Heart Failure 1
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
myths and misinformation about alcohol and heart health
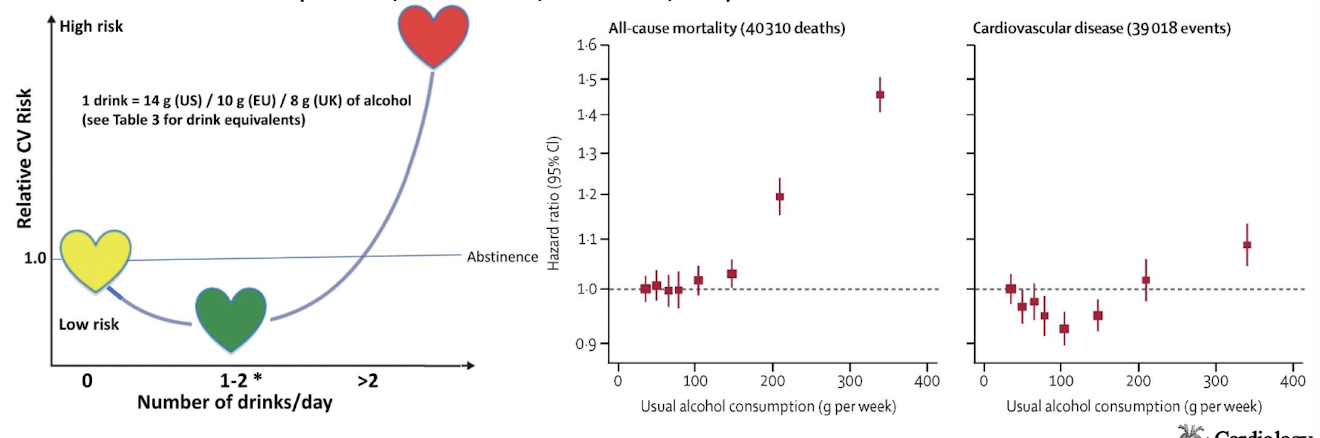
J-shaped curve - low levels of consumption healthy
likely the product of higher income, more activity & healthier lifestyle
what is the safe level of alcohol consumption
cardiomyopathy risk rises at >80g/day over 5 years
risk for women appears to rise at 50% of the level for males
many confounding variables like diet, exercise, etc
other risks (cancer, accidents, cirrhosis, etc)
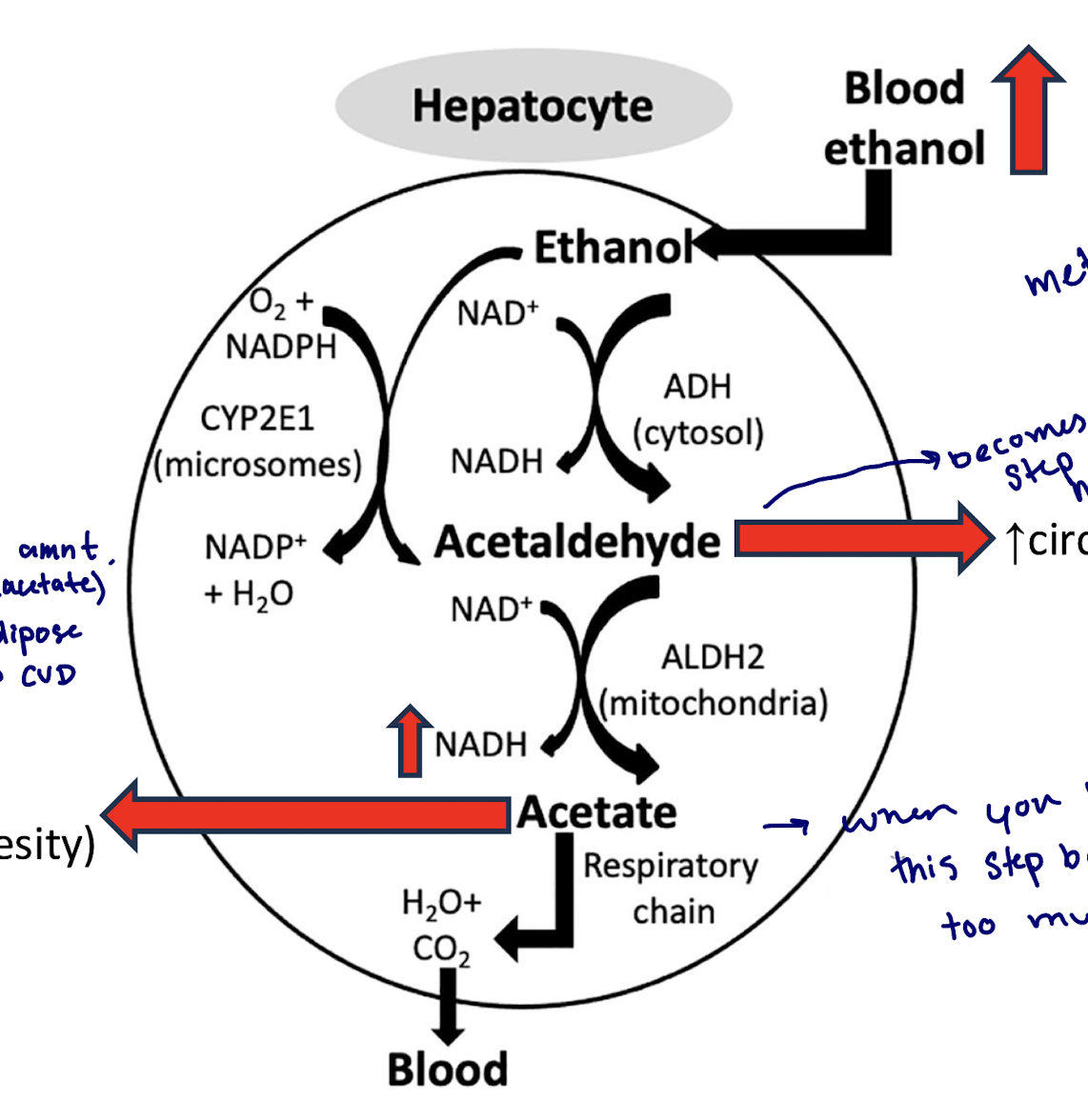
ethanol is metabolized by CYP2E1 to acetaldehyde
acetaldehyde increases circulating acetaldehyde
ALDH2 metabolizes acetaldehyde to acetate
excess acetate is transferred to lipogenesis and becomes adipose tissue (increases CVD risk)
what becomes the rate limiting step when you consume too much
acetaldehyde → enters blood → is a toxin → causes hangover → acute acetaldehyde poisoning
what step backs up when you have too much to drink
acetate → this step backs up because too much NADH
effects of chronic high acetaldehyde
DNA damage → increased apoptosis
w/ loss of cardiac myocytes, you lose contractility
impaired mitochondrial function
disrupts energy proteins
increased oxidative stress
release of proapoptotic factors (e.g. cytochrome C)
mtDNA damage (decreased mt biogenesis)
cardiomyocyte cell death, fibrosis
loss cardiac myocytes and replace with fibrosis… stiffer, acts as a load, harder to contract
endothelial dysfunction
ROS-driven apoptosis
decreased NO production
vasodiltion
increased shear stress
DNA damage causes what
increased apoptosis
ventricular dilation
with loss of cardiac myocytes, you lose contractility
impaired mitochondrial function causes what
apoptosis
decreased contractility
decreased ATP production
disrupts energy proteins
higher oxidative stress
release of proapoptotic factors
mtDNA damage
cardiomyocyte death causes what
decreased contractility
lose cardiac myocytes and replace with fibrosis
stiffer, acts as a load, harder to contract
endothelial dysfunction leads to what
increased apoptosis
ROS-driven apoptosis
decreased NO production
decreased vasodilation
increased shear stress
oxidized myofilaments effect
decreased contractility
oxidized RyR effect
Arrhythmias (AFib)
SR Ca2+ leak
quebec beer drinkers
almost 50 pts with acute sudden onset DCM
all alcoholics
stopped drinking and DCM regressed
did not appear to be alcoholic cardiomyopathy
what caused the cardiomyopathy in the Quebec alcoholics
quebec pts drank Dow beer
cobalt was in the beers to increase foam stability
cobalt created an acute and transient poison that caused DCM
how did cobalt cause cardiomyopathy
cobalt competes with magnesium and calcium (binds to binding sites)
disrupts enzymes for metabolism
effects not often seen with cobalt alone → require other issues like thiamine deficiency and alcoholism
alcoholics often thiamine deficient (poor diet and stomach damage limits uptake)
can you use alcohol to an advantage
yes, for hypertrophic cardiomyopathy
catheter inserted in femoral → guided to coronary artery… balloon inflated to block and alcohol is released… kills part of your heart you dont want (i.e. enlarged part) + it decreases, yes, damaged, but now blood can flow through aorta
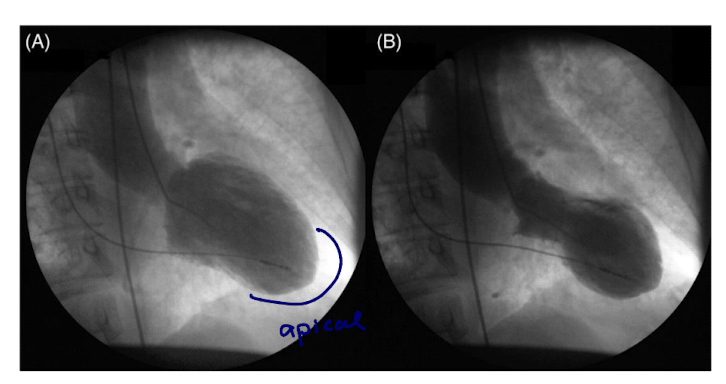
Takotsubo Cardiomyopathy
a stress induced, acute cardiac syndrome
stress is often emotional in origin
much more prevalent in women
apical akinesis is typical (apical region doesn’t move)
is takotsubo cardiomyopathy always associated with negative emotions
no, sometimes it can be triggered by a strong positive emotion
why does takotsubo cardiomyopathy occur
catecholamine surge targets heart (high local catecholamines)
B1 adrenergic receptors stimulated to increase contractility
B2 adrenergic receptors stimulated to decrease contractility
high concentration on B2 adrenergic receptors in apex
may allow for conditional depression of myocardium
there is a high concentration of which type of receptor in the apex
high concentration of B2 receptors in the apex
more even distribution of B1 and B2 in the basal region
what leads to apical region akinesis
the higher concentration of B2 receptors in the apex, leads to more of an inhibitory drive in the apex of the heart\
eventually, apical region will be depressed, leading to regional akinesis
what are B1 adrenergic receptors preferentially activated by
NE>E
40% more SNS fibers in basal area
neuro-NE preferentially stimulates basal contractilty
*Acute
B2-adrenergic receptors preferentially activated by what
E>NE
circulating E preferentially affects apical LV
chronic stimulation induces ‘stimulus trafficking’
as SNS fades, sustained drive comes from epinepherine
*Chronic
when active B1 and B2 usually both increase contractility, but in this case,
the B2s undergo this switching wheret he Gs is switched to Gi and now there is an active inhibition ny targeting myofilaments to reduce their contraction, targeting Ca2+ so it doesnt enter as much
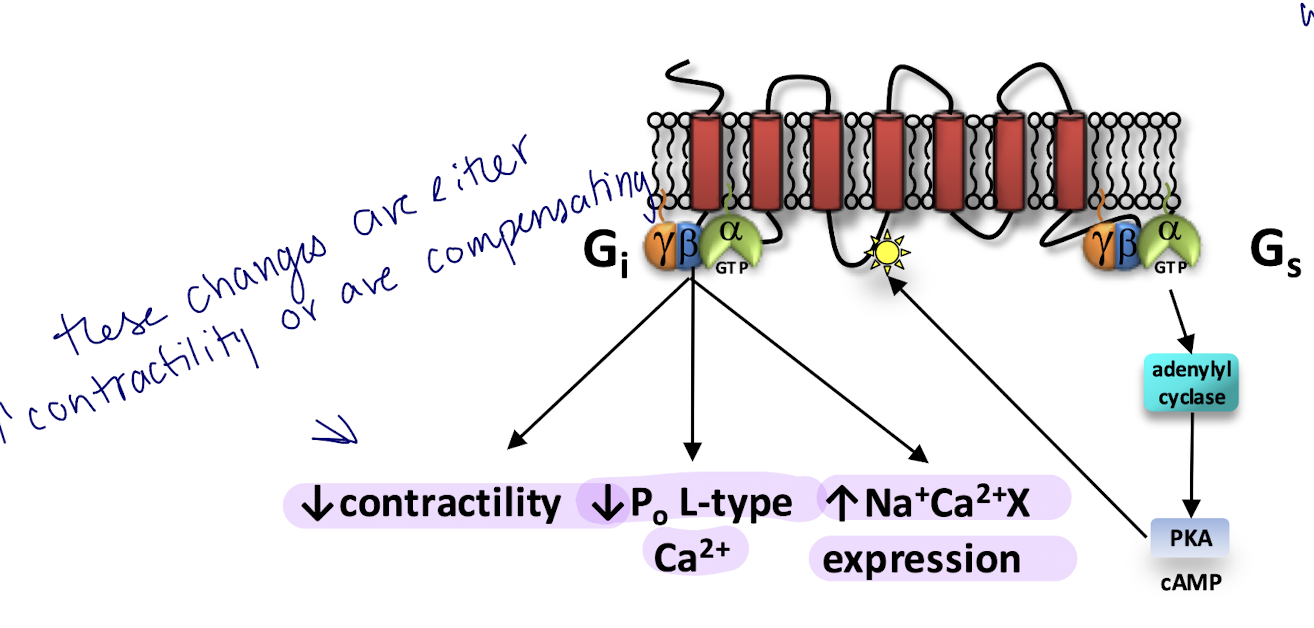
Gs activation does what
increases PKA activity
PKA phosphorylates B2-adrenergic receptor and couples to Gi
are B blockers the solution if B-adrenergic receptor overactivation is the problem
no, because if you block B1 + B2, you are removing inhibition (B1), but also removing stimulus (B2)
inconsistency in studies due to the type of B-blocker used
are they specific to B2 or not?
why else may B-blockers might not work
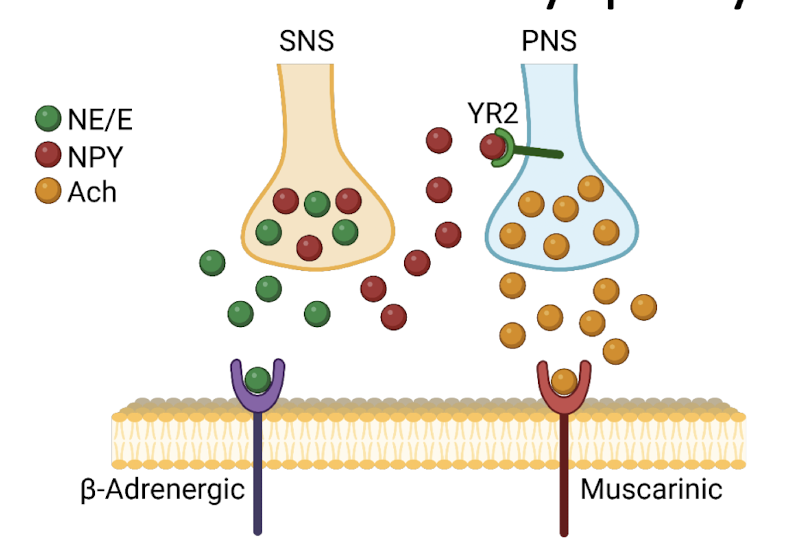
because there is an additional pathway,
SNS terminals release NE
high stimulation also release NPY (neuropeptide - Y)
high circulating levels of NPY (adrenals)
NPY activates PNS terminals to release Ach
Ach depresses contraction (binds to muscarinic receptors)
YR2 expression in apex (apical inhibition)
adrenal glands are still stimulated hours later - still releasing NPY - suppress contractility through muscariniwhatc receptors
what happens with takotsubo when you exercise
decreased phosphoreactive levels
thus, small decrease in energy supply (ATP)
when you exercise + place demand, pushes over edge + develop MI or HF
what is the rate of mortality 5 years after like
similar to that of MI
is takotsubo benign
mostly considered benign because few die and many fully recover
what is the magic number it takotsubo
10 days → if at 10 days HF is normal you will likely recover
if at 10 days not normal, may not fully recover