Module 3 - RV Systolic Dysfunction and Pulmonary Herat Disease
1/57
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
58 Terms
Name the views for imaging and assessment of the RV.
PSLAX
PSSAX
PF RV inflow
Apical 4C
Focused apical 4C
Modified apical 4C
Subcostal views
Compare modified 4C vs focused 4C.
Modified: assess RV wall function and TR Doppler
Focused: measure RV diameter and show true structure of RV
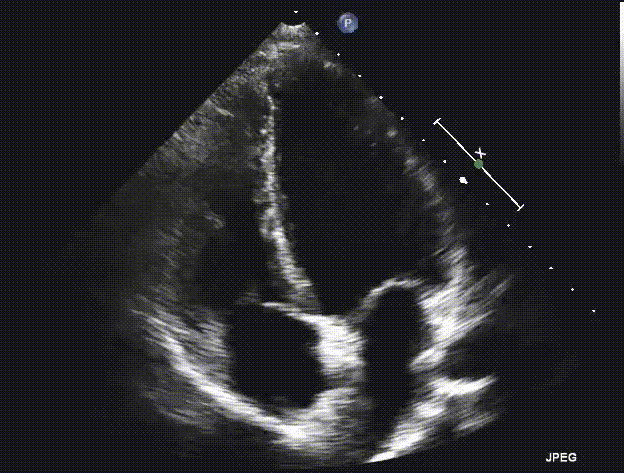
Identify this view.
RV focused apical 4C.
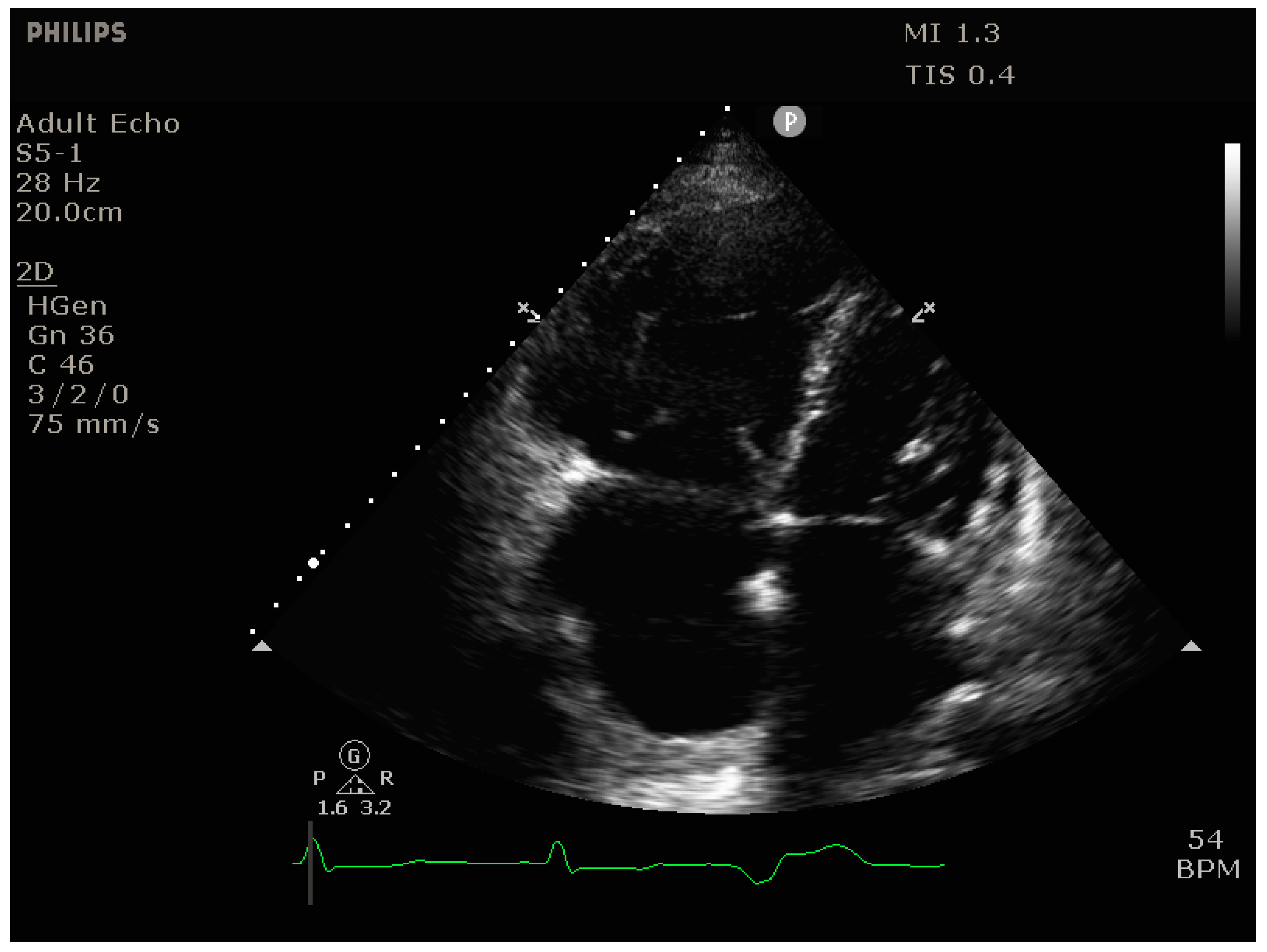
Identify this view.
RV modified apical 4C.
Explain the process of obtaining RV linear measurements.
All measured during diastole.
From RV focused apical 4C, make one longitudinal measurement from annulus to apex and horizontal measurements at the basal and mid walls.
From PSLAX, measure RVOT.
From PSSAX, measure RVOT proximal and RVOT distal.
Explain how to measure RV EDWT.
From SC 4C, zoom on the RV lateral wall and measure.
Explain how to measure TAPSE.
From apical RV focused 4C, place the M-mode cursor through the lateral tricuspid annulus. Measure the slope of the lateral annulus from end-diastole to mid-systole.
Describe how TDI can be used to measure RV function.
Derived tricuspid lateral annular systolic velocity.
RV TDI can assess S’ velocity by moving the cursor through the lateral annulus in RV focused 4C.
Explain how to measure FAC.
From RV focused apical 4C, trace the endocardial border in end-diastole and end-systole. Ignore trabeculations and the moderator band.
Wat does FAC stand for? What does it measure?
Fractional area change.
Measures the overall wall motion of the RV.
Provide some examples of qualitative measurements of the RV.
RV enlargement (RV>LV)
Wall motion abnormalities
Provide some examples of quantitative measurements of the RV.
RV linear dimensions
RV TDI S’`
TAPSE
FAC
Define end-organ consequence.
Organs supplied by the circulatory system suffer damage from hypertension.
Why is aging a risk for hypertension.
Progressive stiffening and loss of compliance in arteries.
What does it mean when a disease is “primary” vs “secondary”?
Primary - unknown etiology
Secondary - identified cause
Explain how renal disease can cause secondary hypertension.
Kidneys regulate blood volume. When kidneys are dysfunctional, blood volume increases → increased BP → damage to the arteries → cardiovascular disease.
List some common echo findings with renal disease.
Hypertension
LVH
Pericardial effusion
Describe the myocardial remodeling progression of the LV due to HTN.
LVH → diastolic function impaired, systolic function preserved
Ventricular dilation → diastolic function better but still impaired, systolic function impaired
List some common echo findings with systemic HTN.
LVH
Diastolic dysfunction
LA dilation
Systolic dysfunction
Valve disease
What are the 4 parameters required to assess LVH?
Septal and posterior wall thickness
RWT
LVM/BSA
LV geometry
How does the LV remodel in response to ↑Pr? How is this beneficial but decompensatory?
Increases wall thickness → ↑concentric force
Reduces wall stress but decreases compliance.
How does the LV remodel in response to ↑volume? How is this beneficial but decompensatory?
Dilates → accommodate larger volumes
Increases compliance but decreases systolic function.
In concentric hypertrophy, sarcomeres are added…
In parallel
In eccentric hypertrophy, sarcomeres are added…
In series
Describe the geometry of LV eccentric hypertrophy.
Dilated LV.
Describe the geometry of LV concentric remodeling.
Increased RWT.
Describe the geometry of LV concentric hypertrophy.
Dilated LV with increased RWT.
Describe the Doppler patterns found in a patient with grade 1 hypertension.
Diastole is impaired but presents with a pseudonormal pattern because of ↑LAP.
MV PW is normal in appearance.
TDI shows ↓E’/A’.
Describe a situation where you might observe hyperkinetic LV walls.
Hypertrophic cardiomyopathies to preserve EF.
List some common valvular diseases associated with systemic HTN.
MR
MAC
AR
Ao root dilation
List some examples of secondary pulmonary heart disease.
Diseases that cause elevated pulmonary venous pressure
Intrinsic lung disease
Acute and chronic pulmonary embolism
Intracardiac shunting.
Describe the initial compensatory mechanism for chronic pulmonary HTN. Describe how this becomes decompensatory and the subsequent effects on the rest of the heart.
Initial - RV hypertrophy to preserve RV systolic function.
Becomes decompensatory as the RV dilates to preserve diastolic function.
Leads to TR, RA enlargement, and elevated PAP.
Describe how pulmonary HTN causes RA enlargement.
RV dilates → ↑TV annulus size
TR → ↑volume in RA
Define cor pulmonale.
Right sided heart failure.
Name the 2 components of cor pulmonale and the symptoms associated.
Chronic pressure overload (RVPO)
Increased RV afterload
Symptoms:
Dyspnea
Syncope
Peripheral edema
Jugular vein dilation
List some echo findings that could indicate pulmonary HTN.
Elevated RVSP
Signs of RVPO (↑RVFWT, paradoxical septal motion)
TR
RA enlargement
Pulmonary flow mid-systolic notch
Name the most reliable method to estimate PAP.
RVSP
What variables are needed during an echo to calculate RVSP?
Peak TR jet
IVC diameter
Collapsibility index

Estimate RVSP when:
Peak TR jet = 5.0m/s
IVC diameter = 1.9cm
IVC collapse <50%
RAP = 8mmHg
RVSP = 4V2 + RAP
RVSP = 4(5.0m/s)2 + 8mmHg
RVSP = 4(25) +8mmHg
RVSP = 100 + 8mmHg = 108mmHg
List signs of RVPO on echo.
RV dilation
↑RVFWT
Paradoxical septal motion
Describe and explain septal motion in a patient with RVVO.
The LV has a D shape in diastole.
Increased volume in the RV pushes the septum flat but LV roundness is restored during systole.
Describe and explain septal motion in a patient wit RVPO.
Paradoxical septal motion: the LV has a D shape in diastole and systole.
Increased pressure in the RV pushes the septum flat in diastole and systole.
Describe how mild, moderate, and severe RV enlargement is qualifiable.
Mild RVE: RV < LV but dilated
Moderate RVE: RV = LV
Severe RVE: RV > LV
How is RV hypertrophy measured?
RVFWT
List some causes of RVH.
Pulmonary HTN
Pulmonary stenosis
Cardiomyopathy
TR is secondary to…
Pulmonary HTN
RV dilation
RV systolic dysfuction
List some expected consequences of severe TR and how they are assessed in echo.
Systolic flow reversal in IVC and HV - large a-wave reversal in HV PW
RA dilation - compare to LA size and RV size
Name a imitation to assessing a large TR jet on echo.
Because of the larger area for blood to travel through, regurgitant volume is dispersed, not well visualized, and the peak velocity will be underestimated (underestimate RVSP).
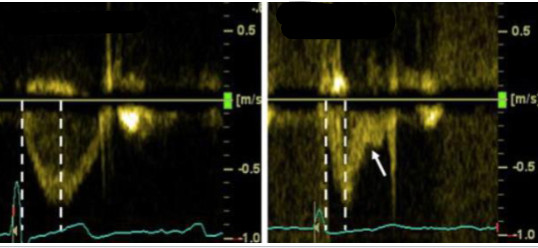
Compare these two tracings of the same valve on different patients. What valve is being measured? Which is normal and which is abnormal? What does the abnormal tracing indicate?
PV PW.
Left is normal with normal acceleration time, peak in the middle of the waveform, and appropriate deceleration time.
Right is abnormal with shortened acceleration time, an early peak, and a mid-systolic notch. These are indications of pulmonary HTN.
Explain why a PV mid-systolic notch may occur in the spectral tracing.
The PV starts closing because the RV pressure and PAP equalize but the RV is still contracting - generates enough pressure to push the leaflets open again.
What condition causes acute pulmonary HTN?
Pulmonary embolism.
List some indirect signs of pulmonary embolism on echo.
Elevated PAP
Acute RVPO
RV dilation and dysfunction
TR
Explain McConnell’s sign. What does it indicate?
Regional RV dysfunction:
Mid RV free wall is akinetic - ↑wall stress → ↓perfusion
RV apex is hypercontractile - proximity to RV apex offloads some wall stress to the LV
Indicates pulmonary embolism.
What happens to a patients clinical status if pulmonary embolism is left untreated.
Pulmonary embolism → ↑PAP → ↑RV afterload → RV dilation → RV dysfunction → ↓RV CO → ↓LV preload → ↓LV CO → hypotension
Echo is an effective way to monitor thrombolytic therapy. Within several hours, after thrombolytic therapy or suction embolectomy, echo demonstrates:
Reversal of RV size to normal
Reversal of RV dysfunction to normal
A patients requestion includes suspicion of pulmonary HTN. What are some observations/measurements you want to make during an echo to investigate?
RV size and function
FAC
TAPSE
S’
RVFWT < 5mm
RA size and volume
Paradoxical IVS
RVSP
IVC dilation
TR
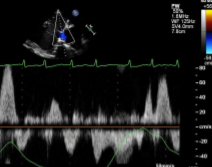
Given this HV PW trace, what would you expect to find when imaging the heart?
Elevated A-wave reversal
Expect to see:
↑RAP
RA enlargement
TR
RV dysfunction
RVVO or RVPO
Define thromboectomy.
Surgery to remove a blood clot from an artery.