Intro to cancer
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
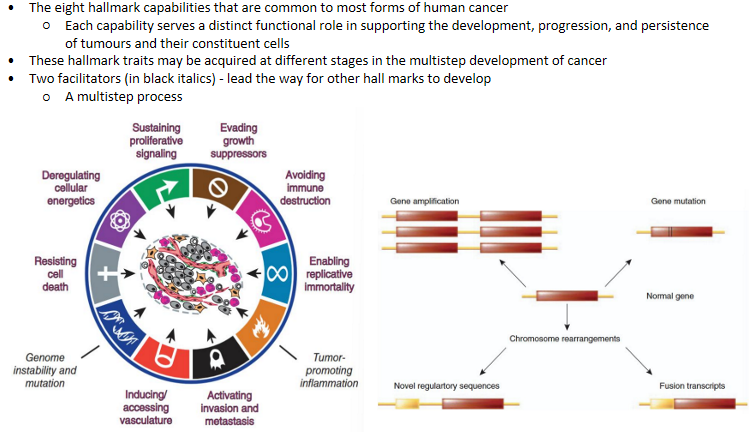
The biological hallmarks of cancer
Which process is central to metastasis in cancer hallmarks?
A) Sustaining proliferative signalling - occurs at tumor sites
B) Activating invasion and metastasis
C) Evading growth suppressors - not related to spread
D) Enabling replicative immortality - tumor resistance
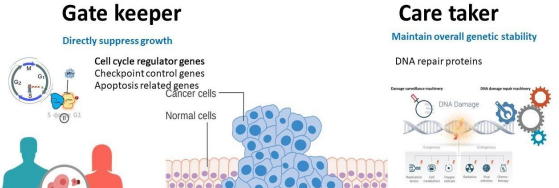
what are tumour suppressor genes
Tumour suppressor genes normally inhibit cell division or promote repair/apoptosis, functioning as "brakes" on growth.
Loss-of-function mutations (often both alleles via the two-hit hypothesis) inactivate them, enabling hallmarks like growth suppressor evasion.
TP53 (guardian of the genome, triggers cell death)
RB1 (cell cycle control)
BRCA1 and BRCA2 (mutations increases risk of breast & ovarian cancer)
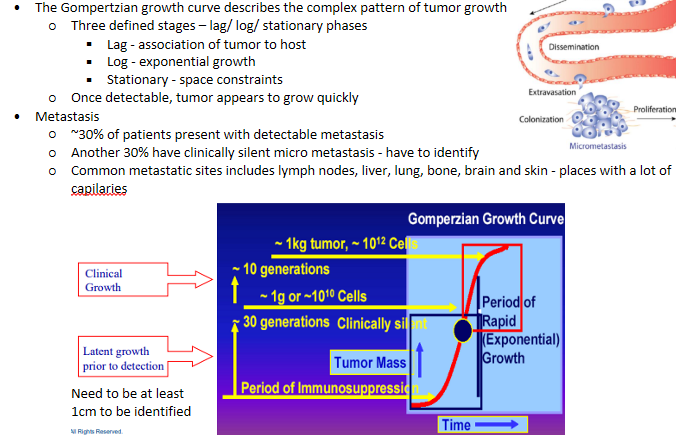
Tumor growth kinetics
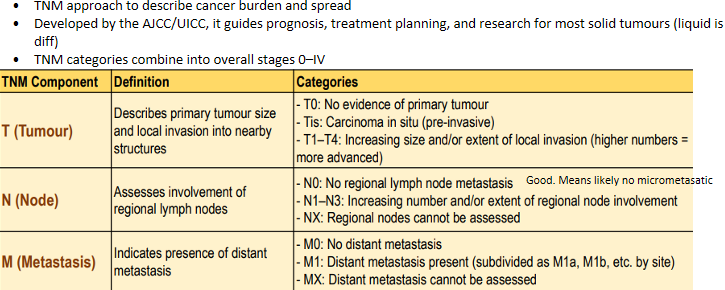
Staging with TNM
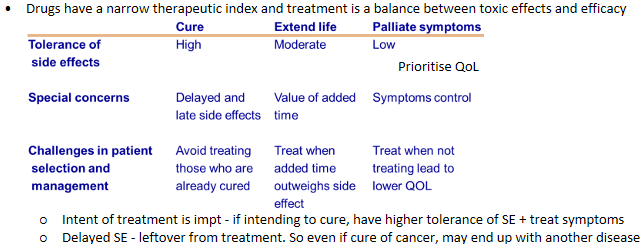
Goals of cancer therapy
Curative
Maintenance of quality & duration of life
Symptom relief (palliative treatment)
Clinical trials for experimental therapies - if no therapies available
Goals of therapy must be discussed between patient, family, physicians and health care team
Types of cancer treatments
Types of chemotherapy
Multimorbidity impacts on prognosis - Comorbidities, Performance Status, and Frailty
Comorbidities, performance status, and frailty each independently worsen cancer prognosis by increasing risks of treatment toxicity, reduced tolerance, hospitalization, and mortality
These factors interact, often amplifying risks in older adults or those with advanced disease.
Biggest concern is whether pt can tolerate treatment
Balancing benefit, toxicity, and quality of life
Therapeutic decisions prioritize maximal benefit (PFS/OS extension) while minimizing toxicity that impairs QoL, such as severe fatigue, neuropathy, or hospitalization.
Align goals, shared decision making with pt and family
Multimorbidity impacts on prognosis - Comorbidities
Multimorbidity, the coexistence of two or more chronic conditions, is highly prevalent among cancer patients and escalates sharply with age, complicating treatment and worsening outcomes.
If the co-morbidities not managed, may cause death
The prevalence of multimorbidity (individuals aged >60) in the study was 48.4%
Multimorbidity and polypharmacy at the time of cancer diagnosis were associated with decreased survival.
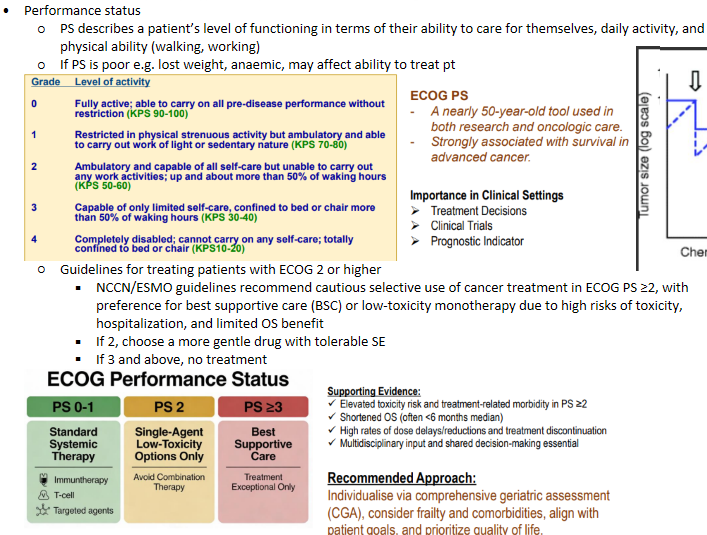
Multimorbidity impacts on prognosis - Performance status
Multimorbidity impacts on prognosis - frailty
Strongly modifies prognosis, with frail patients facing 1.5–2x higher risks of death, toxicity (OR 1.8), intolerance, and hospitalization.
Chemotherapy - fractional cell kill hypothesis
The fractional cell kill hypothesis predicts that a given dose of cytotoxic drug kills a given proportion of cells, rather than a given number, regardless of the tumor size
Reduction in cell kill by each repeated dose of cytotoxic drug due to the reduction in the size of the tumor
Repetitive cycles of treatment are needed
Early treatment when tumor is small gives better clinical outcome
Chemotherapy - NTI drugs
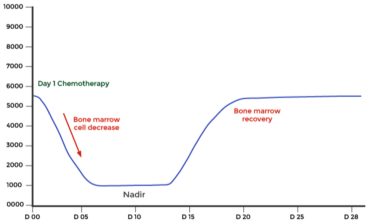
Chemotherapy - myelosuppression
Permanent damage to the bone marrow when cytotoxic drugs administered too often or at high doses that impede bone marrow recovery between treatments
The nadir can differ between different cytotoxic drugs, but usually occurs 7-14 days after treatment administration
Have to watch out during nadir to prevent sepsis
Intermittent administration of cytotoxic drug protocols in treatment cycles is the most common method of scheduling e.g. q21 days, q28 days
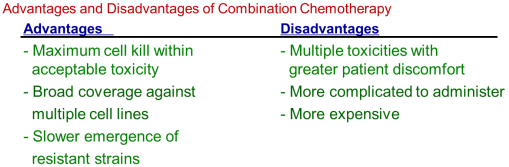
Chemotherapy - combinations
Combination chemotherapy used to improve treatment outcome
Clinical trial outcomes inform the use of certain drugs and drug combinations, their doses and administration frequency based on their efficacy for specific tumor types.
Drugs used in combination may be chosen based on:
individual activity
phases of the cell cycle
synergy
side effect profiles - select drugs with different SE
Chemotherapy - treatment cycles
Anti-cancer drugs may be delivered in intervals called cycles
A cycle consists of treatment days (where the drugs are administered) and rest days, which allow normal cells to recover before the treatment is administered again
Treatment cycles can vary in length, for example 14, 21 or 28 days
Drug-related factors that may influence cycle length include the drug half-life, toxicity profile and cellular target
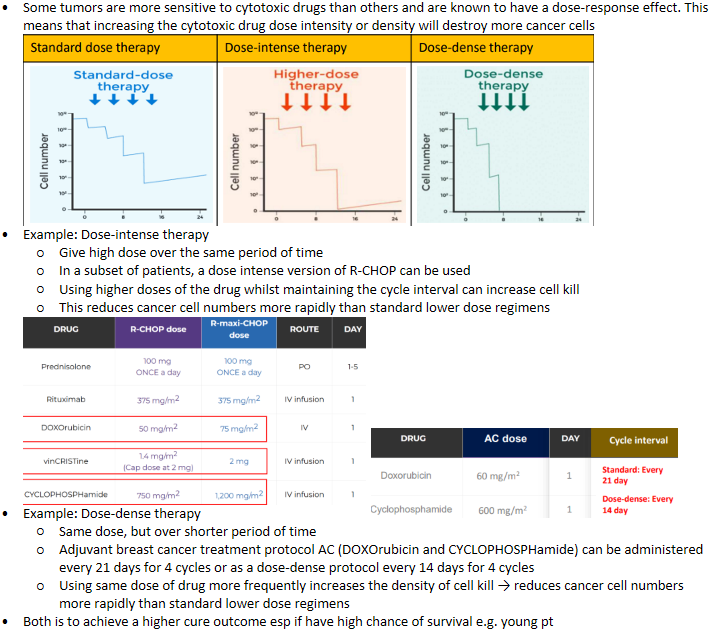
Chemotherapy - Cytotoxic drug dose intensity
Chemotherapy - Protocols concept
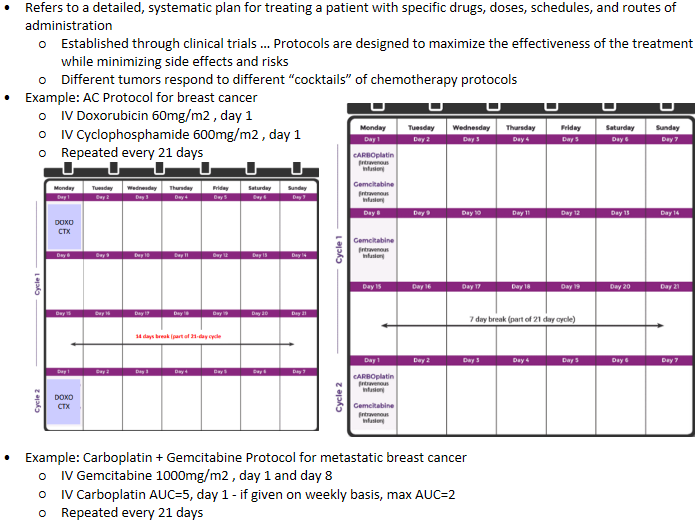
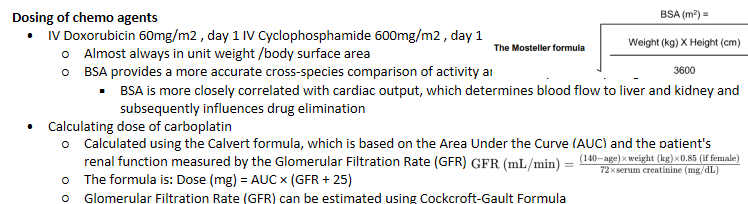
Chemotherapy - Dosing of chemo agents
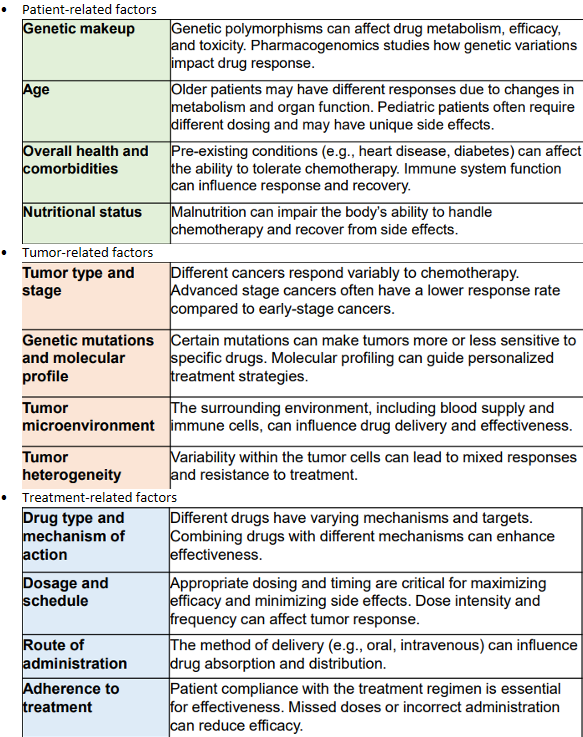
Chemotherapy - Factors affecting the effectiveness of chemo treatment