Spirometry + Pre-Aerobic Quiz
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
What are the three main sources of ATP available to exercising muscle?
Phosphagen system (creatine phosphate), glycolysis, and aerobic respiration
Which ATP source provides the fastest supply during exercise?
Phosphagen system (creatine phosphate)
Why is aerobic respiration considered the most efficient ATP source?
It produces the most ATP per glucose molecule but is oxygen dependent and slower to start
What is oxygen debt?
The elevated oxygen consumption after exercise needed to restore phosphagen and glycogen reserves and repay the oxygen deficit at start of exercise
How does the sympathetic nervous system support exercise?
By increasing heart rate, causing vasoconstriction in skin and gut, and bronchodilation to increase oxygen delivery
What happens to cardiac output and systemic resistance during exercise?
Cardiac output increases while systemic resistance decreases
Why does blood pressure usually increase during exercise?
Because the increase in cardiac output is greater than the decrease in systemic resistance
How does breathing rate change during exercise?
Respiratory rate increases before blood CO2 rises, triggered by proprioceptors and cognitive anticipation
What physiological indicator reflects sympathetic activation on the skin?
Decreasing skin temperature due to vasoconstriction
How does aerobic fitness affect exercise recovery?
More fit individuals recover faster, have less EPOC, larger vital capacity and hearts, and lower resting heart rates
What is Glycolysis?
Intermediate speed ATP producer, occurs in the cytoplasm, doesn’t require oxygen
What is aerobic respiration?
Slowest ATP producer, but most efficient, occurs in mitochondria, requires oxygen
Where is creatine phosphate made?
Made in the mitochondria, but used in the cytoplasm
What is the Cori Cycle?
Involved in regenerating creatine phosphate and glycogen reserves
How do respiratory muscle contractions cause thoracic volume changes?
Expands the thoracic cavity, increasing thoracic volume and decreasing pulmonary pressure, allowing air to flow into lungs
What is the relationship between thoracic volume and pulmonary pressure during breathing?
Inverse relationship: as thoracic volume increases, pulmonary pressure decreases (inhalation), as thoracic volume decreases, pulmonary pressure increases (exhalation)
What are the key functional lung volumes measured in spirometry?
Tidal Volume, Inspiratory Reserve Volume, Expiratory Reserve Volume, Residual Volume, Vital Capacity, and Total Lung Capacity
Define Tidal Volume
The volume of air inhaled or exhaled during normal, relaxed breathing (approx. 500mL)
What is Inspiratory Reserve Volume?
The maximum volume of air that can be inhaled after a normal inhalation
What is Expiratory Reserve Volume?
The maximum volume of air that can be exhaled after a normal exhalation
What is Residual Volume?
The amount of air remaining in the lungs after a maximum exhalation; this air cannot be voluntarily expelled
How is Vital Capacity calculated?
VC=TV + IRV + ERV
What is Vital Capacity?
The total volume of air that can be exhaled after a maximum inhalation
How is Total Lung Capacity calculated?
TLC=VC + RV
What is Total Lung Capacity
Total amount of air lungs can hold
What does Alveolar Minute Volume indicate?
AMV indicates the volume of fresh air reaching the alveoli per minute
How is AMV calculated?
AMV= (Tidal Volume - Dead Space) x Breathing Rate
What is the typical dead space volume used in AMV calculations?
Approximately 150mL of air representing volume in conducting zones not involved in gas exchanged
How do changes in alveolar ventilation influence blood CO2 and pH?
Increased alveolar ventilation lowers CO2, raising pH (alkalosis); decreased ventilation raises CO2, lowering blood pH (acidosis)
What distinguishes restrictive lung diseases from obstructive lung diseases?
Restrictive diseases reduce lung volume due to lung stiffness (pulmonary fibrosis), while obstructive diseases increase airway resistance, impairing airflow rate (asthma)
What spirometry measurement helps diagnose obstructive lung diseases?
FEV1; a low FEV1 indicates airway obstruction
How is FEV1 interpreted in obstructive vs restrictive lung disease?
Obstructive disease shows reduced FEV1, while restrictive disease shows normal or near-normal FEV1
Which respiratory muscles are involved in normal breathing?
Diaphragm and external intercostal muscles contract during inhalation; internal intercostals aid forced exhalation
Describe how blood oxygen saturation is regulated in response to respiratory changes
Chemoreceptors in the medulla and peripheral sites monitor CO2, O2, and pH levels and adjust breathing rates accordingly
What is the role of central chemoreceptors in respiratory regulation
Primarily respond to CO2 and pH changes in cerebrospinal fluid
What is the role of peripheral chemoreceptors in respiratory regulation?
Respond to low O2 and high CO2 in blood, triggering increased respiration
Why is there a time lag between breathing changes and peripheral blood oxygen saturation changes?
Due to circulation time needed for oxygenated blood to travel from lungs to peripheral tissues where saturation is measured
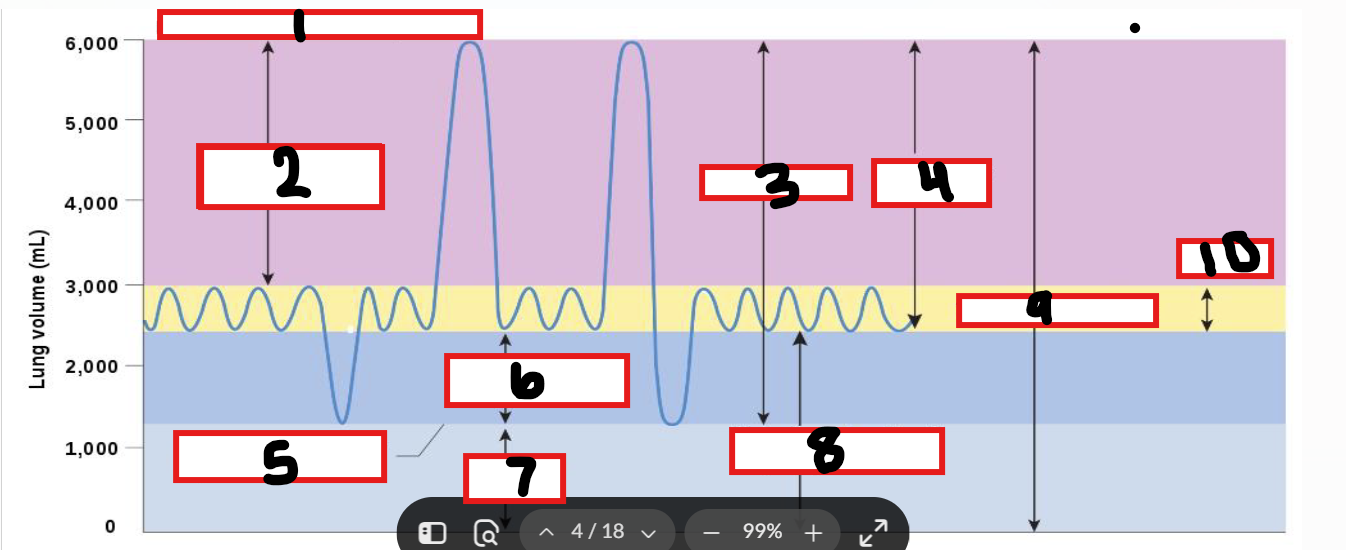
What is 1
Maximum possible inspiration
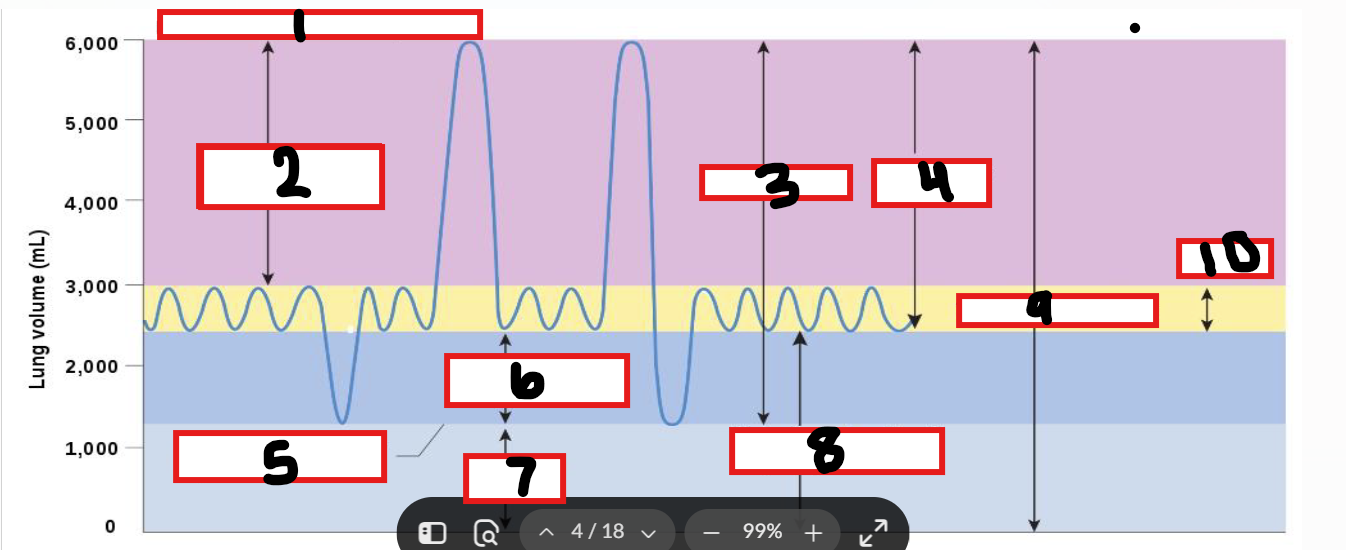
What is 2
Inspiratory reserve volume
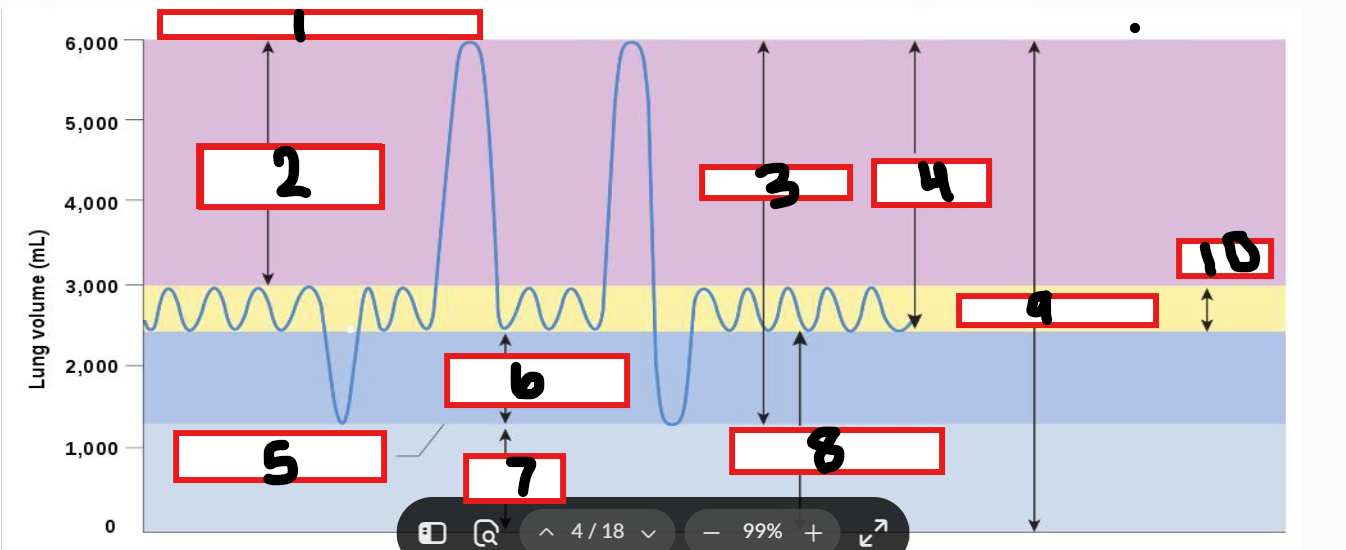
What is 3
Vital capacity
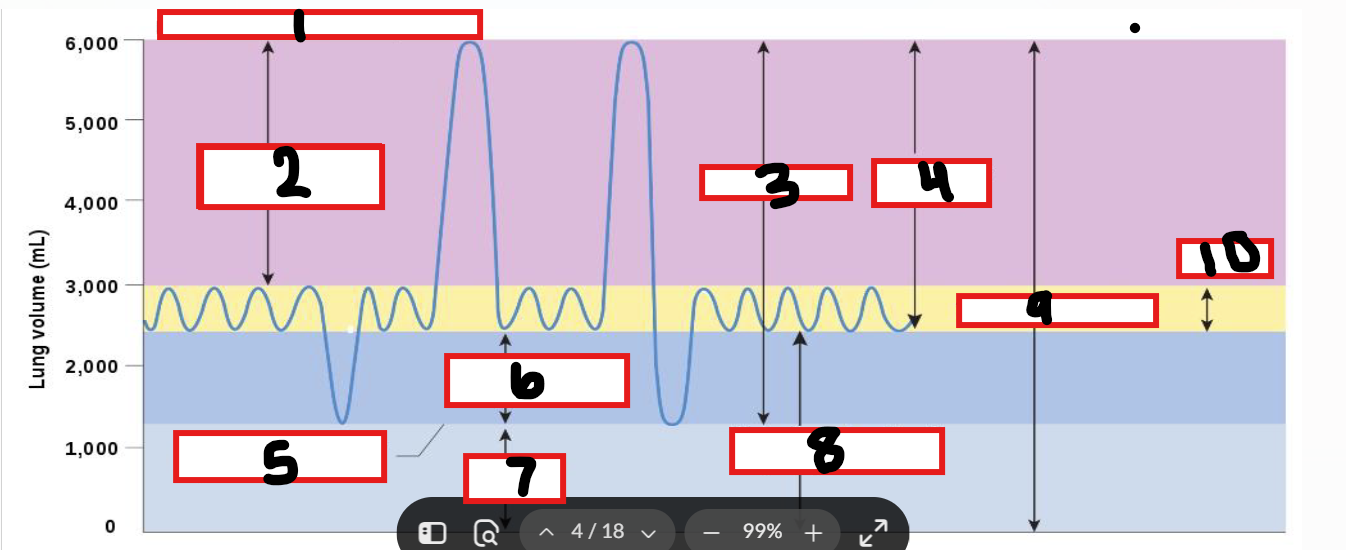
What is 4
Inspiratory capacity
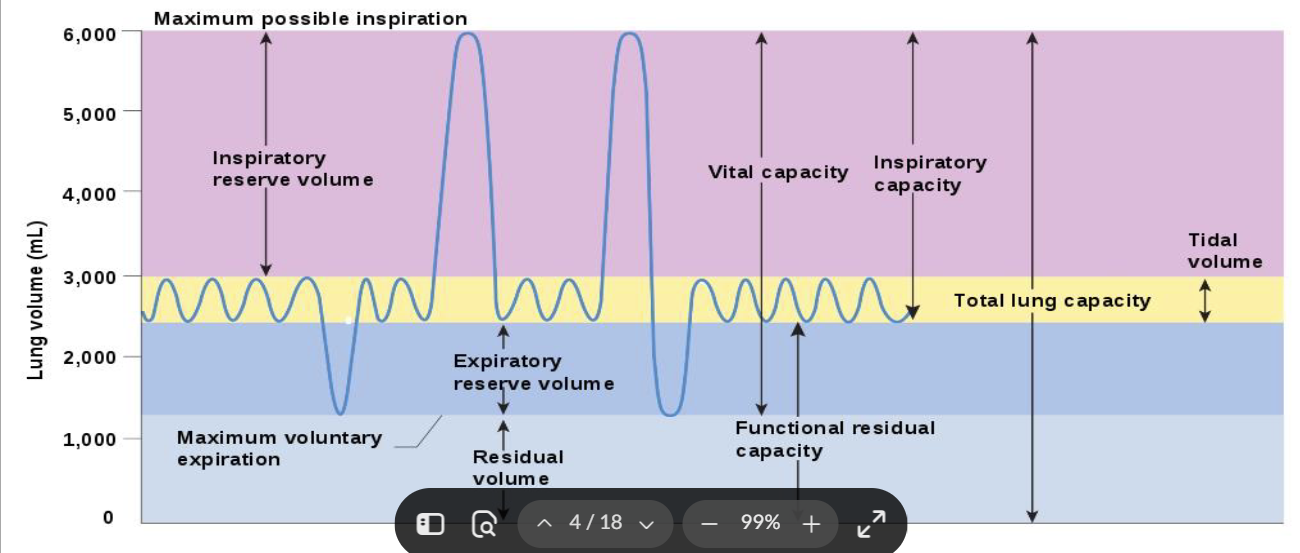
What is 5
Maximum voluntary expiration
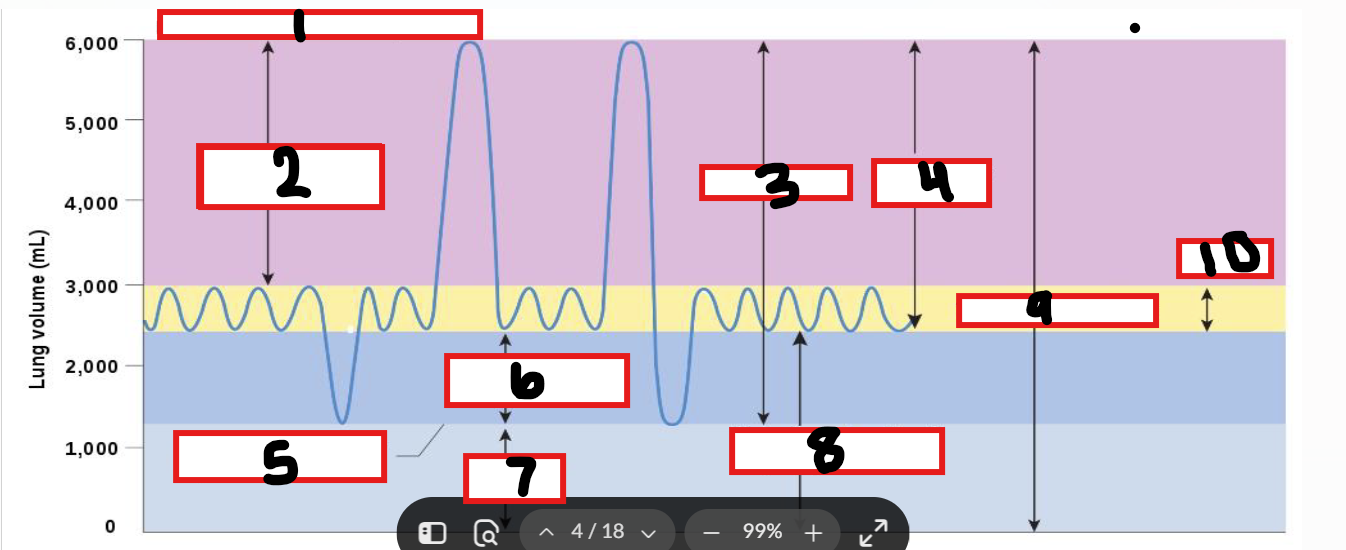
What is 6
Expiratory reserve volume
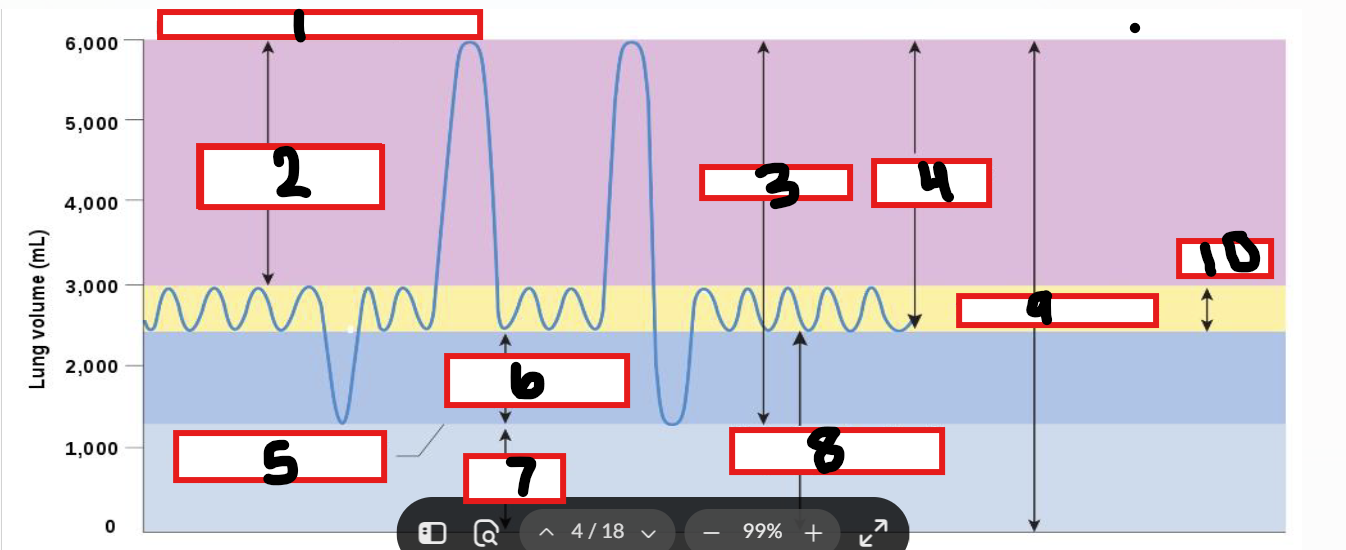
What is 7
Residual volume
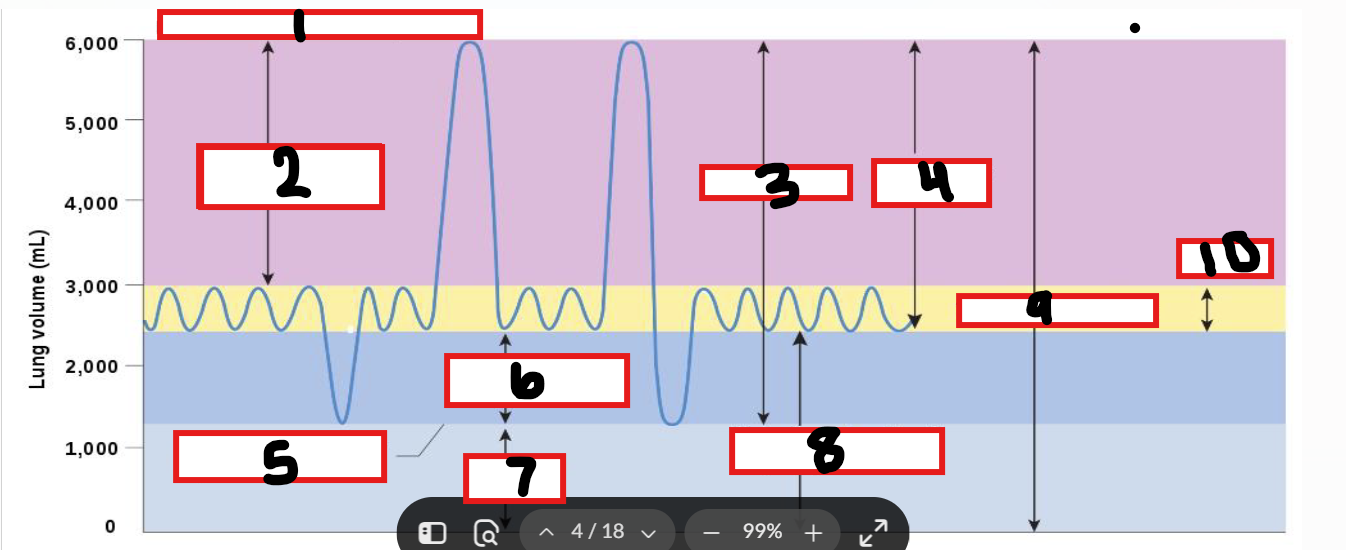
What is 8
Functional residual capacity
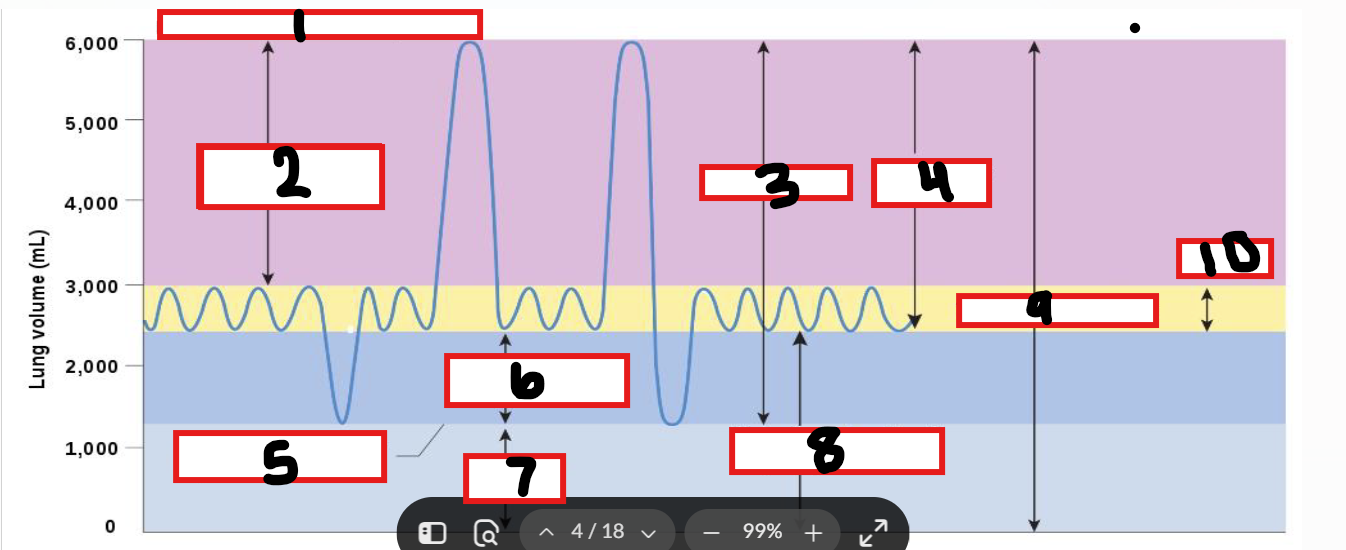
What is 9
Total lung capacity
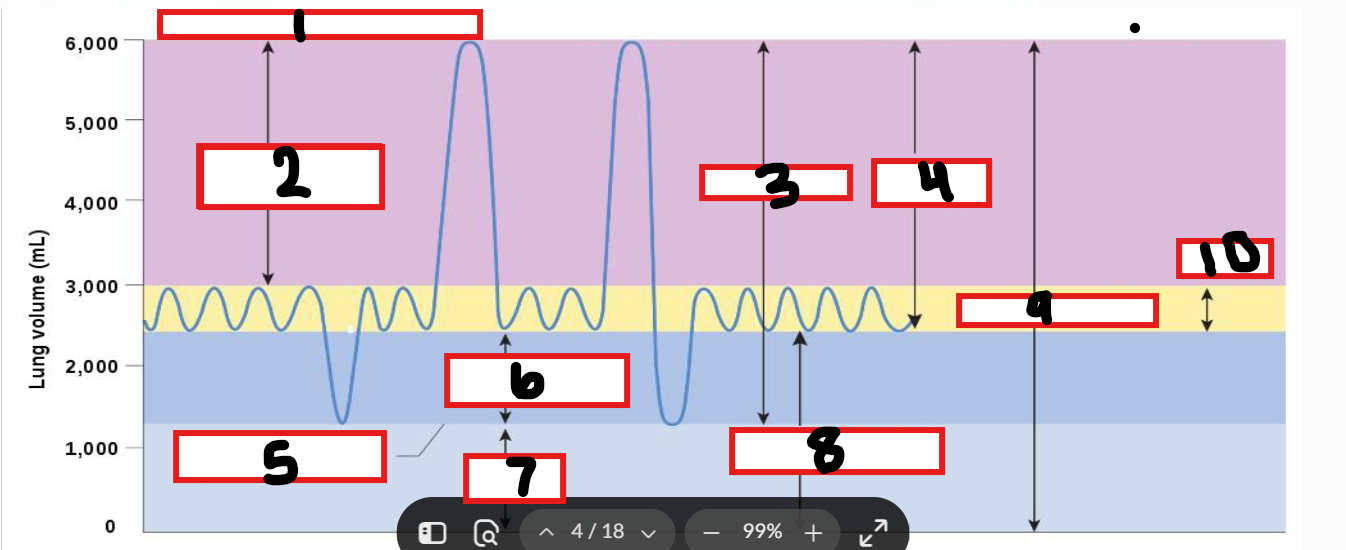
What is 10
Tidal volume