L9: Pons extended version
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
69 Terms
hering’s law of equal innervation
yoked muscles have equal innervation - 2 eyes
ex:
left lateral rectus stimulated
right medial rectus is stimulated equally
sheringtons law of reciprocal innervation
antagonist muscles in the same eye recieve equal and opposite innervation
position of eyes at rest and why
straight ahead
bc they have tone due to intact innervation
nucleus propositus hypoglossi
neural integrator for horizontal movements
helps keep eyes still along horizontal
medulla
what has to work for normal lateral gaze
muscles
ipsilateral LR
contralateral MR
Nerves
CN 6 - LR
CN 4 - MR
Nuclei
Brainstem
MLF - interconnects nuclei of 6 and 3
PPRF
cerebral cortex
frontal eye fields
corticobulbars
lesion of L CN 6
left eye doesnt turn out - eso
6 nerve palsy
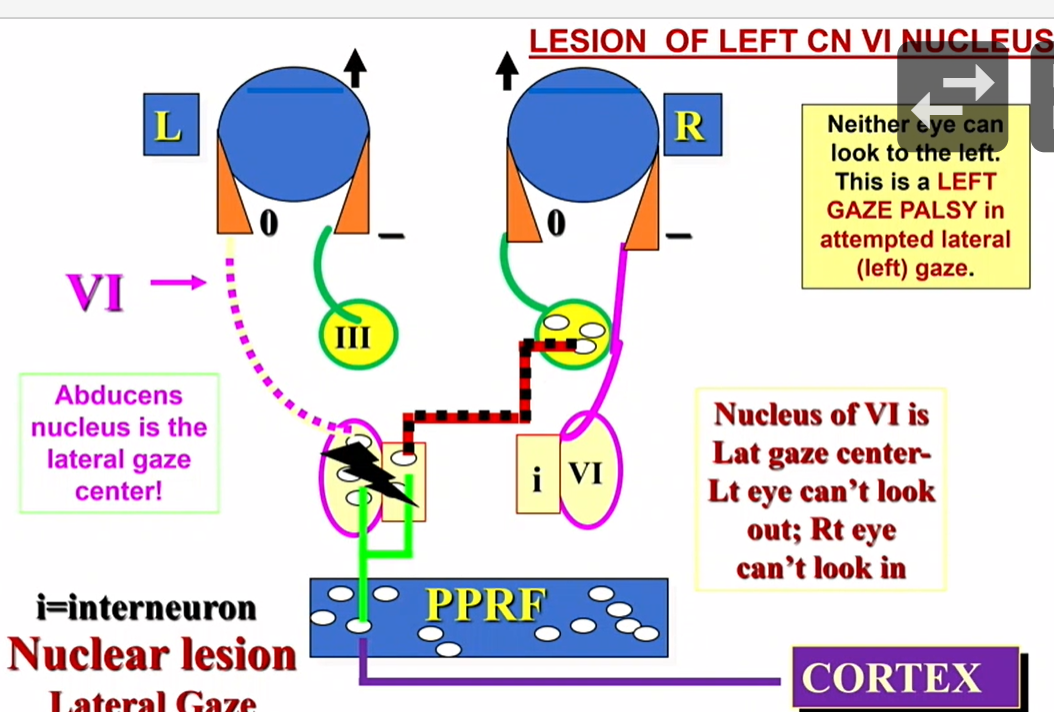
if you damage CN 6 nucleus do you get an abduction deficit
no
lateral gaze center = gaze palsy
damage to what causes an abduction deficit
abducens nerve
what things other than a CN 6 palsy could cause an abduction deficit
damage to lateral rectus
damage to NMJ (myasthenia gravis)
etc
what does raymonds syndrome affect
6 and contralateral hemplegia
gets CN 6 - ipsilateral abduction
also corticospinals - above crossing
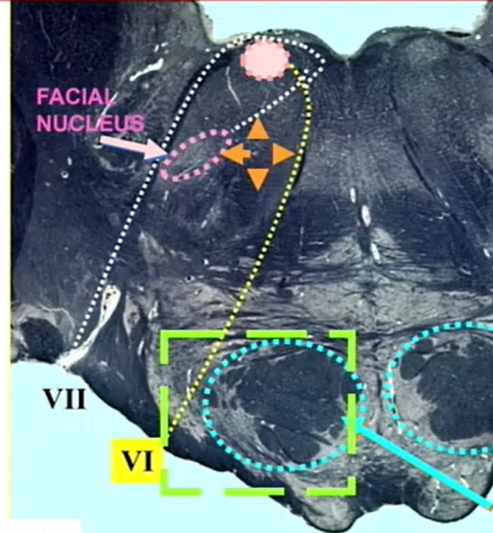
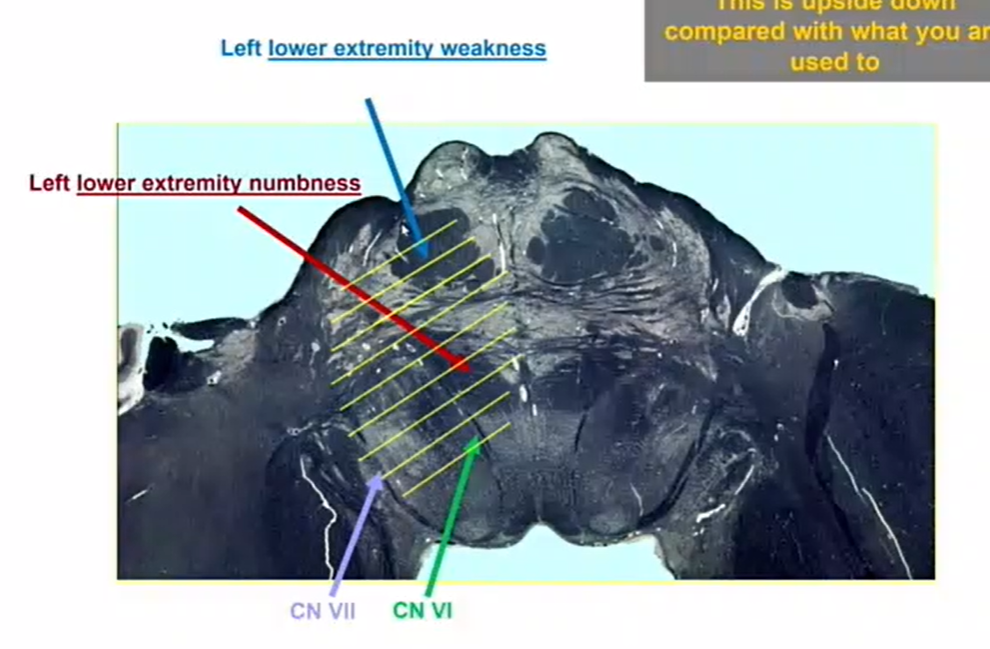
what is this green box a lesion of
raymonds syndrome
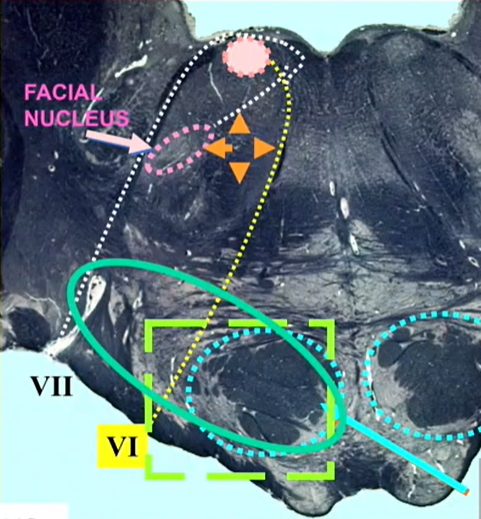
what does aqua oval cause
millard gubler syndrome
millsard gubler syndrome
6 - ipsalateral abduction
7- ipsilateral, LMN
contralateral hemiplegia
lesions dorsally (tegmentum) can get ________
CN
- likely to get sensory pathways
lesions ventrally can get
CN
mote likely to get vol motor pathways
LMN of 7 affects (top/bottom) face
all
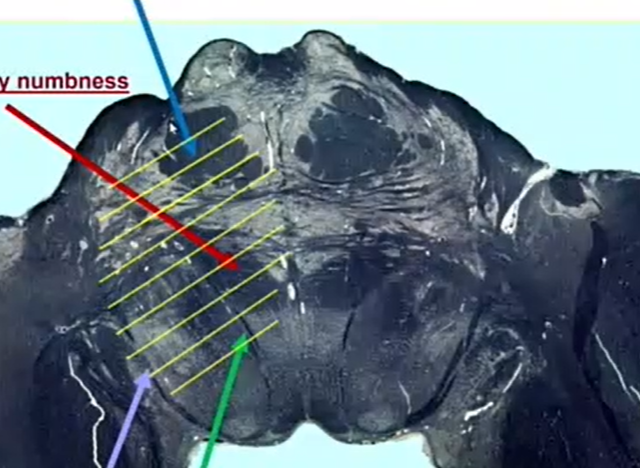
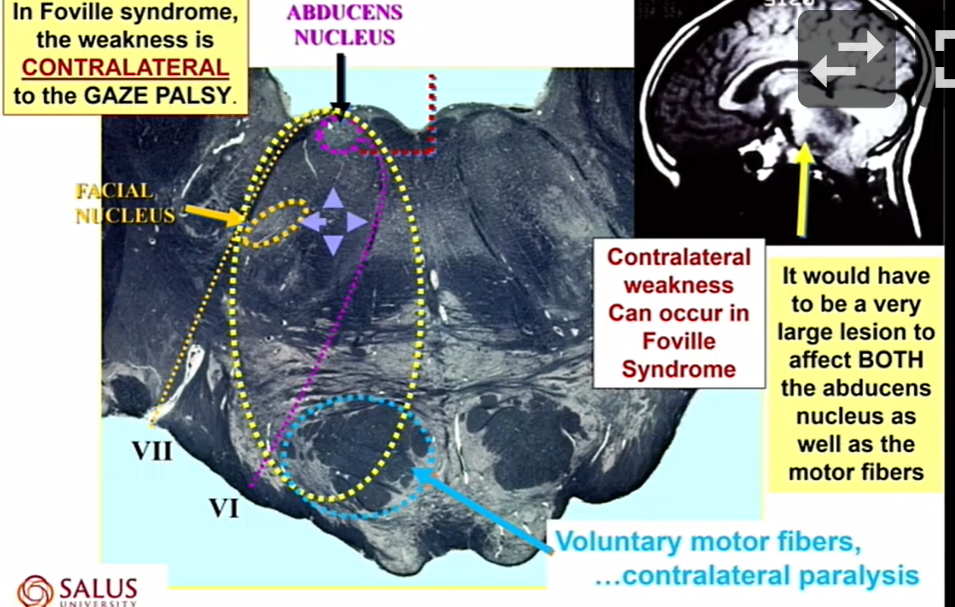
what does this lesion cause
numbness is bc of red sensory fibers
weakness is from corticobulbars
its upside down
what is prepontine cistern a part of
subarachnoid space
could get a meningioma
what is in the subarachnoid space that could damage CN 6
blood vessels
Anterior inferior cerebellar arery
labrynthine artery
(blood vessels)
all CN transverse the ___________
subarachnoid space
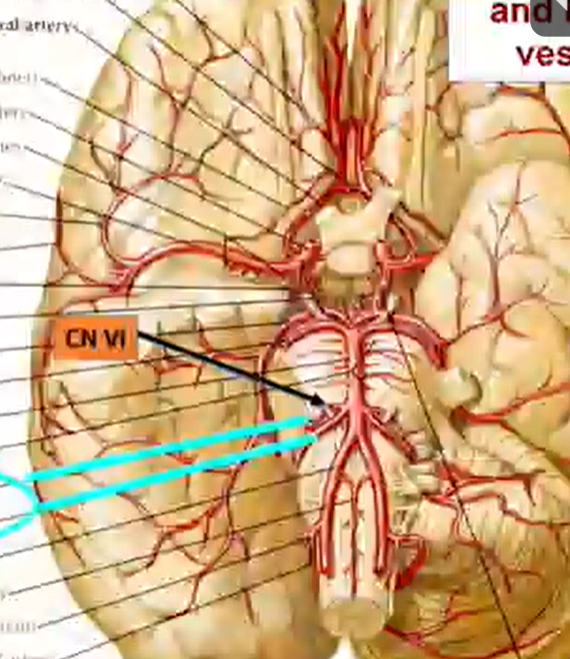
name the arteries that travel near CN 6
Anterior inferior cerebellar arery
labrynthine artery
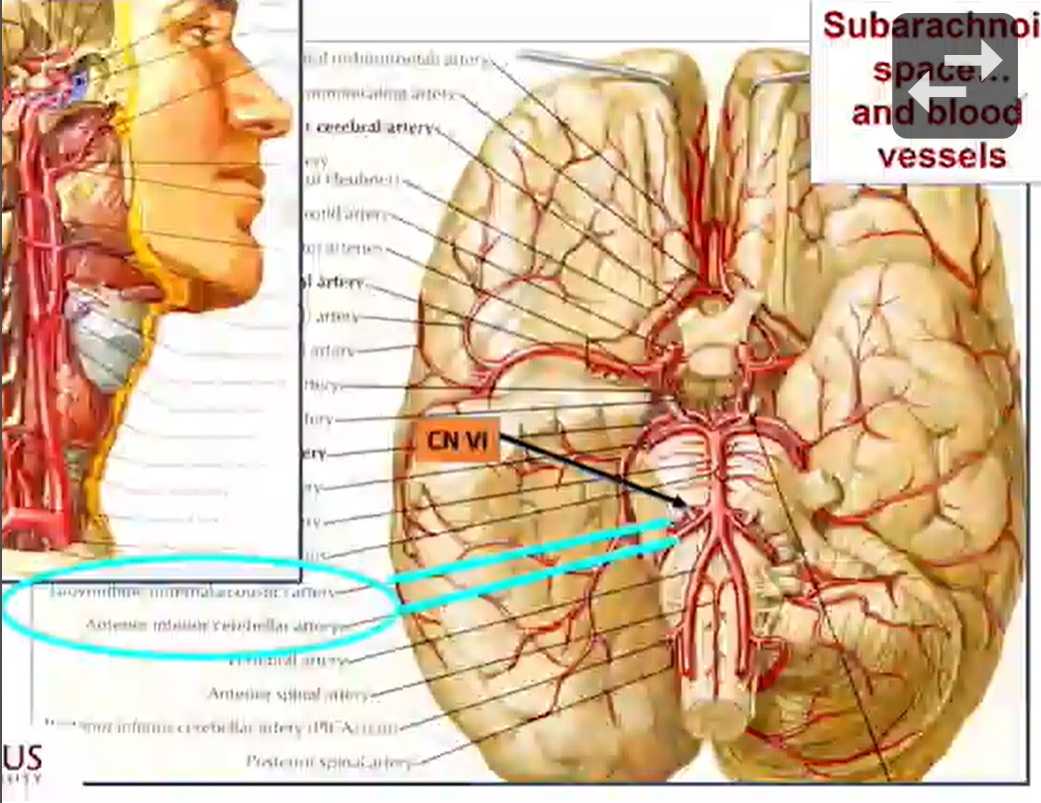
where are the arteries that come near CN 6
cerebellar pontine artery
what CN could be involved in a cerebellopontine angle mass - specifically a vestibular Schwannoma
6, 7, 8
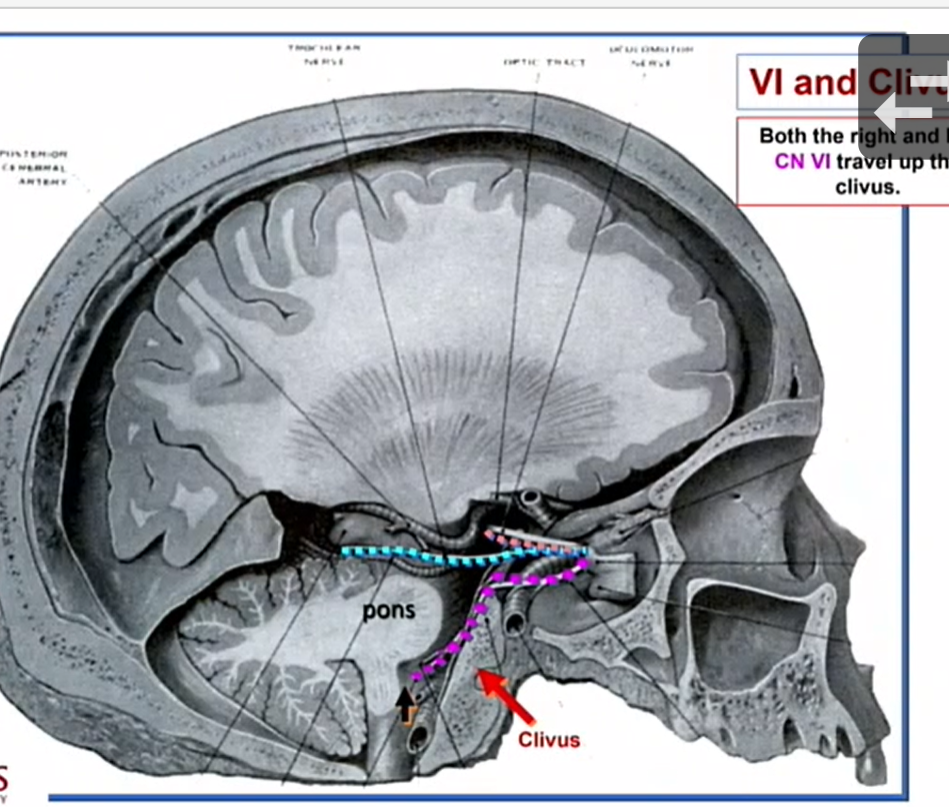
what bone is the clivus made of
occipital
both the right and left CN 6 travel up ______
clivus
what does an issue w the MLF cause
adduction
what can damage CN 6 when traveling up the clivus
spread of nasopharyngeal carcinoma

what other than CN 6 can be damaged by the spread of nasopharyngeal carcinoma
pterygopalatine ganglion - decreased tearing
whats the synapse of GSPN (CN 7)
pterygopalatine ganglion
prior to entering dorellos canal, CN 6 travels close to
inferior petrosal dural venous sinus
ligament —— pushes down and pinches 6 against bone
CN 6
petrous portion of temporal bone
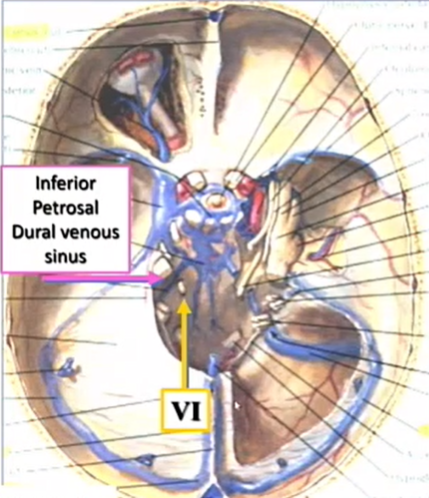
what ligament pushes on CN 6 and pushes it into petrous portion of temporal bone
petroclinoid ligament (of Gruber)
under that is dorellos canal
which CN can be compressed by increased ICP as it is traveling in Dorellos canal
6
papilledema
bilateral in distinct margins that can be caused by ICP that can cause the ligament to push onto CN 6 and shove it into the petrous portion of temporal bone
any time there is an abductino deficit there could be
optic disc edema
potential causes of papilledema/ increaed ICP
epidural hematoma
subdural hematoma
meningitis
intracranial mass
dural venous sinus thrombosis
idiopathic intracranial hypertension
gradenigo syndrome
can affect CN 6
(and 5)
associated w bacterial otitis media w petrous apex involvement
spread of infection from middle ear or mastoid
spreads intracranially via roof
whats the ear discharge in gradenigo syndrome
CSF flows into middle ear
what causes pain in gradenigo syndrome
CN V
facial/scalp/periorbital
what does gradenigo do to the eyes
diplopia from CN 6 palsy abduction deficit
whats the pathway of CN 6
low pons
subarachnoid space
prepontine cistern
clivus
dorellos canal
cav sinus
SOF
orbit
lateral rectus
a lesion affecting CN 3 and 6 is probably a lesion of
cav sinus
what can affect CN 6 in cav sinus
meninges
meningioma
Horners and ipsilateral 6 nerve palsy
6 and ICA (SYMPATHETICS) travel together in caudal cav sinus
ICA anneurysm
6 travels in the caudal cav sinus adjacent to ICA
would you rather have a PCOM or ICA in cav sinus anneurysm
PCOM
would you rather have a RUPTURED anneurysm of PCOM or ICA
PCOM = subaachnoid hemmorhage = death
ICA = cav sinus = in an enclosed venous sinus
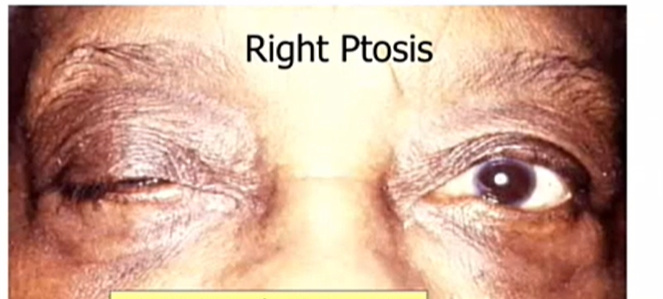
is this a ptosis or mueller issue
ptosis - its large
what can we get in the cav sinus due to the fact htat it is a dural venous sinus
venous thrombosis
this creates resistance to flow so blood will stay backed up in the eye
carotid cavernous fistula - opening of ICA
high flow arterial blood in the Cav sinus makes it difficult for venous blood to get out of the eye and into the cav sinus
does CN 6 travel in or out of the tendinous annulus
inside
Duane’s Retraction syndrome
CN 6 and/or its nucleus fails to develop
so, 3 helps it out and
usually only goes to medial rectus but also goes to lateral rectus
this will cause a crazy thing with sheringtons law —> so the eye sinks back in the globe
whatas the most common Duanes retraction syndrome
Type 1 - abduction deficit w normal adduction
abduction deficit
and the eye goes back in globe == thats bc when you use 3 to adduct its also connected to 6
gaze palsy
lesion of CN 6
primary gaze lesion of left CN 6
no tone from lateral rectus = ESO left eye
right gaze w a lesion of L CN6
look towards R and we can
could have R gaze preference - if we try to look straight ahead we have our eyes to rest
eyes point contralateral to lesion
left gaze w a lesion of L CN6
neither eye can look
foville syndrome
cause of a gaze palsy affecting the abducens nuc and CN 7 in pons
can also affect the autonomic fibers so we could get a Horners Syndrome
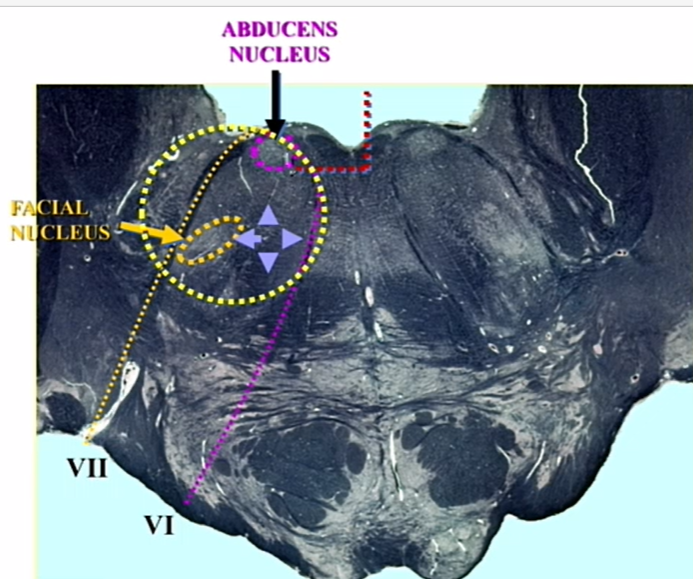
what type of weakness do we get contralateral to the gaze palsy w foville syndrome
contralateral
lesion of frontal eye fields
another cause of gaze palsy but it is not related to the abducens nuc in the pons
related to damage to the cortex
when we stimulate the frontal eye feilds the eyes will move to the _______ sid e
contralateral
where are the FEF
precentral gyrus (closer to motor bc this is motor)
in FEF lesion, the weakness is _______ to the gaze palsy
ipsilateral
In CN 6 nuc lesion, the weakness is _______ tot he gaze palsy
contralateral
distinguish cortical lesion (FEF) form pontine lesion (CN 6 nuc)
FEF = ipsilateral weakness to gaze palsy
CN 6 nuc = contralateral weakness to gaze palsy
abducens nucleus is for
ipsilateral lateral gaze
FEF are for
contralateral lateral gaze
a gaze palsy and an UMN CN 7 palsy localizes to
FEF/Cortex
a gaze palsy and a LMN palzy localizes to
low pons
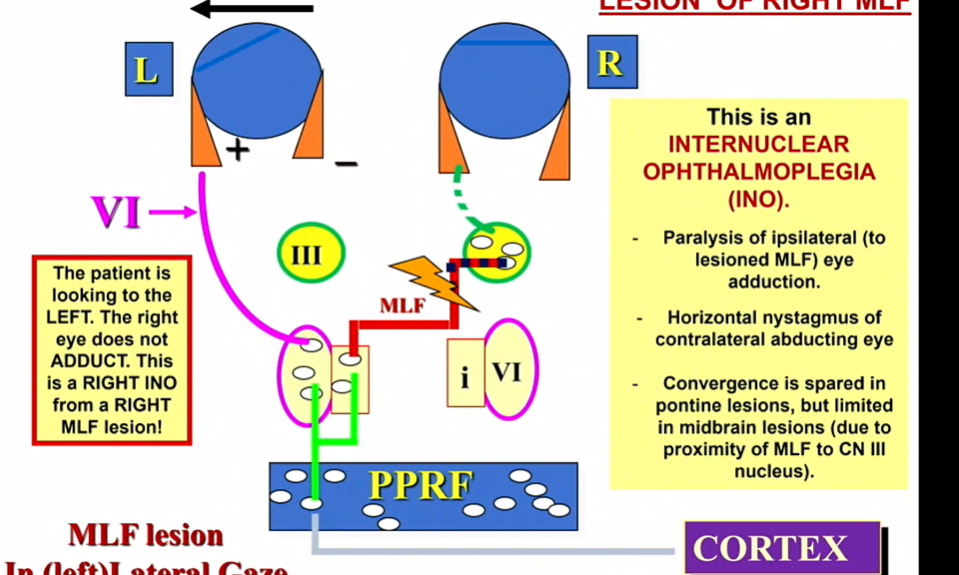
internuclear opthalmoplegia (INO)
lesion of MLF
paralysis of ipsilateral (to lesioned MLF) eye adduction
good eye shakes
caues an adduction deficit
ex: lesion of right MLF - person can abduct but not adduct
two most common causes of internuclear opthalmoplegia
demyelination - multiple sclerosis —> YOUNG PERSON
vasculopathic - stroke, infarction —> OLD PERSON
INO - w MLF lesion if it is in pons convergence is ________
spared
INO - w MLF lesion in midbrain - convergence is _________
abolished