Chapter 11: Physical and Cognitive Development in Adolescence
1/30
Earn XP
Description and Tags
Discuss the nature of adolescence. Describe the changes involved in puberty, as well as the changes in the adolescent brain. Identify adolescent problems related to health. Explain cognitive changes in adolescence. Summarize key aspects of how schools influence adolescent development.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
Adolescence as a Social Construction
“Adolescence” is not a clearly defined physical or biological category; it is a social construction.
Historically, children entered the adult world when they matured physically or began a vocational apprenticeship.
In most parts of the world, adolescence lasts longer and is less clear-cut than in the past because puberty starts earlier and the amount of required training has increased for higher-paying occupations.
Adolescence and puberty
Adolescence is the developmental transition between childhood and adulthood entailing major physical, cognitive, and psychosocial changes.
Adolescence roughly encompasses the years between 11 and about 20.
An important physical change in adolescence is the onset of puberty, the process by which a person attains sexual maturity and the ability to reproduce.
Hormonal changes in puberty
Puberty begins with a cascade of hormonal responses.
The hypothalamus releases elevated levels of gonadotropin-releasing hormone, which in turn triggers a rise in luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
In girls, FSH leads to the onset of menstruation. In boys, LH initiates the release of two additional hormones: testosterone and androstenedione. Adrenarche occurs between ages 6 and 8. Adrenal glands secrete increasing levels of androgens that lead to the growth of body hair, faster body growth, and oilier skin.
In the second stage, gonadarche, the sex organs mature. A girl’s ovaries increase estrogen, stimulating growth of the female genitals, breasts, and body hair. In boys, the testes increase testosterone, leading to growth of the male genitals, muscle mass, and body hair.
Primary and secondary sex characteristics
The primary sex characteristics are organs directly related to reproduction. In the female, the sex organs include the ovaries, fallopian tubes, uterus, clitoris, and vagina. In the male, they include the testes, penis, scrotum, seminal vesicles, and prostate gland.
The secondary sex characteristics are physiological signs of sexual maturation that
do not involve the sex organs, such as the development of breasts in females and broader shoulders in males.
Adolescent Growth Spurt
The adolescent growth spurt refers to the rapid increase in height, weight, and muscle and bone growth that occurs during puberty.
It generally begins in girls at about age 10, and at about 12 or 13 in boys; it lasts about 2 years and ends with the young person reaching sexual maturity.
Sexual Maturity
Maturation of the reproductive organs brings about menstruation in girls and sperm production in boys.
For boys, the first ejaculation, or spermarche, occurs around age 13. It can be experienced as a nocturnal emission while sleeping.
For girls, menstruation is the monthly shedding of tissue from the lining of the womb. The first menstruation is called menarche and usually begins by age 12.5.
Timing of Puberty
There is a secular trend in the onset of puberty spanning several generations: a drop in the ages when puberty begins. A variety of explanations have been proposed, such as these:
•A higher standard of living and better nutrition may contribute.
•The role of body fat in triggering puberty is linked to rising obesity rates (what about starving oneself)
•Stress levels due to factors like being firstborn and harsh parenting practices may also be involved.
Adolescent Brain
Dramatic changes. STeady increase in white matter improving information-processing abilities.
Pruning continues, resulting in fewer but more effective neuronal connections.
Physical and mental health
About 1.2 billion people—1 in 6—are adolescents.
Across many countries, adolescents from less affluent families report poorer health relative to teens from more affluent families who have healthier diets and are more physically active.
Lifestyle patterns tend to solidify in adolescence, which may result in poor lifelong health habits and early death in adults.
Exercise
Only 26.1% of U.S. high school students
engage in the recommended amounts of
physical activity.
Regular exercise benefits teens in terms of improved strength and endurance, healthier bones and muscle,
weight control, reduced
anxiety and stress, and
increased self-esteem,
grades, and well-being.
Sleep Needs and Issues
Only about 25.4% of high school students get sufficient sleep every night.
By 12th grade, 75% of teens do not sleep a full
8 hours, which is problematic given that adolescents need as much sleep as when they were younger—or more.
Sleep deprivation causes irritability, and concentration and school performance suffer.
Obesity in adolescence
In low-, middle-, and higher-income countries, teens are increasingly becoming overweight and obese.
In the United States, approximately 15.6% of high school students are between the 85th and 95th percentile for body mass index (BMI).
Overweight teens tend to be in poorer health than their peers and are at heightened risk of hypertension, diabetes, and cardiac disease.
Culture across the world on obesity
Worldwide, obesity in children and adolescents has increased substantially; the prevalence has tripled since 1975.
Obesity has multiple causes including excessive sugar intake, increased portion sizes, and a decline in physical activity.
Common interventions include increasing physical activity, decreasing screen time, and promoting a healthy diet.
Body image and eating disorders
Body image refers to descriptive and evaluative beliefs about one’s appearance.
Sometimes a concern with
body image may lead to
obsessive efforts at weight
control.
Anorexia nervosa, or self-starvation, is potentially life threatening. An estimated
0.3–0.5% of adolescent girls and young women and a small but growing number of boys and men in Western countries are known to be affected.
Early warning signs include secret, determined dieting, dissatisfaction after losing weight, setting new, lower weight goals, excessive exercising, and interruption of menstruation.
Bulimia nervosa is an eating disorder in which a person regularly eats huge quantities of food and then purges the body with laxatives, induced vomiting, fasting, or excessive exercise.
The disorder affects about 1 percent of international populations.
People with bulimia are not necessarily overweight, but they are obsessed with their weight and shape and may become overwhelmed with shame and depression.
Treatment for eating disorders
The immediate treatment goal for anorexia is getting the patient to eat and gain weight. Treatments include:
•Behaviorally focused outpatient family therapy; and
•Admission to a hospital for 24-hour nursing.
Bulimia is often treated with medication and cognitive therapy. Patients keep daily diaries of their eating patterns and learn ways to avoid the temptation to binge.
Drug use and abuse
Most adolescents do not abuse drugs, but a significant minority do.
Substance abuse is the harmful use of alcohol or other drugs. Abuse can lead to substance dependence, or “addiction,” which may be physiological, psychological, or both, and is likely to continue into adulthood.
Trends in drug use
Nearly half of U.S. adolescents have tried illicit drugs by the time they leave high school.
In the past two decades, there has also been a general increase in opioid use. Use of legal narcotics peaked in 2002 and has been slowly declining since then.
The sharp rise in heroin use in the United States is primarily among older teens and emerging adults, where peak levels were reached in the mid-2000s.
Alcohol, weed, tobacco
Alcohol, tobacco, and marijuana use among U.S. teenagers showed a dramatic rise in the 1990s followed by a smaller, gradual decline.
Marijuana has followed the same pattern, but its usage has remained higher overall and showed slower declines.
Alcohol use is a serious problem in many countries. Approximately 27% of 15- to 19-year-olds across the globe report drinking alcohol. By the end of high school, 61.2% of American teens will have tried alcohol.
The majority of high school students who drink engage in binge drinking, which is consuming five or more drinks on one occasion. Teenage binge drinkers are more likely than other students to report poor school performance and to engage in other risky behaviors.
Marijuana is by far the most widely used illicit drugs in the United States. By the end of high school, students report a lifetime prevalence use of 44.5%.
Heavy use has been associated with damage to the brain, heart, and lungs. It has been correlated with declines in school performance, memory problems, and increased risk of anxiety and depression.
In the United States, currently 28.3% of
12th-graders report having tried cigarettes.
Tobacco use is on the decline in the United States and other industrialized countries, but the use of e-cigarettes is increasing.
Adolescents exposed to alcohol and drugs prior to age 15 are at an increased risk for substance abuse disorders, risky sexual behavior, and low educational attainment.
Depression
In 2017, 13.3% of children ages 12–17 experienced major depression; prevalence rates increase during adolescence.
Symptoms may manifest in adolescence as irritability, boredom, or an inability to experience pleasure.
Being female is a risk factor for depression. Other risk factors include anxiety, stressful life events, chronic illnesses, abuse or neglect, and alcohol and drug use.
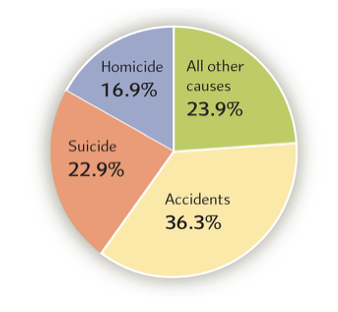
Death in Adolescence
The leading cause of death
among U.S. teens is motor
vehicle collisions, accounting
for one-third of all deaths
in adolescence.
Homicides and suicide are the second and third leading causes of death in the United States. Firearm-related deaths are far more common in the United States than in other industrialized countries.
Aspects of Cognitive Maturation:
Piaget’s Formal Operations
Adolescents enter what Piaget called the highest level of cognitive development, formal operations—the ability to think abstractly.
Around 11, children can use symbols to represent other symbols in algebra, interpret hidden messages, think in terms of what “might be” versus what “is,” and can form and test hypotheses.
Hypothetical-Deductive Reasoning
Piagets Hypothetical-deductive reasoning involves a scientific approach to problem solving that involves developing and testing hypotheses.
Piaget paid little attention to social and cultural influences or other cognitive advances like metacognition—thinking about thinking—which may be the chief advance of adolescent thought.
Language Development
In adolescence, vocabulary continues to grow; by ages 16–18, the average young person knows about 80,000 words.
With abstract thought, adolescents can define and discuss abstractions such as “love,” “justice,” and “freedom.”
Adolescents are more skilled at tailoring their speech: using simpler words when talking with a child, swearing among friends, and showing deference to adults.
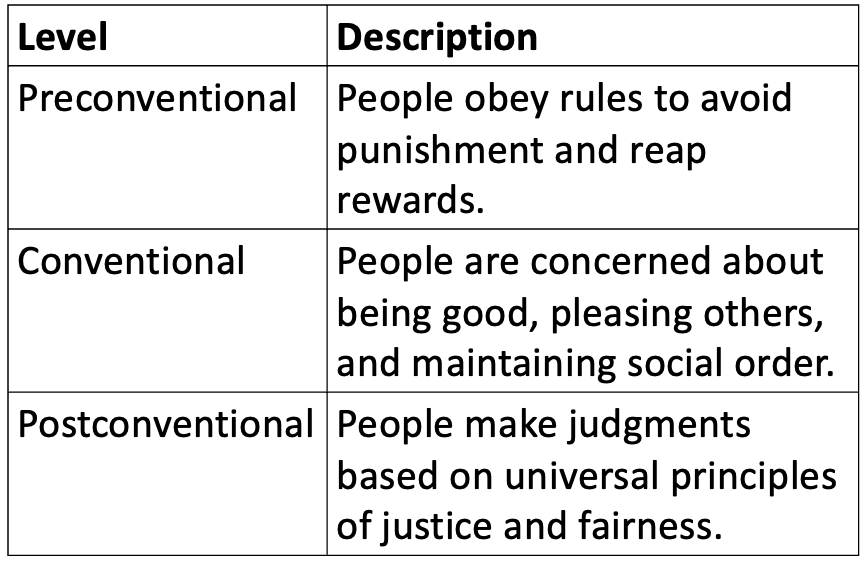
Kohlberg’s Stages of Moral Reasoning
Pre-conventional, conventional, and post-conventional. Each level has two stages that showing the evolution of moral reasoning from self-interest > adherence > societal rules > universal ethical principles.
Gilligans Ethics of care
Gilligan asserted that Kohlberg’s theory was sexist and oriented toward values more important to men than to women. Women, Gilligan argued, hold a different set of values that place caring and avoiding harm as higher goals than justice.
Research has found little support for Gilligan’s claim of a male bias; she has since modified her position. Gender differences in moral reasoning are small.
Prosocial reasoning and behavior
Prosocial behavior typically increases from childhood through adolescence.
Girls tend to show more prosocial behavior and empathic concern than boys, and this difference becomes more pronounced in adolescence.
About half of adolescents engage in some sort of community service or volunteer activity. Students who volunteer tend to be more engaged in their communities and see better academic and civic outcomes.
Student Motivation and Efficiency
Many U.S. students are not self-motivated, and motivation often declines as they enter high school.
However, students who have high self-efficacy—who believe that they can successfully achieve academic goals—are likely to do well in school.
Gender and School Achievement
Reading tests conducted on 15-year-olds in 72 countries shows an advantage for girls, although scores narrowed between 2009 and 2015.
Gender differences in science are small, but boys are more likely to be top performers in all countries with the exception of Finland.
Male and female brains show some differences in structure and organization. Social and cultural factors include home influences, school influences, and societal roles.
In 2017, the dropout rate was 5.4%, and it was higher for boys than girls.
Why are poor and minority adolescents more likely to drop out? Reasons include low teacher expectations, differential treatment, and less teacher support than at the elementary level.
Dropouts are more likely to be unemployed or to have low incomes, to end up on welfare, or to become involved with drugs, crime, and delinquency.
Teen Media Multitasking
More than 25% of adolescents’ media consumption occurs using at least two media types simultaneously.
Evidence suggests that adolescents are not producing high-quality work while texting with friends or listening to music. Media multitasking is associated with poorer academic performance and decreased working memory capacity. Using a cell phone while driving is comparable to driving while drunk.
Influences on student aspirations
How do young people develop career goals and decide whether to go to college?
•Influences include:
•Self-efficacy beliefs;
•Parents’ values;
•Gender-stereotyping;
and
•Preferences for analysis versus creativity.
Adolescents in the Workplace
In the United States, about 20% of students are employed during a given school year.
Researchers disagree over whether part-time work is beneficial to high school students (e.g., helping develop real-world skills) or detrimental (e.g., distracting them from long-term goals).
How much time students work matters: those who work more than 20 hours a week generally suffer academically and are more likely to drop out of school.