Human physiology exam 3
1/56
Earn XP
Description and Tags
cardiovascular physiology
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
the cardio vascular system, is a series of tubes ___ filled with fluid ____ and connected to a pump ____.
vessels, blood, heart
materials entering the body
oxygen, nutrients, and water
materials moved from cell to cell
wastes, immune cell, antibodies, clotting proteins, hormones, stored nutrients
materials leaving the body
metabolic wastes, heat, and carbon dioxide
Heart
one way closed circuit
gas, nutrients, waste
pump
pressure goes high to low
aorta, arteries, arterioles, capillaries, venules, veins, venae cavae
pressure
the force exerted by the fluid on its container. friction causes a pressure drop.
hydrostatic pressure
pressure exerted with no fluid movement. proportional to the height of the water column.
as the radius of a tube decreases
the resistance to flow increases
pericardium
heart encased within a membranous fluid-filled sac called the
atrial ventricular (AV) valves
tricuspid- right
Mitral/ bicuspid- left
semilunar valves
pulmonary artery
aorta
main purpose is to prevent back flow
ventricular contraction
AV valves remain closed to prevent blood flow backward into the atria
ventricular relaxation
semilunar valves prevent blood that has entered the arteries from flowing back into the ventricles.
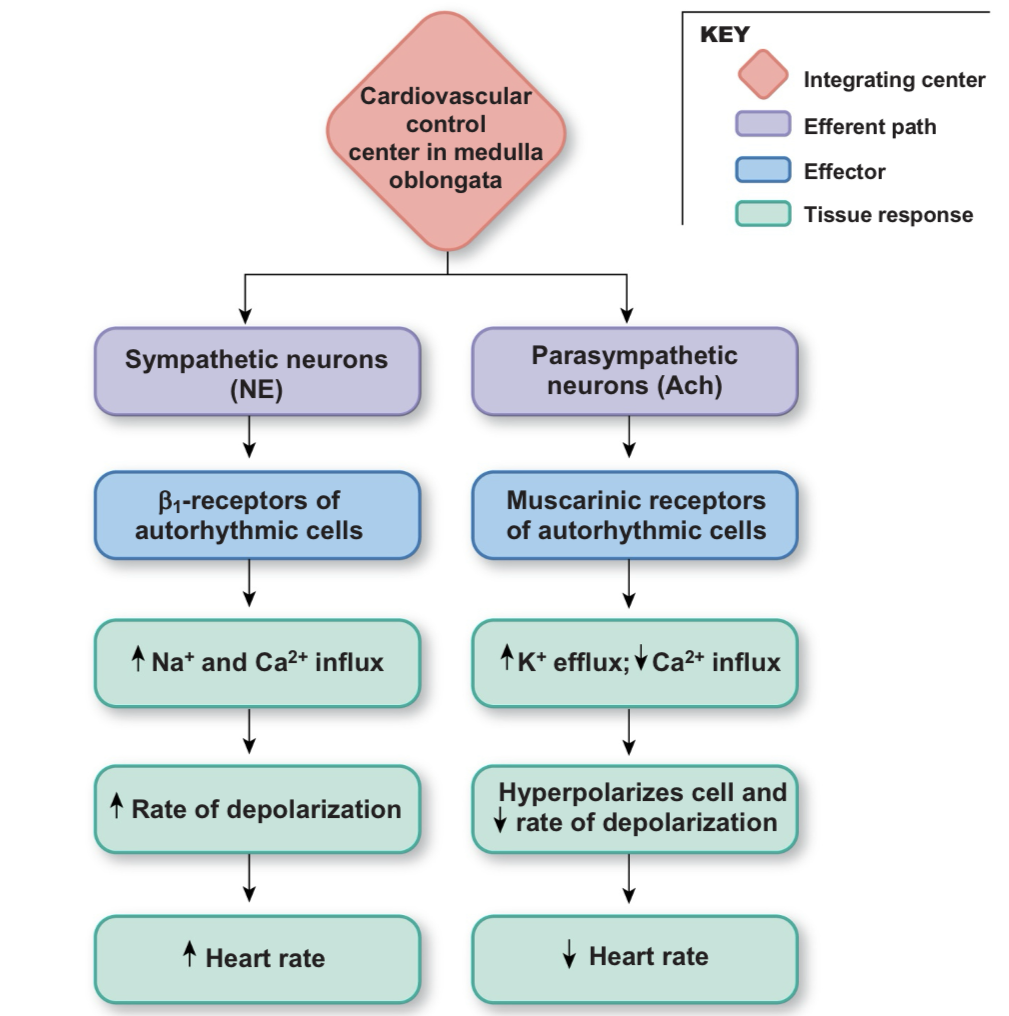
where does the electrical signal come from to initiate contraction in the heart? (myocardial contraction)
autorhythmic cells the medulla controls
cardiac muscles vs skeletal muscles
smaller and have single nucleus per fiber
have intercalated disks
desmosomes allow force to be transferred (strong connections that tie cell together)
gap junctions provide electrical connection ( allows depolarization to spread rapidly from cell- cell)
T- tubules are larger and branch
sarcoplasmic reticulum is smaller
mitochondria occupy one-third of cell volume (very high energy demand, consumes roughly 70-80% of oxygen delivered)
cardiac muscle contraction
can be graded by calcium concentration
sarcomere length affects force of contraction
action potentials vary according to cell type
a lot of calcium stronger contraction
bridges between actin and myosin affects contraction
skeletal muscle
stable at -70 mv
net na+ entry through ACh-operated channels
rising phase of action potential: Na+ entry
Rapid; caused by K+ efflux
hyperpolarization; leak of K+ and Na+ restores potential to resting state
duration of action potential; 1-2 msec
refractory period; brief
contractile myocardium
stable at -90 mv
depolarization enters via gap junction
rising phase of action potential: Na+ entry
repolarization phase; extended plateau caused by ca2+ entry; rapid phase caused by K+ efflux
hyperpolarization; non
duration of action potential; extend 200+ msec
refractory period; long
autorhythmic myocardium
unstable pacemaker potential starts at -60 mv
net Na+ entry through If channels; reinforced by ca2+ entry
rising phase of action potential; ca2+ entry
repolarization phase; normally none
duration of action potential; variable generally 150+ msec
refractory period; none
electrical conduction in the heart
SA node, internodal pathways, AV node, Av bundle, bundle branches, purkinje fibers
AV node
routes the direction of electrical signals
delays the transmission of action potentials
SA nodes
sets the pace of the heartbeat at 70 bpm
AV node (50 bpm) and purkinje fibers (25-40 bpm) can act as pacemakers under some conditions
p wave
atrial depolarization
QRS
ventricular depolarization; also includes atrial repolarization (relaxation)
T wave
ventricular repolarization
Heart rate normal
60-100 bpm
train atheletes may have a slower rate
abnormal heart rate
tachycardia - fast
bradycardia- slow
arrhythmia- irregular
mechanical events
late diastole- both sets of chambers are relaxed and ventricles fill passively (heart at rest)
atrial systole- atrial contraction forces a small amount of additional blood into ventricles
isovolumic ventricular contraction- first phase of ventricular contraction pushes AV valves closed but does not create enough pressure to open semilunar valves (lub)
ventricular ejection- as ventricular pressure rises and exceeds pressure in the arteries, the semilunar valves open and blood is ejected
isovolumic ventricular relaxation- as ventricles relax, pressure in ventricles fall, blood flows back into cusps of semilunar valves and snaps them closed. (dub)
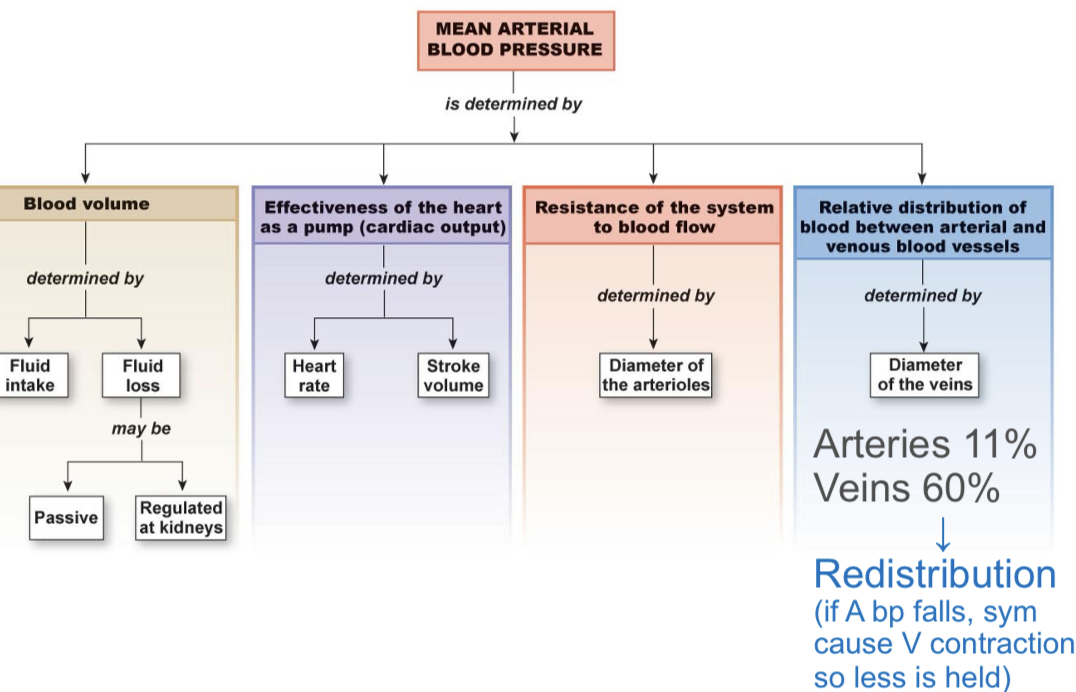
stroke volume
amount of blood pumped out by one ventricle during a contraction
EDV( 135) - ESV (65) = stroke volume (70)
Frank- starling law states - stroke volume increases as EDV increases
EDV is affected by venous return
venous return affected by- skeletal muscle pump, respiratory pump, and sympathetic innervation ( change force of contraction changes volume)
force of contraction is affected by stroke volume
length of muscle fiver and contractility of heart
cardiac output
volume of blood pumped by one ventricle in a given period of time
CO = HR x SV
average = 5 L/min
autonomic neurotransmitters alter heart rate
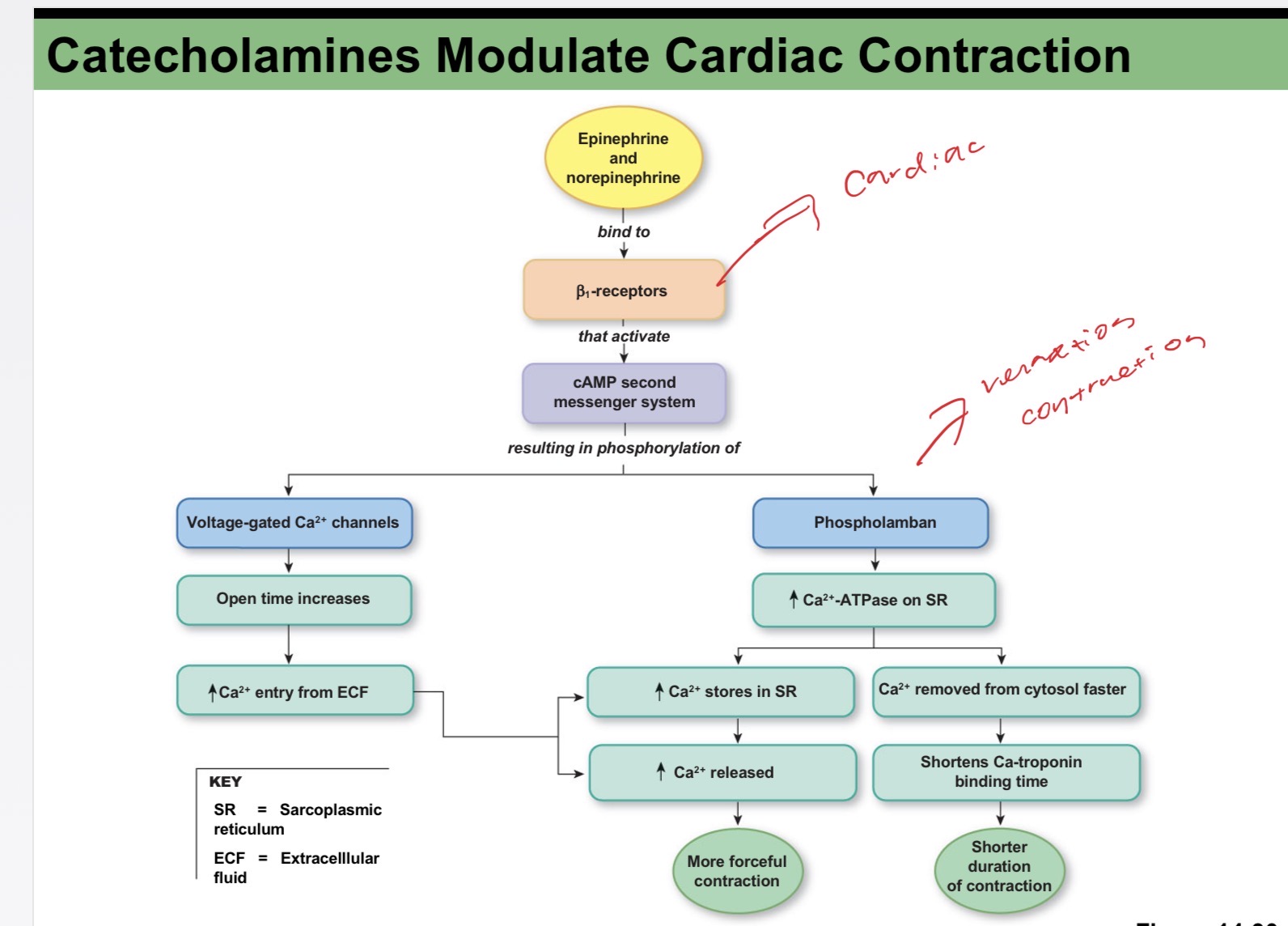
catecholamines modulate cardiac contraction
stroke volume and heart rate determine cardiac output

functional model of the cardio vascular system
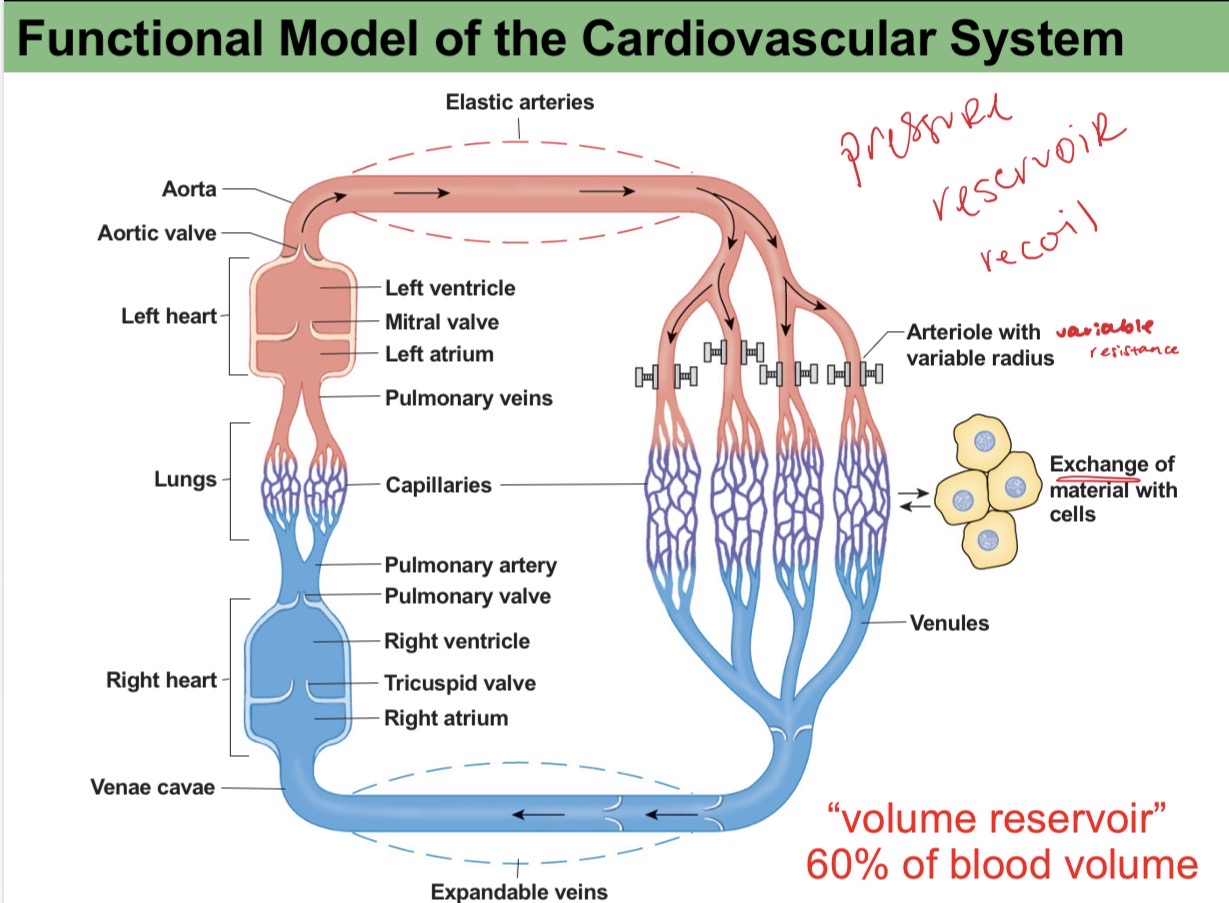
capillaries
smallest vessel
site of exchange
lack smooth muscle and elastic tissue reinforcement, which facilitates exchange through a layer of endothelium
precapillary sphincters- constrict and prevent flow
elastic recoil in arteries
contraction
ventricle contracts
semilunar valve open
aorta and arteries expand and store pressure in elastic wall
relaxation
isovolumic ventricular relaxation
semilunar valves shut, preventing flow back into ventricle
elastic recoil of arteries sends blood forward into rest of circulatory system
hypertension
systolic >140 and diastolic >90
pre-hypertension
systolic-120-139 and diastolic- 80-89
blood pressure
pulse pressure= systolic p- diastolic p
MAP= diastolic P +1/3(systolic p-diastolic p)
mean arterial pressure is a function of cardiac output and resistance in the arterioles
blood pressure control includes rapid responses from the cardiovascular system and slower responses by the kidneys
factors that influence mean arterial pressure
arteriolar resistance
arteriorlar resistance is influenced by both local and systemic control mechanisms
local control- based on mediated by CNS
hormones- control salt and water balance through kidney
chemicals mediating vasoconstriction
norepinephrine; (alpha-receptors) ,baroreceptor reflex, sympathetic neurons, neurotransmitter
endothelin; paracrine mediator, vascular endothelium, paracrine
vasopressin; increases blood pressure in hemorrhage, posterior pituitary, neurohormone
angiotensin II; increases blood pressure, plasma hormone, hormone
chemicals mediating vasodilation
epinephrine (b2); increase blood flow to skeletal muscle, heart, liver, adrenal medulla, neurohormone
acetylcholine; erection flex, parasympathetic neurons, neurotransmitter
nitric oxide; paracrine mediator, endothelium, paracrine
bradykinin (via NO); increases blood flow, multiple tissues, paracrine
adenosine; increases blood flow to match metabolism; cell metabolism; paracrine
histamine; increases blood flow, mast cells, paracrine
natriuretic peptides; reduce blood pressure; atrial myocardium, brain, hormone, neurotransmitter
vasoactive intestinal peptide; digestive secretion, relax smooth muscle, neurons, neurotransmitter, neurohormones
arteriorlar resistance
myogenic autoregulation (sm. muscle contraction influenced by blood pressure)
paracrines- active hyperemia ( low o and high co2; dialation, high blood flow) - reactive hyperemia ( period of low perfusion)
sympathetic control- sns; norepinephrine, adrenal medulla; epinephrine
active hyperemia
more activity more blood flow
paracrine signal causes vasodilation
reactive hyperemia
reactive rebound
Reactive hyperemia is a temporary surge in blood flow after a blockage is removed
o2 drops and metabolites build up
distribution of blood
85% in the liver and digestive tract, kidneys, and skeletal muscle
continuous capillaries
most common, continuous
pass smaller molecules
found in the muscle, con tissue, blood brain barrier
fenestrated capillaries
associated with pores
pass larger molecules and volumes
found in the kidney and intestine
capillary exchange
exchange between plasma and interstitial fluid occurs by paracellular pathway (between cells) or endothelial transport (through cells)
small dissolved solutes and gasses move by diffusion
larger solutes and proteins move by vesicular transport
diffusion rate determined by concentration gradient
bulk flow; mass movement as a result of hydrostatic or osmotic pressure gradients
absorption; fluid movement into capillaries- net absorption on venous end
filtration; fluid movement out of capillaries- caused by hydrostatic pressure, net filtration at arterial end
net pressure= hydrostatic pressure- colloid osmotic pressure
lymphatic system
returning fluid and proteins to circulatory system
picking up fat absorbed and transferring it to circulatory system
serving as filter for pathogens
edema
two causes
inadequate drainage of lymph
filtration far greater than absorption
disruption of balance between filtration and absorption
increase in hydrostatic pressure
decrease in plasma protein concentration
increase in interstitial proteins
baroreceptors
BP goes down- less firing (carotid and aortic)
SA node change heart rate (parasympathetic)
BP goes up-more firing (carotid and aortic)
response to high blood pressure
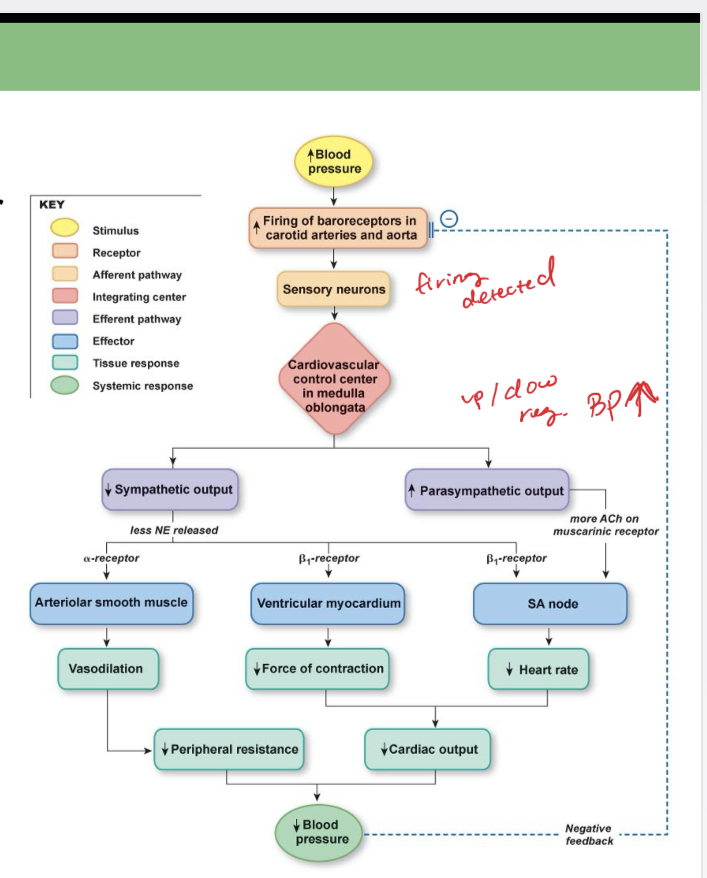
response to low blood pressure

CVS; Risk factors
not controllable
-sex
-age
-family history
controllable
-smoking
-obesity
-sedentary lifestyle
-untreated hypertension