Insomnia, Drowsiness and Fatigue
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
Presentation of Insomnia
Difficulty falling sleep
Frequent awakening with difficulty falling back asleep
Early morning awakening with difficulty falling back asleep
Disturbed quality of sleep with unusual or troublesome dreams
Poor sleep in general
Impaired daytime functioning
Duration of sleep may be normal compared to average, but it may taken them longer to fall asleep
Quality of life is negatively impacted
Other: fatigue, drowsiness, anxiety, irritability, depression, decreased concentration, memory impairment.
Exclusions for Self Care
<12 years
> 65 years of age
Pregnancy
Frequent nocturnal awakenings or early morning awakenings (may be associated with depression)
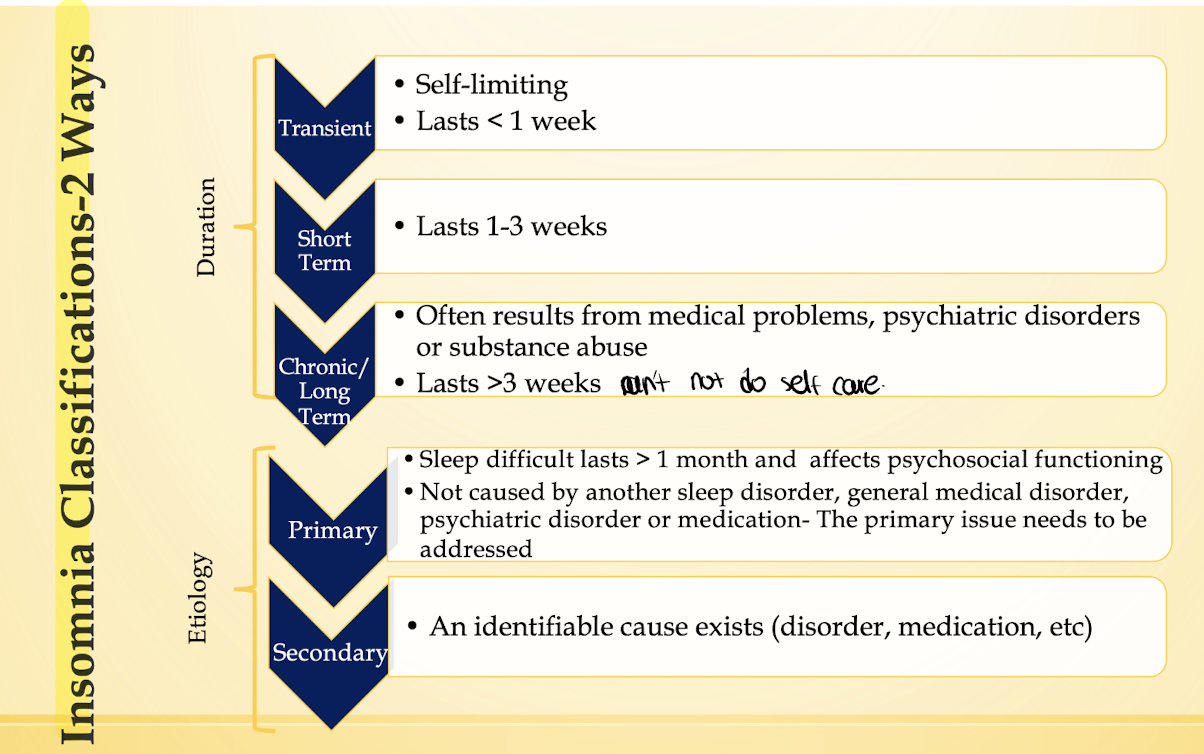
Chronic insomnia > 3weeks (OTC options aren’t generally helpful)
Sleep disturbances secondary to psychiatric or general medical disorders
Treatment goals
Improve duration and quality of sleep
reduce fatigue and drowsiness during the day
Improve daytime functioning
Minimize adverse effects of treatment
Improve the pateint’s presenting symptoms
Improve quality of life
Nonpharmacologic treatment
Recommended for transient and short-term insomnia with no underlying medical or psychiatric conditions that cause insomnia
sleep hygiene
Establish a normal sleep cycle: go to bed and wake up at the same time every day, including weekends
Make the bedroom comfortable for sleeping
Engage in relaxing activities before bed
Use bed for sleep and intimacy only
Avoid caffeine, alcohol and nicotine 4-6 hours before bed
Exercise regularly but avoid late-night exercise (2-4 hrs before bed)
Eat a snack if hungry but avoid late-night heavy meals 2 hrs before bed
Avoid daytime napping
Remove environmental distractions (noise, lighting, uncomfortable temperatures, new surroundings)
Don’t lay in bed if unable to fall asleep, get up and perform a relaxing activity until tired
Do not watch the clock
Pharmacologic Treatment: Diphenhydramine MOA
MOA:Competes with histamine for H1-Receptors sites on effector cells in the gastrointestinal tract, blood vessels, and respiratory tract; anticholinergic and sedative effects are also seen
Indication
Symptomatic management of transient and short-term sleep difficulty (particularly sleep latency)
Use of diphenhydramine as a sleep aid should be limited according to the 2017 American Academy of Sleep Medicine (AASM) guidelines
Dosing
50 mg at bedtime, some patients benefit from 25 mg at bedtime
After 3 days take an “off” night to assess sleep
Tolerance develops ~ 4 days
Use for no more than 7- 10 consecutive nights as insomnia
may be secondary to a serious medical or psychiatric conditi
Pharmacologic Treatment:Diphehydramine Side effects
Anticholinergic: dry mouth/ throat, constipation, urinary retention, blurred vision and tinnitus; anticholinergic toxicity may occur
Drowsiness
Drug interactions
Other medications that can cause drowsiness→2D6 inhibitor
Kinetics
Max sedations in 3-6 hours after the dose
Half-life is 2.4-9.3 hours
Anticholinergic side effects
Salivation
Lacrimation
Urination
Defecation
can pee cant see cant spit cant shit
Pharmacologic Treatment: Diphenhydramine
Counseling Points
Avoid driving, cooking,operating heavy machinery until they know they are effected
Do not drink alcohol while taking
Paradoxical excitation may occur (most frequent in children, elderly, those with mental illness
Contraindications
Older men with BPH and trouble urinating
Angle-closure glaucoma
Patients with angina or arrhythmias
Patients with decreased cognition/dementia
1st Generation Antihistamines
Doxylamine→ safety and efficacy as a sleep aid not fully established
First Generation Antihistamines often cause drowsiness!The side effects seen are similar to those common with diphenhydramine- Anticholinergic
Pharmacologic Treatment: Doxylamine& Ethanol
Doxylamine
Safety and efficacy have not been fully established
Commonly available in sleep aid products
DO not recommend - less efficacy data than diphenhydramine
Ethanol
Commonly used by patients to induce sleep
Associated with hazardous drinking
Initially improves sleep in patients who do not abuse alcohol
High dose:sleep disturbances occur in the second half of the night
Tolerance develops quickly→leads to using higher doses
Chronic uses causes disorganization of sleep, restless sleep, reduced sleep duration
Present in some OTC products (10%)
Pharmacologic Treatment CAM - Melatonin- Strongest Evidence
Benefits are limited -May be effective for some types of insomnia
Usual dose is 0.3-5 mg at bedtimes (30 minutes prior)
AASM data based on 2 mg
Conflicting data
BEST evidence seen in patients with neurological disorders, elderly, depression or jet lag
Pharmacologic Treatment CAM 5-Hydroxytryphan (5-HTP)
Immediate precursor to serotonin
Efficacy is not established; May be linked to eosinophilia-myalgia syndrome (EMS)
Do not recommend
Pharmacologic Treatment CAM Valerian (valeriana officinalis)
Limited benefit
Trials have used doses of 400-900 mg
Continuous nightly use for days- weeks is needed for effects (not useful in acute insomnia)
withdrawal can occur when large doses are taken for many years, discontinue slowly via taper
Pharmacologic Treatment CAM Kava
Associated with serve hepatotoxicity
do not recommend
Chamomile, ginseng, lavender, hops, lemon balm, passion flower
Inadequate evidence
Special Populations insomnia
Pregnancy
Benefit vs. risk→refer to medical provider
Diphenhydramine: pregnancy catergory B
Breastfeeding
Increased risk CNS effects in breastfed infants whose mothers ingest sedating antihistamines
Use of low dose after daytimes feeding may lessen the effects
Drowsiness can be seen in infants whose mothers ingest larger doses of sedating antihistamines for sustained periods
Special populations continues insomnia
Children/ Adolescents:
May present with insomnia secondary to circadian rhythm disorder
Use behavioral interventions/ sleep hygiene first
Diphenhydramine/ doxylamine are not indicated for insomnia in children <12
Diphenhydramine may cause paradoxical excitation in younger children
Do not use both oral and topical diphenhydramine in children (toxicity)
Teenagers:
Ask about use of caffeine/ alcohol
Older Adults:
▪ Beers criteria recommends avoiding anticholinergics in older adults
▪ Diphenhydramine may cause cognitive impairment/ falls -> refer to medical provider
Patient Counseling
Practice good sleep hygiene-this may resolve insomnia on its own!
▪ Review the dosage guidelines and duration of therapy if recommending a pharmacologic option
▪ Review adverse effects, drug interactions, precautions and warnings for
recommended pharmacologic options
▪ Educate on the signs and symptoms that indicate the patient should see their provider (i.e. sleep has not improved within 10 days)
▪ Discourage the use of more than 1 concomitant pharmacologic insomnia option (due to increased risk of adverse effects)
▪ AASM’s weak recommendation against the use of diphenhydramine for treatment of sleep-onset and sleep-maintenance insomnia is based on low-quality evidence in patients receiving 50 mg doses
Drowsiness and Fatigue Basics
▪ Most often caused by inadequate sleep (duration and quality)
▪ increase risk of workplace and transportation accidents-
▪ increase accidents in drivers who report <7 hours of sleep per night
▪ Adversely effects on mood, productivity, and overall health
▪ May affect 22% of the population
Caffeine
▪ The most commonly used stimulant worldwide
▪ Average caffeine intake is 227 mg daily
▪ Caffeine is in multiple OTC drugs, Rx drugs, dietary
supplements and beverages
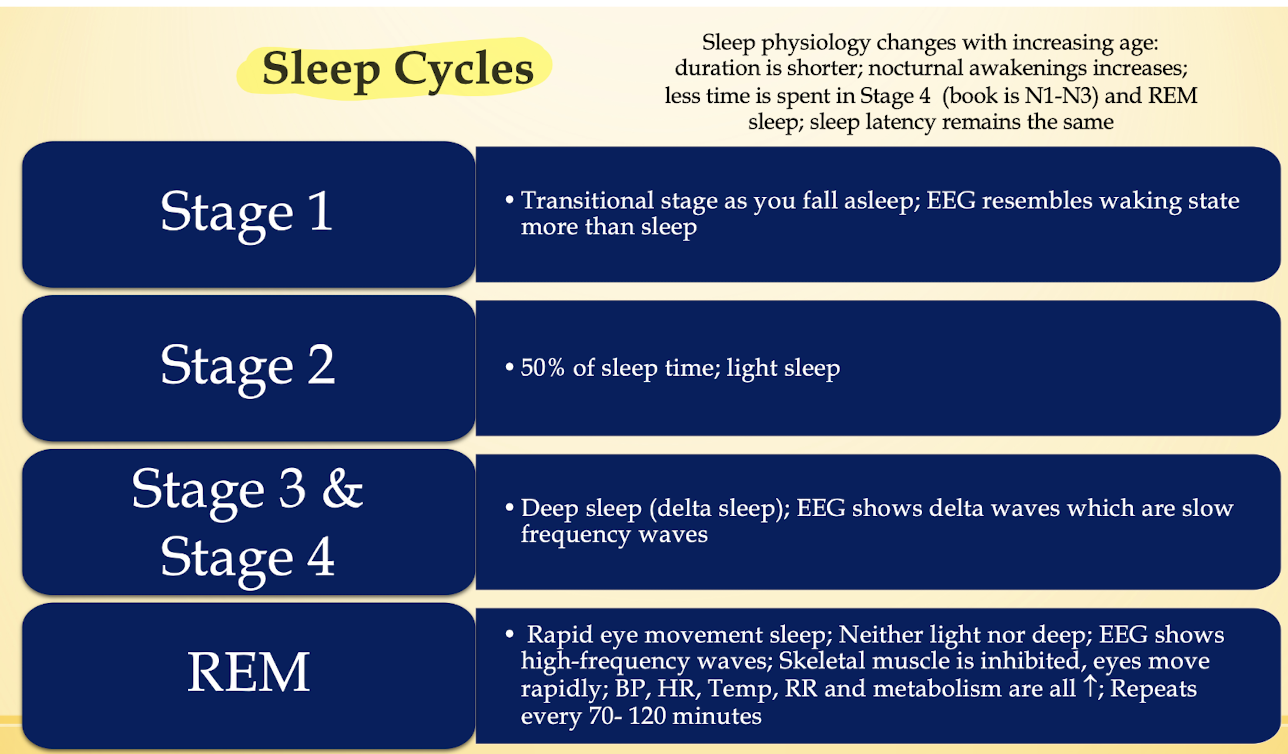
Sleep and Wakefulness
Sleep and wakefulness is affected by
1. Homeostatic mechanisms
2. Circadian rhythms
3. Medications
▪ CNS depressants, benzodiazepines, hypnotics, antihistamines,
antipsychotics, antidepressants, mood stabilizers, alcohol,
anticonvulsants, opioids, dopamine agonists, antibiotics, antihypertensives
4. Diseases
▪ Depression, cancer, anemia, hypothyroidism, chronic pain, overexertion,
imbalances in diet/ exercise
Presentation of Drowsiness and Fatigue
Sleepiness
Yawning
Eye rubbing
Tendency to fall asleep
Decreased ability to focus and concentrate.
Exclusions for self Care
▪ <12 years of age
▪ Pregnancy
▪ Breastfeeding
▪ Heart disease
▪ Anxiety
▪ Medication-induced drowsiness (refer to prescriber for dose adjustment)
▪ Chronic fatigue (refer to PCP to rule out hypothyroidism, sleep apnea, other
medical conditions)
Treatment Goals
▪ Identify and eliminate the underlying cause
▪ Improve mental alertness and productivity
▪ Maintain wakefulness
Nonpharmacologic treatment for drowsiness and fatigue
Sleep Hygiene
See insomnia
Pharmacologic Treatment: Caffeine
▪ Caffeine cannot compensate for inadequate sleep!!!
▪ MOA: Increases levels of 3'5' cyclic AMP by inhibiting phosphodiesterase; CNS stimulant which increases medullary respiratory center sensitivity to carbon dioxide, stimulates central inspiratory drive, and improves skeletal muscle contraction(diaphragmatic contractility); prevention of apnea may occur by competitive inhibition of adenosine
▪ Indication
▪ Occasional use to restore mental alertness or wakefulness
▪ Low-moderate caffeine doses increase arousal, decrease fatigue and elevate mood; High
doses are associated with anxiety, nausea, and nervousness
▪ Dosing
▪ 100- 200 mg every 3-4 hours as needed; rapid tolerance is seen
Pharmacologic treatment Caffeine
Side Effects
▪ Withdrawal may occur with abrupt discontinuation, symptoms include throbbing headache, fatigue, decreased alertness, drowsiness, depressed mood and irritability
▪ Aggravation of peptic ulcer disease (PUD), gastric reflux and esophagitis
▪ Increase in blood pressure and heart rate
▪ Increased risk of kidney stones in at risk patients
▪ Delayed sleep onset
▪ Drug Interactions
▪ Cigarette smoking may increase the clearance of serum caffeine (1A2) by >50%
▪ What do you need to tell someone who is trying to quit smoking?
▪ Table 8 -> additional drug-drug interactions
▪ Kinetics
▪ Peak concentration in 30- 75 min
▪ Elimination half-life is 3- 6 hrs
Pharmacologic Treatment: Caffeine
Contraindications
▪ Patients taking monoamine oxidase inhibitors (MAOIs)
▪ Patients with existing coronary artery disease (CAD)
▪ Uncontrolled hypertension
▪ Preexisting arrhythmias
Additional Counseling
▪ Caution use of dietary supplements and weight-loss supplements which often do not list
caffeine amount
▪ Symptoms of excessive intake
▪ Irritability, tremor, rapid pulse, dizziness and heart palpitations
Pharmacologic Treatment-CAM
▪ Ginseng
▪ Contradictory evidence exists regarding ginsengs ability to boost mental and physical energy
▪ Strongest evidence for Chronic Fatigue Syndrome (not a self-care condition)
▪ Cola nut, guarana, yerba mate
▪ Often found in caffeine-containing dietary supplements
▪ Risk of additive adverse effects and toxicity when taken in excess
Special populations
Pregnancy
▪ Caffeine: pregnancy category B; Freely crosses placenta
▪ Moderate consumptions ≤ 200 mg/ day is acceptable
Breastfeeding
▪ Consume caffeine in small-moderate amounts, preferably after breast-feeding to reduce infant exposure
Children
▪ More susceptible to cardiovascular and CNS effects
▪ Maximum recommended intake is 2.5 mg/kg/day
▪ Nonprescription caffeine products are not indicated for children <12 years of age
Older adults
▪ Elimination half-life of caffeine is prolonged
▪ May experience an exaggerated pharmacologic effect and sleep interference-Avoid after dinner
Patient counseling
▪ Practice good sleep hygiene
▪ Eliminate factors that interfere with normal sleep
▪ Review dosage guidelines for caffeine products
▪ Review adverse effects, drug interactions, precautions and warnings for caffeine products including irritability, tremor, rapid pulse, dizziness and heart palpitations (especially in older adults)
▪ Educate on the signs and symptoms of caffeine withdrawal
▪ Excessive sleepiness is a warning of inadequate sleep which is potentially LIFE THREATENING
▪ Educate on the signs and symptoms that indicate the patient should see their provider (i.e.increased pulse, headache, anxiety, etc)