wilhelm diarrhea and constipation
1/80
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
81 Terms
what are the 3 types of solute movement btwn GI lumen and blood
1. active transport= pumps against a gradient (ex: AAs and glucose)
2. diffusion= no energy, goes from high to low concentration
3. solvent drag= when water moves it drags along molecules with it (ex: sodium)
3 patterns of muscle contraction in GI
1. non-propulsive segmental= churning in one place. not moving.
2. short segmental propulsive= move short distance
3. long segmental propulsive= move long distance (migratory motor complex MMC)
diarrhea is caused by a disruption of which 4 mechanisms
1. change in active ion transport
2. change in intestinal motility
3. increase in luminal osmolarity
4. increase in tissue hydrostatic pressure
how can an increase in tissue hydrostatic pressure cause diarrhea
if walls of GI are engorged with fluid, extra pressure makes it harder for anything to pass and harder to absorb nutrients/water-> causes diarrhea
ex: edema in heart failure, kidney dysfunction
4 classifications of diarrhea
1. secretory (a lot of water)
2. osmotic (poorly absorbed things)
3. exudative (inflammation)
4. altered intestinal transit (increased motility)
describe secretory diarrhea
potential causes?
either increased secretions into GI or decreased absorption of water back into body
- large volume, isotonic
- NOT altered by fasting
causes:
- dietary fat
- laxatives
- hormones
- bacteria
- excess bile salts
t/f: secretory diarrhea may be altered in the presence of fasting
false. if pt stops eating, secretory diarrhea still ensues
describe osmotic diarrhea
potential causes?
poorly absorbed substances remain in GI and pull water in
causes:
- lactose intolerance
- lactulose
- celiac disease
- pancreatic insufficiency
- antacids (magnesium
subsides after pt fasts!!
t/f: osmotic diarrhea may be altered in the presence of fasting
true. osmotic diarrhea is a result of a substance not being absorbed. fasting may eliminate diarrhea. this is a differential btwn secretory diarrhea
describe exudative diarrhea
causes?
inflammation causes mucus, blood, and serum proteins to move into gut (leaky walls)
causes:
-graft versus host disease
- colitis
-IBD
- colonic neoplasma
- invasive infections
what can cause altered intestinal transit diarrhea
- pro-kinetic meds (erythromycin)
- surgery (resections/bypass bc shortened GI tract)
- IBS
- diabetes
increased motility causes less fluid to be absorbed= diarrhea
common infections that may cause diarrhea
- e. coli
- campylobacter
- c. diff
- salmonella
- shigella
- rotavirus
- norwalk virus
which medications can cause diarrhea
Magnesium (antacids)
Laxatives
Prokinetic agents
Broad spectrum abx (c. diff prevails)
Erythromycin
Statins
Theophylline (structure like caffeine)
Digoxin
Cholinergics (para= rest/digest)
Anti-arrhythmias
Propranolol
NSAIDs
Colchicine
BEST Diarrhea CAP NC "best diarrhea capsules not covered"
JL has started drinking 2 glasses of milk a day and has had 2-3 loose stools per day. Today she doesnt drink milk and does not experience anything. What type of diarrhea is this?
osmotic (due to lactose intolerance/ indigestibles most likely)
acute vs chronic diarrhea
acute: 0-14 days, self limiting, tx symptomatically
chronic: >14 days, fluids, electrolytes, abx
oral rehydration is a key tx for diarrhea to prevent dehydration. what should you look for when recommending smtg for rehydration
sugar! solution must have sugar to be taken in via active transport and for water and electrolytes to follow
ex: pedialyte
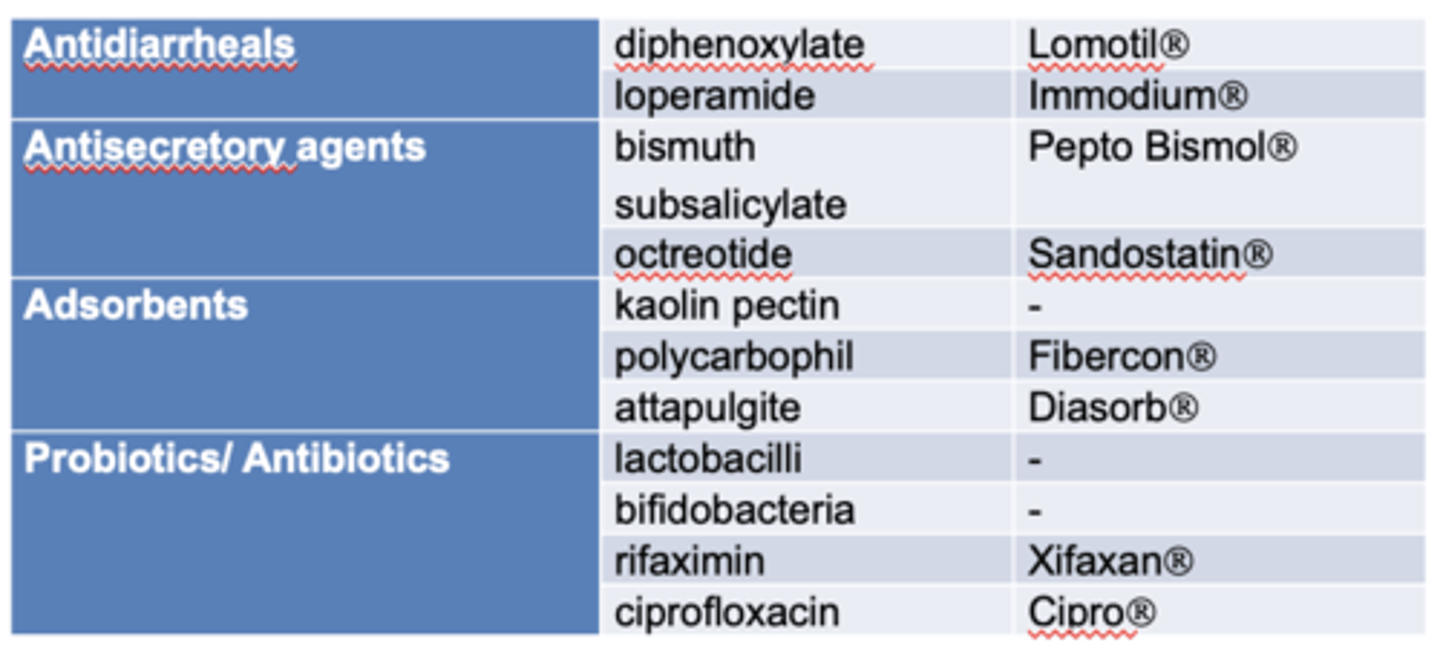
how do adsorbents work to treat diarrhea? example?
=fiber supplement soaks up fluid and adds bulk to stool to lessen diarrhea
- remember it not only absorbs water, but drugs and nutrients too. so separate other oral meds
ex: polycarbophil (Fibercon)
a pt comes into the pharmacy asking if they can take fiber for their diarrhea. what is your reply
yes. only adsorbent recommended by FDA is polycarbophil (Fibercon)
-fiber will soak up the excess liquid but it will also absorbs drugs
- SEPARATE oral meds from the Fibercon
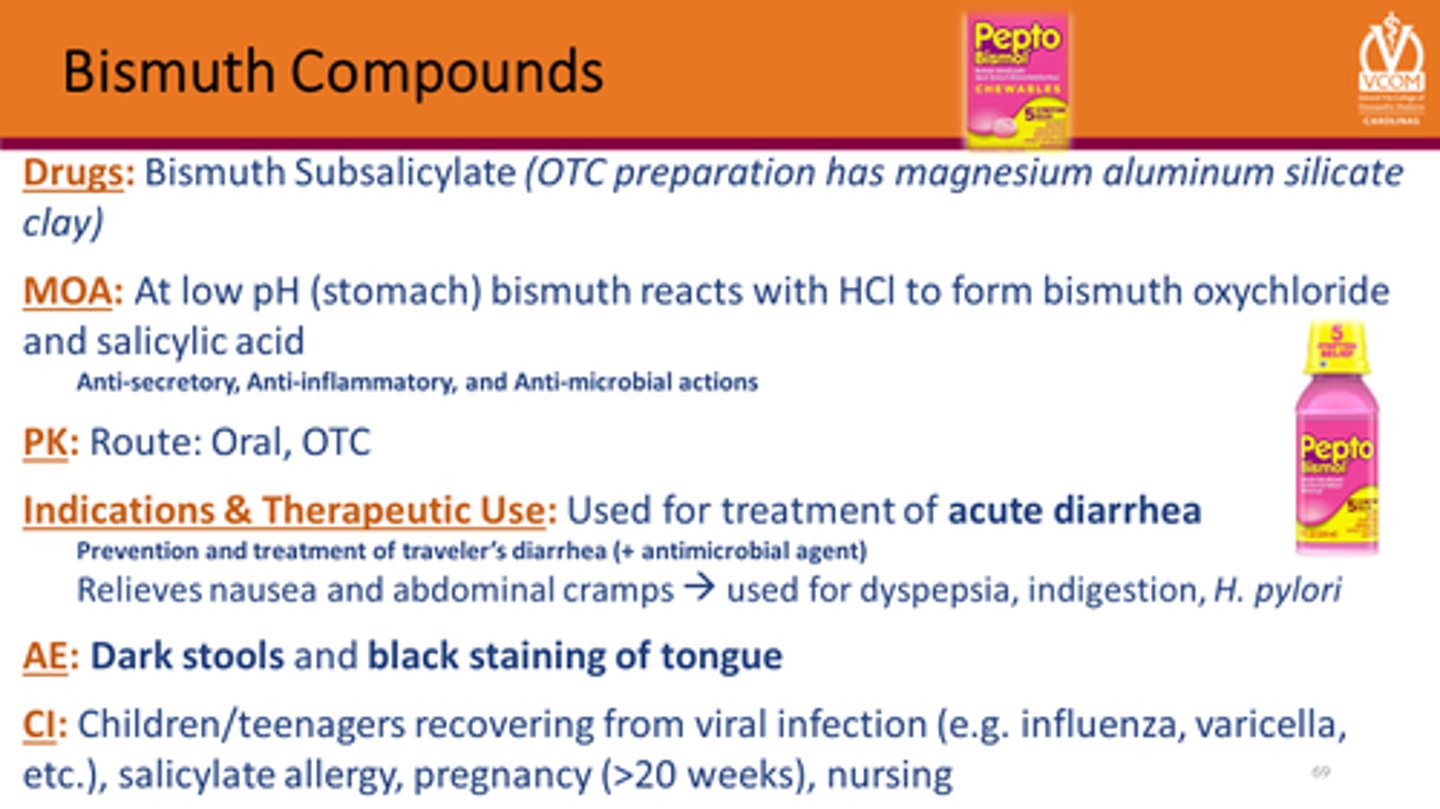
how is pepto bismol (bismuth subsalicylate) used for diarrhea?
CI:
ADRs:
DDI:
its an anti-secretory that reduces fluid secretion into bowel
CI: aspirin allergy (bc of salicylate)
ADRs: black tongue, dark stool, tinnitus, gout attack
DDI: warfarin (bc salicylate, may increase bleeding)
summary tx options for diarrhea with no fever/systemic sx
1. oral rehydration= smtg with water, electrolytes, glucose
2. Fibercon (polycarbophil)= soaks up like sponge
3. Antisecretory= bismuth subsalicylate, octreotide (subQ)
4. opiate derivatives/ antimotility= loperamide, diphenoxylate, opium tincture
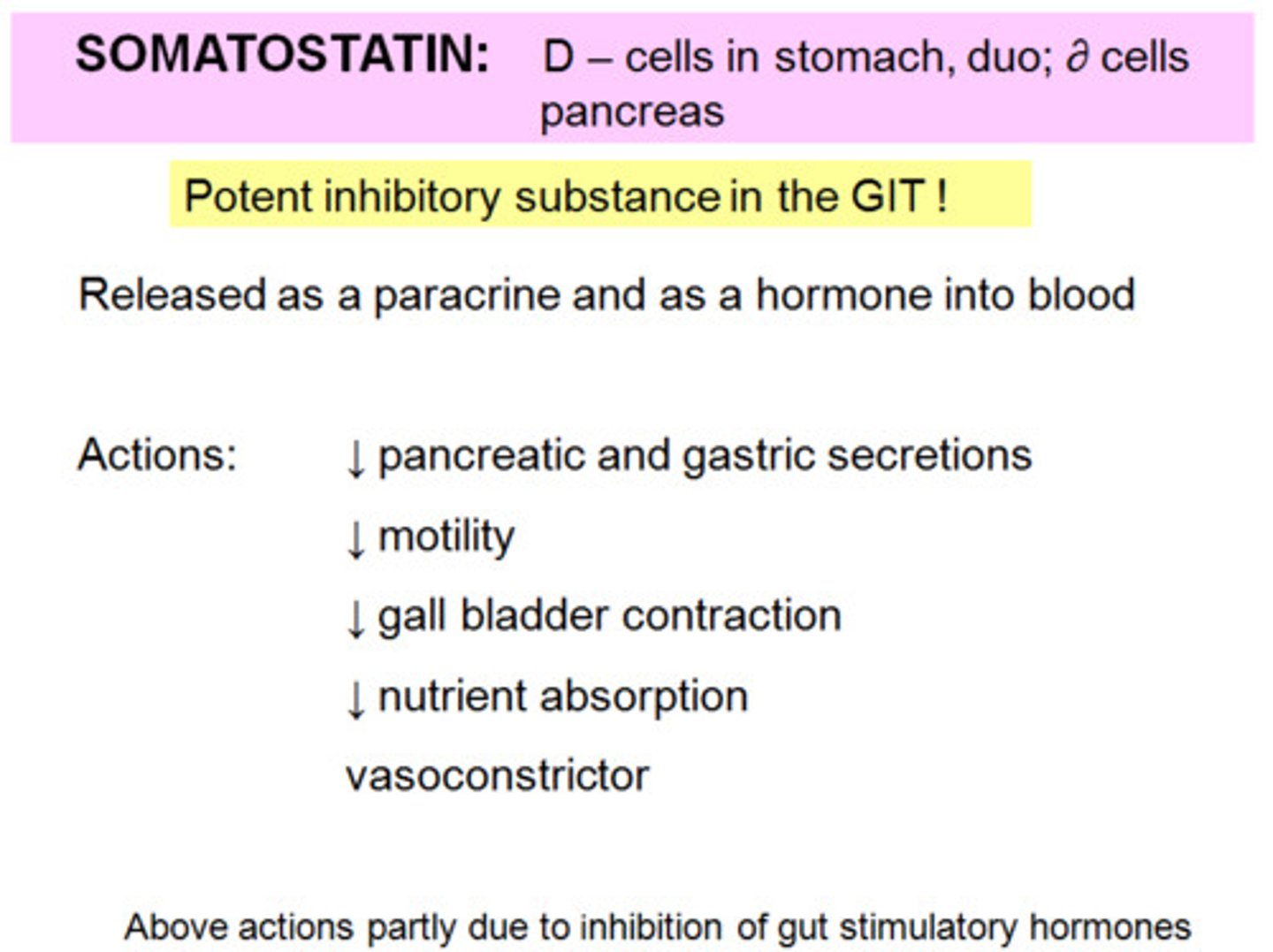
octreotide (Sandostatin)
RX injectable for long term diarrhea
- for diarrhea caused by vasoactive substance secreting tumors
- antisecretory
ADRs: cholelithiasis, steatorrhea
loperamide
Imodium (OTC)
-opiate derivative that lowers GI motility
-mainly peripheral activity; low abuse potenntial

diphenoxylate + atropine
Lomotil (Rx)
- opium derivative that lowers GI motility + anticholinergic (to lower abuse & additive effect)
- side effects: cholinergic bc of atropine

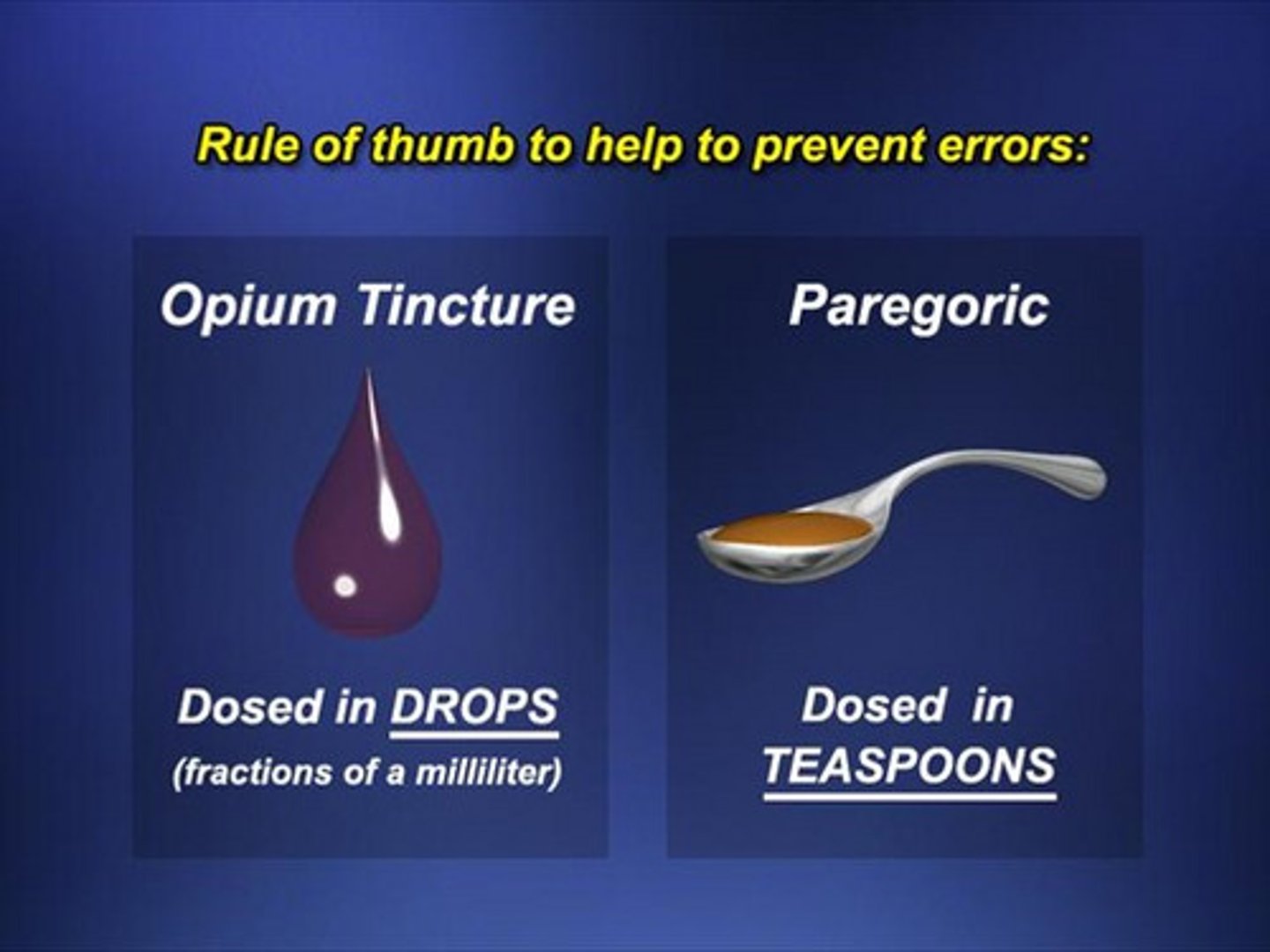
opium tincture/ anhydrous morphine
Paregoric
- old opium derivative that lowers GI motility. high abuse potential. not rlly used
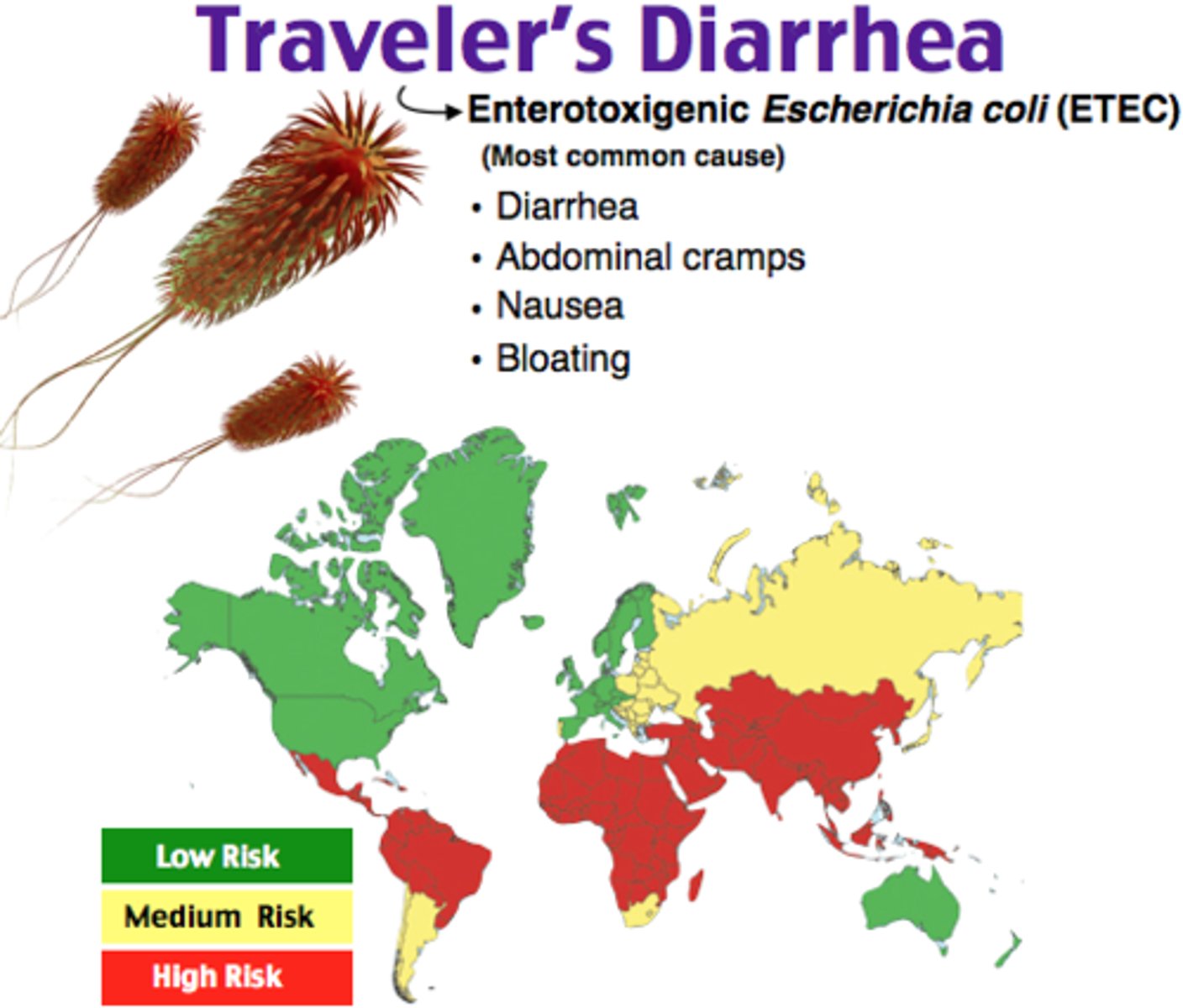
which infectious agents most often cause traveler's diarrhea
E. coli= main
Shigella
Campylobacter
Salmonella
Viruses
what can increase the risk for traveler's diarrhea
- traveling near equator
- immunocompromised
- high gastric pH ex: PPIs (no acid to kill off bacteria)
symptoms of traveler's diarrhea
- begins within first several days
- lasts 4 days without treatment
abdominal pain, cramping, N/V, tenesmus (incomplete after stool passes)
may or may not have fever and bloody stool
traveler's diarrhea prophylaxis (what should u suggest to pts before/during travel?)
- food: peel/boil/cook. dont eat raw or skin
- purify water. dont add ice
- probiotics shown to be effective BUT take the entire time
-travel kit: bismuth subsalicylate, loperamide, 3 day course of abx
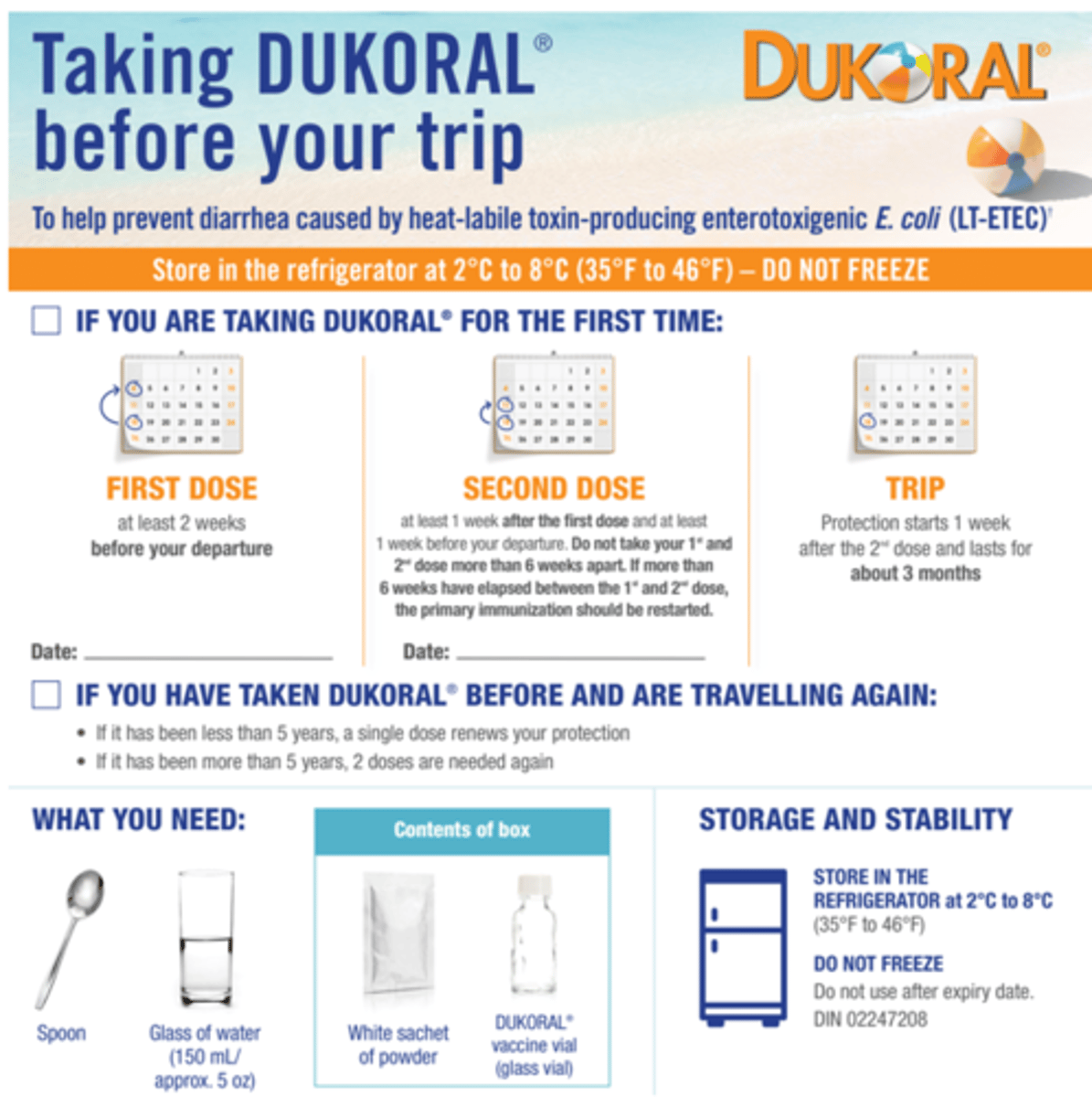
which vaccine is given for TD prophylaxis in Canada without prescription?
Dukoral
- recombinant Cholera toxin
- ORAL vaccine for 2+
- protects against 25% of cases
which vaccine is given in US for TD? is this generally recommended?
Vaxchora (oral cholera vaccine)
- for adults 18-64 (compare to Dukoral 2+)
- not rlly recommended bc not studied in TD prevention
2 OTC treatments for symptomatic traveler's diarrhea. which is more effective?
- loperamide= MORE EFFECTIVE
- bismuth subsalicylate
do not use if blood in stool or fever!!
when can antimotility agents be used in traveler's diarrhea tx
adjunct to abx only if there is NO BLOOD and NO FEVER
t/f: antimotility agents combined with antibiotics are safe and effective for diarrhea with fever as long as there is no blood in stool
false. effective and safe only if NO BLOOD and NO FEVER
when can you NOT use bismuth subsalicylate (pepto bismol)
- doxycycline for malaria prophylaxis (complexes together)
- anticoags, aspirin, NSAIDs (bleeding risk)
- pregnant
- aspirin allergy
-> use loperamide instead!
pt MA is pregnant and experiencing traveler's diarrhea. she heard that pepto bismol is good for symptomatic TD. what do you tell her
pepto bismol and loperamide are good for traveler's diarrhea BUTTT pepto bismol is not recommended in pregnancy AND loperamide is more effective
which antibiotics can you consider for TD tx
1. azithromycin= preferred for severe and systemic (ok in pregnancy)
only if no blood/ no fever:
2. ciprofloxacin/ Levofloxacin (NOT in pregnancy)
3. rifaximin/ Xifaxan (for NON-invasive only/ localized to GI)
4. rifamycin (for NON-invasive only/ localized to GI)
Pt PH had been prescribed azithromycin for severe TD. He does not have bloody stools or fever. What else can be added to his tx plan?
add antimotility agent like loperamide
-> may also consider switching to rifaximin/rifamycin/cipro
what is the best TD tx option if there is blood in the stool or a fever is present
Azithromycin
-cipro and rifaximin only target GI. Azithro is good for systemic infections
- do NOT use antimotility agents like loperamide!!
what is the proper day therapy for azithromycin for TD
500mg daily x 3 days
or
1000mg x 1 day
t/f: in TD, the presence of fever and bloody stool suggests the need for a systemic antibiotic like azithromycin, and the discontinuation of all antimotility agents such as loperamide
true
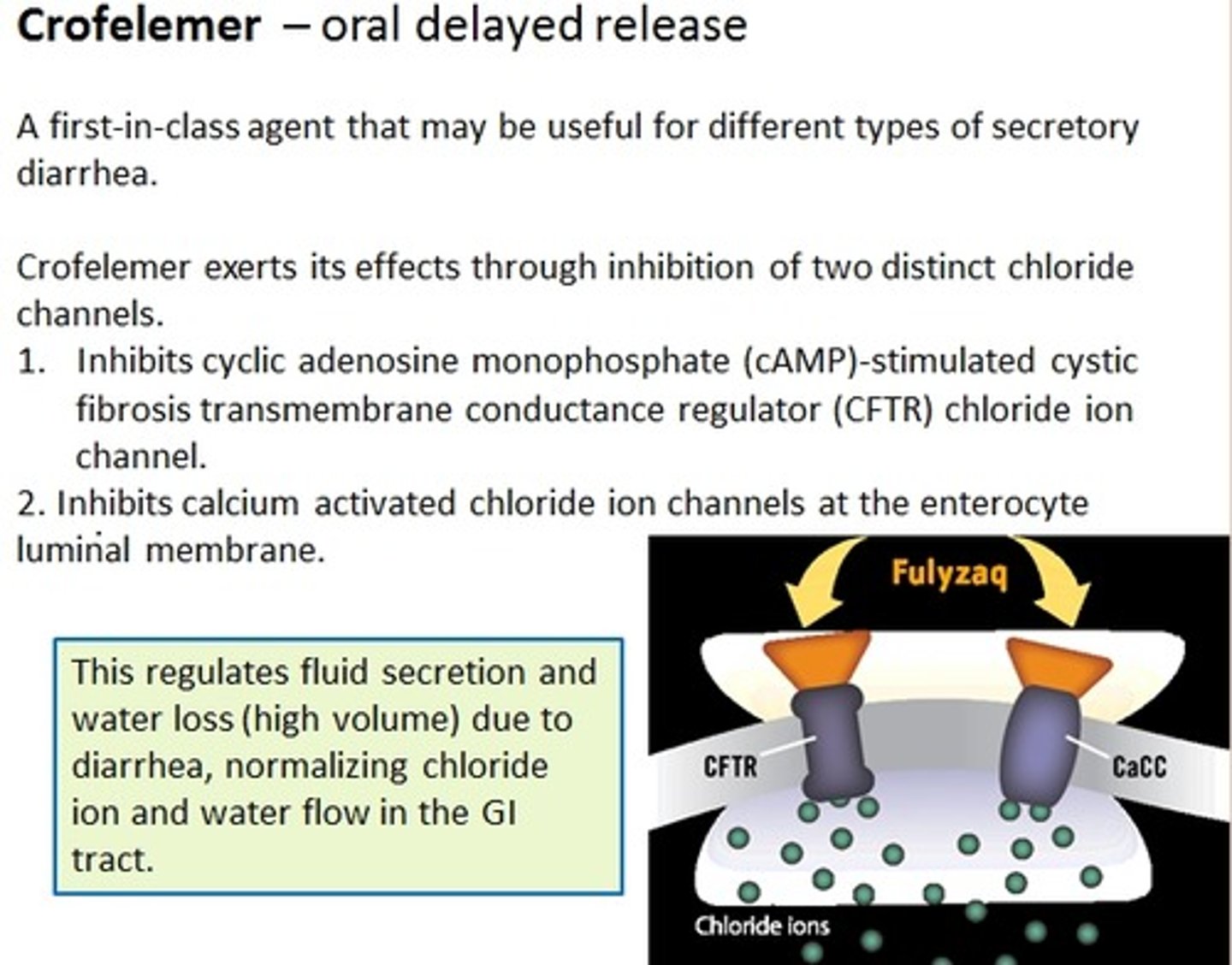
Crofelemer
MOA?
Mytesi
relief of non-infectious diarrhea in adults with HIV/AIDS on antiretroviral tx
moa: blocks chloride channels from pushing Cl into GI therefore reducing water movement
DELAYED RELEASE DO NOT CRUSH
Rome IV functional constipation criteria must be fulfilled for how long?
criteria fulfilled for last 3 months with sx onset at least 6 months prior to dx
t/f: a major aspect of constipation is <3 bowel movements/week or 3 days without a bowel movement
true
Rome IV functional constipation criteria
1. two or more of the following for >25% of time
-straining, lumpy/hard, incomplete sensation, sensation of blockage, manual maneuvers, <3 movements per week
2. loose stools=rare
3. insufficient criteria for IBS
MUST happen during last 3 months with sx onset >6 months ago to be classified as functional constipation (chronic)
which medications can cause constipation
antacids= calcium, aluminum
anticholinergics (antihistamines, TCAs, phenothiazines, antiparkinsons, atropine)
calcium channel blockers
clonidine
diuretics
iron
opiates
resins
laxative abuse
nonpharm tx for constipation (summary)
-physical activity
- dietary fiber
- fluid
- hot, caffeinated beverage after waking
- breakfast within 1hr of waking
- good sleep
- toilet training (schedule, <10mins, avoid strain, relax, position)
proper toilet training for constipation
- have routine regardless of urge
- dont ignore urges
- dont remain on toilet >10mins
- avoid straining
- deep relaxation
- proper position (squat)
bulk-forming agents for constipation
moa?
meds?
counseling?
FIRST LINE for long term (NOT ACUTE TX)
- increases bulk in intestines-> draws out water into GI
meds:
-methylcellulose (Citrucel)
-polycarbophil (Fibercon)
-psyllium (Metamucil)
counseling:
ADRs: distention, cramps, gas
- effect in 3-5 days
- will get worse before it gets better since fiber is adding even more bulk before it draws out the water and eventually helps pass stool
- start w low dose and go higher
what can
-methylcellulose (Citrucel)
-polycarbophil (Fibercon)
-psyllium (Metamucil)
be used for?
first line tx for constipation (not acute relief!!!). will pull water into GI
- polycarbophil can also be used for diarrhea to act as sponge and soak up water
stool softeners
moa?
meds?
counseling?
moa: reduce surface tension/ increase stool fluid content (surfactants)
NOT for acute constipation. only for preventing constipation.
- softer stool within 1-3 days
med: docusate sodium (Colace)
why are lubricants (ex: mineral oil) for constipation not generally recommended
1. if absorbed, can have immune rxn
2. aspiration-> lipid pneumonia
3. reduced ADEK absorption
4. pruritus, ruins clothes
[also takes 2-3 days to work. it lubricates feces to prevent water from reabsorbing]
how do hyperosmotic agents for constipation tx work
by adding large non absorbable molecules, water is dragged into stool= increases distention, reduced transit time
GOOD FOR ACUTE TX
meds:
- glycerin suppository (good for children!)
- lactulose
- sorbitol
which OTC constipation tx is good for children
glycerin suppository
which OTC constipation tx are good acutely? long term? (summary)
acute:
1. hyperosmotics (glycerin suppository, lactulose, sorbitol)
2. saline laxative (magnesium citrate, magnesium hydroxide, PEG)
3. stimulants (senna, bisacodyl, cascara)
chronic:
1. bulk forming (methylcellulose, polycarbophil, psyllium)
2. stool softener (docusate)
never:
1. mineral oil
saline laxatives for constipation tx
moa?
meds?
caution?
- osmotic effect: more salt in GI= pulls in fluid
- RAPID! 1-6hrs if by mouth, <1hr rectally
meds:
- Mg citrate, Mg hydroxide, Mg sulfate
- PEG (GoLYTELY w electrolytes orrr Miralax without)
caution: dont give high electrolyte load to renal or heart failure pts
which pts should be cautious of GoLYTELY
heart or renal failure
GoLYTELY is PEG with electrolytes (saline laxative). the high electrolyte load might mess w conductivity. opt for miralax (without electrolytes) instead
what is GoLYTELY used for
Used to clean the bowel before colonoscopy, a barium xray, or other intestinal procedures
(basically Miralax with electrolytes, caution in heart or renal failure pts)
constipation tx: stimulants
moa?
meds?
counseling?
moa: stimulate peristalsis via mucosal irritation and nerve plexus activity
meds:
- senna
- bisacodyl (Dulcolax)
- cascara sagrada
counseling:
- effects in 6-12hrs
- ACUTE use only (chronic= cramps, electrolyte imbalance)
melanosis coli is seen in ____________
stimulant laxative abuse (darkening of GI lining. will go away once u stop using)
lubiprostone
brand?
moa?
dose?
ADRs?
Amitiza
moa: chloride channel activator (pushes Cl into GI to draw Na and water in to help constipation)
- for chronic idiopathic constipation
dose: 24mcg BID WITH FOOD!!
ADRs:
1. nausea, diarrhea
2. abdominal pain/distention
3. flatulence
PREGNANCY CATEGORY C
t/f: Crofelemer and lubiprostone have similar moas, with crofelemer activating Cl channels and lubiprostone blocking them
false. opposite
crofelemer= blocks Cl channels to lower water secretion into GI (diarrhea in HIV/AIDS)
lubiprostone= activates Cl channels to increase water in stool (CIC or OIC)
linaclotide
brand?
use?
Linzess
for chronic idiopathic constipation
- amino acid peptide
- take 30 mins before breakfast QD
ADULT USE ONLY
ADE: just diarrhea. not rlly systemically absorbed
plecanatide
brand?
use?
Trulance
for chronic idiopathic constipation
- amino acid peptide
- take without regard to food
ADE: just diarrhea. not rlly systemically absorbed
t/f: linaclotide and plecanatide are both amino acid peptides that work on guanylyl cyclase to increase cGMP and stimulate chloride channels to help with constipation
true
prucalopride
brand?
moa?
ADE?
counseling?
Motegrity
for chronic idiopathic constipation QD (adults)
MOA: 5-HT4 serotonin agonist/ prokinetic agent
ADE: diarrhea, flatulence, distention, headache
counseling: taken without regard to meals
Rx chronic idiopathic constipation tx options (summary)
1. lubiprostone (Amitizia)= BID with food (bc nausea). pregnancy category C
2. linaclotide (Linzess)= QD before breakfast; good ADE
3. plecanatide (Trulance)= QD regardless of food; good ADE
4. prucalopride (Motegrity)= QD regardless of food
PAMORAs
moa:
drugs:
indication:
peripherally acting mu-opioid receptor antagonist
drugs:
1. methylnaltrexone (Relistor)
2. naloxegel (Movantik)
3. Naldemedine (Symproic)
indication: opioid induced constipation for opioids >4 weeks
PAMORAs
ADEs:
CIs:
ADEs: ab pain, flatulence, diarrhea, dizziness
CI: GI obstruction!! (dont use any laxatives)
methylnaltrexone
brand
moa
use
Relistor
PAMORA= peripherally acting mu-opioid receptor antagonist
- does not pass BBB so allows opiates to work centrally but stops constipation
- tabs or subQ injection

naloxegol
brand
moa
Movantik= OIC
PAMORA= peripherally acting mu-opioid receptor antagonist
-Pgp substrate!! efflux across BBB

naldemedine
brand
moa
Symproic
PAMORA= peripherally acting mu-opioid receptor antagonist
- does not pass BBB so allows opiates to work centrally but stops constipation
which tx for constipation can be given to pregnant patients? cant?
give= bulk forming agents and stool softeners (BUT not for acute)
cant= stimulants (may still be used but cautionn uterine contractions)
(AVOID MINERAL OIL)
nursing home/ bedridden pts constipation management
need bowel regimen chronically:
- bulk forming agents
- stool softeners
- stimulants prn only
(AVOID MINERAL OIL)
when is the only time that stimulant laxatives may be used chronically
opioid induced constipation. opioids lower GI motility so stimulants are needed and are more effective than bulk forming agents
t/f: stimulants are more effective than bulk forming agents in opioid-induced constipation
true
which chronic idiopathic constipation med can also be used for opioid induced constipation
lubiprostone
which agents help relieve constipation in <6hrs
- magnesium citrate (saline laxative)
- magnesium hydroxide
- magnesium sulfate
- bisacodyl suppository (stimulant)
which agents help relieve constipation in 6-12hrs
- bisacodyl (oral)
- senna
(stimulants)
which agents help relieve constipation in 1-3 days (not for acute tx)
1. bulk forming/osmotics
- methylcellulose
- polycarbophil
- psyllium
2. stool softeners
- docusate
- lactulose
- mineral oil (NEVER RECOMMEND THIS)
which of the following is not an appropriate tx for opioid induced constipation
a. docusate/ senna combo bid
b. methylnaltrexone
c. naloxegol
d. lubiprostone
e. psyllium
e. psyllium
this is bulk forming and will make the constipation worse since GI motility is lowered in opioid-induced constipation
a pregnant pt comes in complaining of constipation due to increased iron intake. what suggestions can you give to her
non pharm: increase fluids, exercise, high fiber diet
pharm: stool softeners, fiber once constipation resolves
may use stimulants at lowest dose for shortest time onlyyy if necessary. warn about uterine contraction risk