Lecture 3: Specific phobias
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
14 Terms
Fear responses and phobias look very similar on the outside. What is the difference?
Fear is a response to a danger. A phobia is triggered even when there is no danger present
What are common phobic objects?
•Animal (e.g., spiders, insects, dogs).
•Natural environment (e.g., heights, storms, water).
•Blood-injection-injury (e.g., needles, invasive medical
procedures)
•Situational (e.g., airplanes, elevators, enclosed places).
•Other (e.g., situations that may lead to choking or vomiting; in
children, e.g., loud sounds or costumed characters)
Conditioning (classical)
US (bite) = UR (fear)
CS (dog) = CR (fear)
What types of conditioned responses exist?
Physiological responses
Electromyography (EMG)
Skin conductance (SCR)
Subjective responses
Fear ratings
Expectancy Ratings
Behaviour
Avoidance/Freezing
Fear generalization
the spread of fear to
objects similar to the phobic object (e.g. all dogs)
What is a problem with conditioning models?
Neither necessary nor sufficient to explain phobias
No individual differences
Assumption that all stimuli can be
similarly conditioned
No direct experience needed
How can fear conditioning be a procedure, an effect and a mechanism?
Procedure (What is happening?)
Effect (What do we find?)
Mechanism (Why it is happening
What types of exposure therapy are there?
In vivo exposure
Virtual reality exposure
Imaginary exposure
(Interoceptive exposure - more used in treating PD)
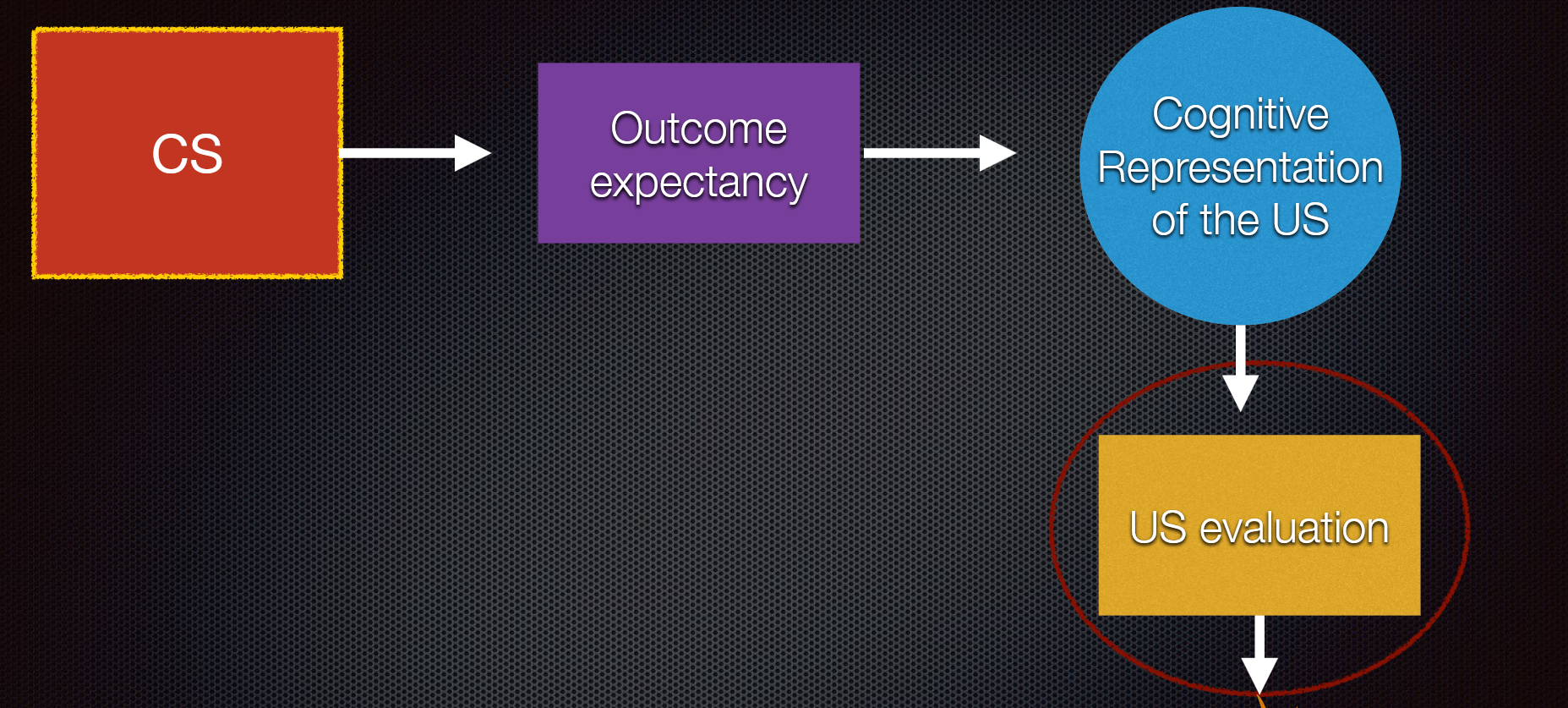
Explain this
In a phobia, the CS is associated with the US and thus there is an expectancy that the US will occur. The fear is caused by the expectation that the US will occur as well as the evaluation of the US as dangerous
What are the steps in exposure therapy?
(I) Intake
(II) Fear hierarchy
(III) Flooding (start with most fearful component) or desensitization (start with least
fearful component)
(IV) Behavioral Approach Task (With Response Prevention)
(V)Duration: Typically one long session (3h) or 3-5 shorter sessions (1h) are
sufficient
(VI) Pharmacological enhancement/support can be considered (e.g., when patients
is highly distress) (Maybe safety cue)
What are problems with in-vivo exposure therapy?
1.Treatment acceptance (e.g., Garcia-Palacios et al., 2001)
•75-85% of phobic patients do not seek treatment
•25% of patients who seeks treatment refuse exposure therapy
2.Drop-out
•0-45% drop-out rates (Choy et al., 2007)
3.Relapse
•19-62% of patients relapse after exposure therapy (Craske & Mystkowski, 2006)
What is
Spontaneous recovery
Reinstatement
Renewal
Rapid reaquisition
Spontaneous recovery: fear just coming back after a while
Reinstatement: Fear coming back after another encounter with the US
Renewal:the return of conditioned fear observed when the threat cue is encountered outside the extinction context
Rapid reaquisition: The phobia coming back quickly when CS and US are paired together
What did the study with propanolol find?
That providing people with a propanolol pill erased the behavioural activation of the fear memory 24 hours later, e.g. the fear memory was not remembered as being fearful
This could potentially be a factor in relapse rates
What did another study on propanolol find?
That the reconsolidation process was only disrupted if the patients who took propanolol encountered the feared stimulus 2 days (rather than 4 weeks) after the intervention