
In crisis work, safety comes before insight
Regulation comes before reflection.
Stabilization comes before processing
What does Crisis intervention target?
Sympathetic overactivation (fight/flight)
Dorsal vagal shutdown (collapse)
Goal of Crisis intervention
Bring the client back into the Window of Tolerance
when you sit with a client in crisis, what should you ask yourself?
Are they hyperaroused?” “Or are they collapsed?
Psychological Crisis Intervention for hyperarousal?
ypu need to Downregulate :
• Slow voice & pacing
• Extend exhalation
• Ground in the present
• Reduce stimulation
Do not analyze. Regulate
Psychological Crisis Intervention for shutdown?
Gently Activate:
• Increase engagement
• Orient to the environment
• Encourage small movement
• Use relational presence
Do not over-soothe. Re-engage
Is crisis intervention a technique?
Crisis intervention is not a technique. It is state-dependent regulation
Imagine a client who says: “I can’t breathe, I’m going to die.” What do you do?”
“Let’s slow this down.”
“Look at me.”
“Feel your feet on the floor.”
“Long exhale… slower than the inhale.
Imagine a client who says: “I don’t care. Nothing matters.” ’What do you do?
“Can you look around and name three things you see?”
“Press your feet into the floor.”
“Can you feel the chair supporting you?”
“What temperature is the room?”
Phases of Psychological Crisis Intervention
1. Ensure Immediate Safety:
• Medical risk
• Suicide risk
• Environmental danger
2. Regulate the Nervous System:
• Downregulate hyperarousal
• Activate shutdown
3. Restore Cognitive Orientation:
• What happened?
• What is needed now?
• What are the next 24 hours?
4. Mobilize Support:
• Who can help?
• What resources are available?
• What is the follow-up plan?
What is crisis intervention all about?
Crisis intervention is not about solving the person’s life. It is about stabilizing the moment
Common Clinical Mistakes in Crisis Intervention
Processing trauma too early: “Tell me exactly what happened.” “How did you feel in that moment?”
Ignoring suicide risk: “They look calm. They’re fine.”
Over-reassuring: “It’s going to be okay.” “Don’t worry.”
Over-talking
Therapist anxiety: You regulate first yourself. Then the client.
When do crisis interventions fail?
when we move faster than the nervous system
The Role of Multidisciplinary Teams in Crisis Intervention
Collaborative Approach:
Crisis intervention often requires a team of professionals, including psychologists, psychiatrists, social workers, and counselors.
The team works together to provide comprehensive care and support
Summary of video “How stress affects your brain - Madhumita Murgia”
Chronic stress, unlike short-term stress, negatively affects brain structure and function by activating the hypothalamus-pituitary-adrenal (HPA) axis and releasing cortisol.
High cortisol levels increase activity in the amygdala (fear center) and deteriorate the hippocampus (involved in learning and memory), weakening stress control and causing brain shrinkage, particularly in the prefrontal cortex.
This leads to difficulties in concentration, decision-making, and social interaction, and raises risks for depression and Alzheimer's disease.
Stress effects extend to epigenetic changes, as shown in rat studies where maternal care influenced offspring's stress sensitivity and these changes were inheritable across generations.
However, exercise and meditation can reduce stress, increase hippocampus size, and improve memory, offering ways to counteract stress's harmful brain effects.
Summary of video “Trauma and the Nervous System: Stephen Porges & Gabor Maté”
The interview features Gabor and Stephen Porges discussing trauma and the polyvagal theory, which explains how the autonomic nervous system, particularly the vagus nerve, regulates our physiological states in response to safety or threat.
Porges emphasizes that trauma is defined by the body's chronic state of threat rather than just traumatic events.
They explore how facial expressions and voice convey emotional and physiological states, influencing social connection and co-regulation.
The conversation highlights that safety involves active connection, not merely absence of threat, and that societal factors often frustrate this biological imperative for connection, contributing to trauma.
They also discuss how prior autonomic dysregulation predisposes individuals to PTSD and other stress responses, underscoring the importance of understanding trauma through the lens of nervous system regulation and evolutionary biology.
Summary of video “Why the Body with Dr. Pat Ogden”
Pat Ogden, founder of the Sensory Motor Psychotherapy Institute, emphasizes the critical role of the body in psychotherapy, particularly for trauma and attachment issues.
Initially trained in talk therapy, she found integrating body-oriented approaches like posture and movement with traditional therapy led to more lasting change.
Ogden's work began in the 1970s teaching yoga and dance in psychiatric settings, noticing patients improved faster when body work was included.
She studied various body integration methods but realized psychological issues needed addressing alongside physical posture changes for lasting effects.
Sensory Motor Psychotherapy combines top-down talk therapy with bottom-up body awareness, using mindfulness to help clients connect bodily sensations with emotions and memories.
Ogden shares examples of clients whose body postures revealed underlying trauma and emotional blocks, enabling breakthroughs in therapy.
She advocates for the future of psychotherapy to integrate mindful body awareness with traditional approaches for deeper, more integrative healing.
Effective Strategies for De-escalation During a Psychological Crisis
Active Listening - Engaging in empathetic listening to make the individual feel heard and understood. Validating their emotions and experiences without judgment
Calm Communication - Using a calm, soothing tone of voice to help reduce anxiety. Avoiding confrontational language and keeping instructions simple and clear
Non-Threatening Body Language- Maintaining an open, non-aggressive posture. Respecting personal space and avoiding sudden movements
Grounding Techniques- Encouraging the individual to focus on the present moment through breathing exercises or sensory experiences. Using techniques like 5-4-3-2-1 (naming five things they see, four they can touch, etc.) to anchor them to reality
Safety Assurance- Reassuring the individual of their safety and that help is available. Ensuring that the environment is safe and free from potential triggers
whats the Influence of Cultural Factors on Crisis Intervention
Recognizing that cultural background influences how individuals perceive and respond to crises. Being aware of cultural norms around expressing emotions and seeking help
Difference between PFA & Psychological Crisis Intervention
Psychological First Aid (PFA):
Focus: Immediate support after a traumatic event to stabilize and reduce initial distress.
Scope: Addresses basic needs like safety, emotional support, and connection to further help.
Approach: Non-clinical, often provided by trained community members, first responders, or healthcare workers.
Goal: To prevent long-term psychological issues by providing early intervention and connecting individuals to additional resources
Psychological Crisis Intervention:'
Focus: Acute psychological care for individuals experiencing a severe mental health crisis (e.g., suicidal ideation, panic attacks, psychotic breaks).
Scope: Involves clinical interventions such as de-escalation techniques, emergency counseling, and crisis stabilization.
Approach: Typically conducted by mental health professionals with specialized training.
Goal: To manage the immediate crisis, stabilize the individual, and prevent harm to self or others
What does the painting of water lilies by Monet represent?
The water represents the turbulences of life, whereas the lilies represent stabilization.
Prolonged Grief Disorder definition
Persistent and intense grief that does not diminish over time
Prolonged Grief Disorder facts
Duration:
Adults 12+ months
Children/Adolescents: 6+ monthsClinical significance:
• significant distress
• impairment in functioningDifferential diagnosis:
Make sure it’s distinct from PTSD and depression. Grief is the main thing.
Prolonged Grief Disorder symmptoms
persistent longing or preoccupation with the deceased
identity disruption
intense emotional pain
emotional numbness
loneliness
avoidance of reminders
Signs of adaptive grief
emotional pain, but gradual fluctuation of emotions
ability to experience moments of relief or connection
continuing engagement with life
maintaining relationships
capacity to remember the deceased without overwhelming distress
gradual integration of the loss
Signs of pathological grief:
persistent intense yearning
inability to accept the loss
severe avoidance of reminders
identity collapse - “I am nothing without them.”
inability to function in daily life
prolonged grief lasting longer than expected
severe guilt or self-blame
persistent intrusive memories of death
Clinical case- a woman who lost her husbn suddenly lost her husband.
She has symptoms of: intrusive memories, intense guilt, insomnia, avoidance of shared place. Is this grief, trauma, or both?
Both
When does Traumatic/Complicated grief occur?
when responses to trauma, and to losing someone- overlap
Traumatic/Complicated grief is a combination of:
1. Grief processes:
intense longing for the deceased
sadness and emotional pain
preoccupation with memories of the relationship
2.Trauma symptoms:
intrusive images of death
avoidance of reminders
hyperarousal (sleep disturbance, anxiety)
What often happens to people with Traumatic/Complicated grief?
Clients often alternate between Attachment activation (yearning for the person who died), and Threat avoidance (avoiding reminders of how the death occurred).
They want to remember the person, but not how he died, which might complicate therapy.
what difficulties can Traumatic/Complicated grief bring to therapy?
The person might be hyper-aroused because of the trauma, but he might also be hypo-aroused because of the grief.
We need to adjust treatment to his current state.
Therapeutic Approaches in Traumatic Grief
Treatment often requires addressing both trauma and grief processes
Stages:
1.Stabilization and Safety:
emotion regulation
grounding techniques
strengthening coping resources
2. Trauma Processing
EMDR or other trauma-focused therapies
reducing intrusive memories and distress
3. Narrative Integration
Reconstructing the story of the loss
meaning-making and memory integration
4. Gradual Exposure to Memories
safely approaching avoided reminders
integrating both the relationship and the loss
What is the goal of therapy in Traumatic grief
The goal of therapy is not to erase grief, but to help the client integrate the loss without being overwhelmed by trauma
Who wrote the book about Meaning Reconstruction in Grief Therapy?
Robert A. Neimeyer,
The ideas of Meaning Reconstruction in Grief Therapy
1. Focus of therapy:
reconstructing meaning after loss
integrating the loss into personal narrative
exploring identity transformation
2. Key therapeutic processes:
narrative reconstruction
meaning-making
continuing bonds with the deceased
3. Clinical relevance: Especially helpful in:
complicated grief
traumatic loss
identity disruption
What is the Grief Support Specialist Certificate in University of Wisconsin–Madison (USA)? What does it include?
An example of structured training in grief support.
1. Focus of the program:
understanding grief processes
supporting bereaved individuals
communication skills in grief contexts
2. Key areas:
normal vs complicated grief
cultural aspects of grief
grief across the lifespan
ethical and professional boundaries
3. Skills developed:
active listening
emotional support
grief-informed communication
Types of Grief
Normal Grief: Typical emotional, physical, and cognitive reactions that gradually adapt over time.
Complicated Grief: Prolonged and intense grief that impairs daily functioning.
Anticipatory Grief: Grief experienced before an impending loss, often in terminal illness cases.
Disenfranchised Grief: Grief not socially recognized or supported
Possible Sources of grief
death of a loved one
peritraumatic loss - safety, trust, identity, loss of control over life
divorce or relationship breakup
loss of health or functioning
migration, displacement
loss of future expectation
Cultural Considerations in Grief
Cultural Variations: Different cultures have unique mourning practices and beliefs about death.
Cultural Sensitivity: Adapting interventions to respect and incorporate cultural practices.
Adapting Compassionate Inquiry Across Cultures
Case Example: Supporting a grieving family from a culture that emphasizes collective mourning rituals
Possible Therapeutic Interventions for Trauma
Eye Movement Desensitization and Reprocessing (EMDR)
Group EMDR Integrative Group Treatment Protocol (IGTP) (IGTP) with Drawing Protocol
Sensorimotor Psychotherapy
Internal Family Systems (IFS) Therapy
Prolonged Exposure Therapy (PE)
Virtual Reality Exposure Therapy (VRET)
who’s the founder of EMDR?
Francine Shapiro
Definition of EMDR
EMDR is a psychotherapy that enables people to heal from their symptoms and emotional distress resulting from disturbing life experiences. Strong empirical support for EMDR in treating PTSD.
It uses bilateral stimulation (eye movements, taps, tones).
Phases of EMDR
History taking, Preparation, Assessment, Desensitization, Installation, Body Scan, Closure, Reevaluation
Tools Used in EMDR Therapy
1. Eye Movements Therapist-guided eye tracking
2. Auditory Stimulation (Sound):
Alternating tones (left ↔ right)
Delivered via headphones
3. Tactile Stimulation (Tappers)
Handheld devices (“tappers”)
Gentle alternating vibrations
4. Self-Administered BLS (Butterfly Hug):
Client crosses arms and taps alternately
Promotes: grounding, emotional regulation
Often used in: group settings, stabilization phase, crisis intervention
5. Other Forms:
Therapist tapping (e.g., knees, hands)
Visual light bars
Digital EMDR tools
What are the EMDR Professional Organizations
1. EMDR International Association (EMDRIA): Global professional organization for EMDR therapy, founded in the United States. Sets international standards for training and certification.
2. EMDR Europe Association: Professional organization representing EMDR therapy across Europe
3. EMDR Training Pathway (Europe):
Entry Requirements
Completed or ongoing accredited psychotherapy training.
Clinical experience is required.
Structure of EMDR Training:
Part 1 (theory + practicum)
Part 2 (advanced protocols
EMDR Europe Conference 2026: Location, who organizes it, focus and why it matters.
Location: Oslo, Norway. Organized by EMDR Europe Association Gathering of clinicians, researchers, and trainers.
Focus: Latest research in trauma and EMDR, Clinical innovations and case-based learning Workshops, panels, and live demonstrations
Why It Matters: Reflects current developments in trauma therapy , Connects professionals across countries, Supports lifelong professional growth
Integrative Group Treatment Protocol (IGTP) - case study facts
They drew together
8 women
16-week program, 1x weekly / 120 minutes
Socially disadvantaged community
Exposure to: Domestic violence; Loss and grief; Chronic poverty stress; Interpersonal conflict
Symptoms: Anxiety; Depression; Emotional dysregulation; Sleep disturbance; Parenting stress
Integrative Group Treatment Protocol (IGTP) - case study phases
Stabilization & Preparation (Weeks 1–4)
Trauma Processing (Weeks 5–13)
Integration & Closure (Weeks 14–16)
Integrative Group Treatment Protocol (IGTP) - case study advantages
No need for verbal trauma disclosure
Group support reduces isolation
Efficient and scalable
Core Principles of EMDR IGTP
Parallel processing (each client works internally)
No forced sharing of trauma content
Use of drawing instead of narration
Bilateral stimulation (butterfly hug)
Strong emphasis on stabilization
EMDR IGTP Drawing Protocol
Each session:
1.Stabilization (breathing, grounding)
2.Identify target memory (no sharing required)
3.Draw the memory / symbol
4.Rate distress (SUD)
5.Bilateral stimulation (butterfly hug)
6.Re-draw (after processing)
7.Body scan
8.Return to safe place
Why Drawing is good in EMDR IGTP case study
Bypasses verbal limitations
Reduces shame
Accesses implicit memory
Culturally adaptable
Sensorimotor Psychotherapy: founder, definition, techniques, theoretical basis and application
Founder: Pat Ogden
Definition: Body-centered approach that integrates cognitive and somatic techniques to treat trauma.
Techniques: Body awareness, mindfulness, movement exercises.
Theoretical Basis: Based on the connection between physical sensations and emotional trauma.
Application: Particularly effective in treating trauma that manifests in physical symptoms
Internal Family Systems (IFS) Therapy: Founder, Definition, Key concepts, and Application
Founder: Richard C. Schwartz
Definition: IFS is a form of psychotherapy that identifies and addresses multiple subpersonalities or "parts" within a person’s mental system.
Key Concepts:
The concept of “Self” and its role in healing
Parts: Exiles (Hold pain, trauma, shame, sadness. Often pushed away or “hidden”), Managers (Try to keep you in control and safe), Firefighters(Act when emotions get overwhelming).
Application in Trauma: IFS helps individuals understand and heal the inner parts that hold traumatic memories
Prolonged Exposure Therapy (PE)- Founder,Definition, Core techniques and theoretical basis
Founder: Edna Foa
Definition: Evidence-based trauma-focused therapy that reduces PTSD symptoms through systematic, repeated exposure to trauma-related memories and situations.
Core Techniques:
Imaginal exposure (revisiting the traumatic memory in detail)
In vivo exposure (gradual confrontation of avoided situations)
Emotional processing of fear responses
Theoretical Basis: Based on emotional processing theory, trauma persists because of avoidance and fear structures; exposure allows corrective learning and habituation
Video about “understanding our inner critic”
Critical voice- How do we speak to it? We need to be mindful to it, and curious. We need to understand it. We cant understand it if we hate it.The voice will tell us- he’s doing this to protect us.
Summary of video “How Does Virtual Reality Exposure Response Prevention Therapy Work?”
Virtual reality exposure therapy involves clients wearing a VR headset to immerse themselves in anxiety-provoking scenarios under clinician guidance.
The clinician monitors anxiety levels and adjusts virtual scenarios to keep exposure challenging yet manageable.
Repeated exposure helps reduce anxiety and build confidence by weakening the link between feared situations and anxious responses.
This therapy is effective for various anxiety disorders such as phobias, social anxiety, panic disorder, and PTSD, with lasting symptom improvements comparable to traditional exposure therapy.
Summary of video “Edna B. Foa, Ph.D. Talks About Anxiety, Trauma”
Dr. Edna Foa is a leading expert on PTSD who developed prolonged exposure (PE) therapy over 30 years ago, now a frontline treatment worldwide.
Initially interested in how people process distressing events, she focused on sexual assault victims and anxiety symptoms before PTSD was formally recognized in DSM-III.
She adapted exposure therapy used for phobias to address traumatic memories in PTSD, creating PE therapy with four components: education, breathing exercises, imaginal exposure (revisiting traumatic memories in detail), and in vivo exposure (gradual real-life confrontation of avoided situations).
PE helps patients confront and process traumatic memories and related fears, reducing symptoms by teaching them they can tolerate distress and that many feared situations are safe.
Despite initial skepticism, especially about treating women, PE has shown strong results, with 40-50% of patients losing their PTSD diagnosis and no evidence of harm.