Week 13-14: Wrist & Hand
1/459
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
460 Terms
Carpal bones proximal row
scaphoid, lunate, triquetrum, pisiform
Carpal bones distal row
trapezium, trapezoid, capitate, hamate
wrist joints
-DRUJ
-----pro/sup
-Radiocarpal
------includes articular disc
-Midcarpal
------ med/Lat compartments
Extrinsic wrist ligaments
Connect the forearm to a carpal bone
More superficial layers
Intrinsic wrist ligaments
from carpal to carpal.
Deepest layer.
Tightly binds the carpal bones
TFCC (triangular fibrocartilage complex)
Occupies the ulnocarpal space.
Includes
Triangular fibrocartilage (TFC) aka articular disc
Capsular ligaments of DRUJ
Ulnar collateral ligament
TFCC main responsibility
Primary stabilizer of the DRUJ, which is responsible for pronation and supination
Max grip force occurs at about
30º of extension
nerves of the wrist/hand
-Median (motor and sensory)
-Ulnar (motor and sensory
-Radial (sensory only in wrist/hand)
wrist/hand specific patient history
-Age
-repetitive movements? (Occupation?, Sports?, Hobbies?)
-Onset (sudden, gradual, clear cause or insidious)
-MOI
-Numbness/tingling, Paresthesia's at night?
-Alleviating movements/positions
-pain/problems/injuries anywhere else in the upper quarter
Trauma to hand
Causes lots of hand injuries esp occupational health d/t workplace accidents and equipment malfunctions
Observation: Common Hand Deformities
Bouchard's nodes
Heberden's nodes
Mallet finger
Boutonniere
Claw Hand
Zigzag
Ulnar drift
Swan neck
Wrist drop
Functional hand assessment
Open and closed hand
Lumbrical
hook grip
Straight fist: DIPs are extended, PIP and MCP are flexed
Closed fist w/ thumb
Pulp to pulp
Tip to tip
Key pinch
straight fist
DIPs are extended, PIP and MCP are flexed

Intrinsic plus
MCP flexion, PIP and DIP extension

extrinsic plus
MCP hyperextension and IP flexion
Grip and grip strength
CMC of thumb and 5th CMC are contributors to make cylinder and spherical grip
Chuck or three finger pinch (digital prehension)
Thumb, index, and middle finger grasp and object
wrist/finger Tissue Length testing
- Finger extrinsics
- Finger intrinsics
lateral or key pinch
Thumb and index finger adduct and flex
resting position of the radiocarpal joint
neutral, slight ulnar deviation
Closed pack position of the radiocarpal joint
extension
capsular pattern of radiocarpal joint
flexion and extension equally limited
resting position of the intercarpal joint
neutral or slight flexion
close pack position of the intercarpal joint
extension
resting position of the midcarpal joint
neutral or slight flexion with ulnar deviation
closed pack position of the midcarpal joint
extension with ulnar deviation
capsular pattern of the midcarpal joint
equal limitation of flexion and extension
carpometacarpal joint resting position
thumb - midway between abduction and adduction, flex/ext
finger - mid flexion/extension
carpometacarpal joint closed pack position
thumb - full opposition
finger - full flexion
carpometacarpal joint capsular pattern
thumb - abduction, extension
fingers - equal in all directions
metacarpophalangeal joint resting position
slight flexion
metacarpophalangeal joint closed pack position
thumb: full opposition
fingers: full flexion
metacaropophangeal joint capsular pattern
flexion, then extension
interphalangeal joint resting position
slight flexion
interphalangeal joint closed pack position
full extension
interphalangeal joint capsular pattern
flexion and extension
when providing OP to the wrist, where should the pressure be placed, and why?
the 3rd MCP, it is the central pillar and most stable. 4th, 5th, and 1st MCP are very mobile.
wrist flexion end feel
tissue stretch
wrist extension end feel
firm/hard
wrist RD/UD end feel
firm/hard
end feels of the digits
-MCP flex - hard/firm
-MCP ext - firm
-Abd - firm
-IP flex - firm/hard, maybe soft tissue
-IP ext end feel - firm
-composite finger flex - soft tissue/ firm
end feels of the thumb
-CMC flex - firm/soft tissue
-CMC ext - firm
-CMC abd - firm
-CMC opposition - firm/soft tissue
Composite finger flexion
Measure from distal palmar crease to tip of finger
Tip should be able to touch palmar crease for norma
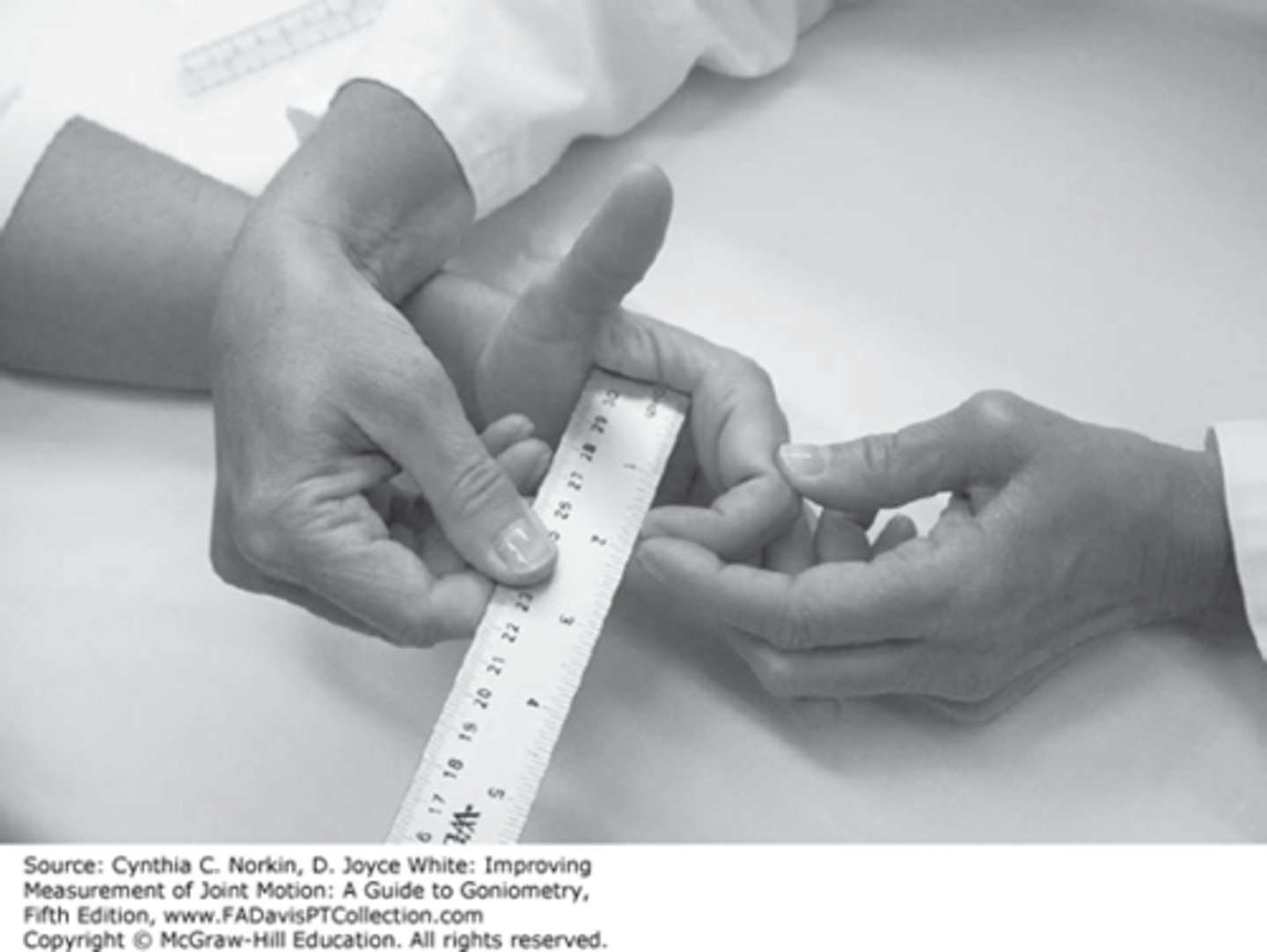
CMC opposition
Measures distance between thumb and 5th metacarpal
position for dynamometer grip testing
arm at side, elbow at 90 degrees. Handle in midposition, but depends on patient's hand size.
grip is most effective with the wrist in what position?
slight extension
when to question's a patients effort with grip dynamometry ?
if there is a >20% discrepancy in repeated trials
general trends of grip strength
peaks from early to mid-adulthood, then declines.
5- 10% difference in dominant vs nondominant is normal
Pinch dynamometer
Average of 3 trials on each hand
Do each type of pinch
Chuck
Lateral
Tip to tip
Wrist reflex tests
Reflexes same as the UQ Screen
- Biceps
- Triceps
- Brachioradialis
static 2 point discrimination
uses a two point discriminator, determines where a patient can feel. Start at 15mm spacing, bring it down smaller and smaller
normal 2 point discrimination
<6mm spacing
fair 2 point discrimination
7-10 mm spacing
poor 2 point discrimination
11-15 mm spacing
2 point discrimination can help determine what?
can give idea about where a patients sensory function is.
what does a patient need for protective sensation?
perception of one point on 2 point discrimination
moving 2 point discrimination
More functionally correlated
Tests person's quickly adapting mechanoreceptors
Start with 8mm and move to 2-5mm
Easier to feel moving than static
Move along length of nerve longitudinally
normal moving 2 point discrimination
2-5 mm is normal, moving it along the length of the nerve longitudinally.
what to assess for circulation of the wrist/hand
-pulses
-skin color, trophic changes
-allen test
-capillary refill
-edema
-Volumetrics
-figure of 8 method
GIRTH OR CIRCUMFERENTIAL
Landmarks
MP heads, radial head, measured point from landmark
Volumetrics for edema
Fill with room temp water
Must be room temp
Put arm in straight
Spreader bar between 3rd & 4th
Measure the water that comes out
Normal volumetrics
~10 ml >non-dom
MDC 10ml
Swelling volumetrics
30 - 50 ml
figure of 8 method
-Start at ulnar styloid.
-Across volar wrist crease
-Dorsal to 5th MCP
-Around to volar 2nd MCP.
-Dorsal back to ulnar styloid.
functional assessment for hand
-Jebsen-Taylor Hand Function test
-Box and Block Test
-Moberg's Pick up test.
-Purdue Peg board test
-9 hole peg test.
Dorsal glide of the wrist helps with what movement?
flexion
volar glide of the wrist helps with what movement?
extension
lateral glide of the wrist helps with what movement?
UD
medial glide of the wrist helps with what movement?
RD
Joint Play Digits
Fingers/Thumb MP, IP
- Volar glide
- Dorsal glide
- Lateral glide (MCP)
-Distraction
Joint Play Digits Intermetacarpal
- AP rocking
Joint Play Digits
Thumb CMC
- Volar/dorsal
- Medial/lateral
- Internal/external rotations
- Distraction/compression
palpation of wrist/hand
-skin/tissue mobility
-scars
-carpals
-metacarpals
-phalanges
-distal radius and ulna
-tendons
Wrist ligamentous special tests
Varus & Valgus Stress of Finger IP's
Thumb UCL Stress Test
Retinacular test (oblique retinacular lig)
Lunotriquetral Ballotment Test
Watson Scaphoid Shift Test (S-L Instab)
Dorsal Capitate Displacement Apprehension Test
Finger Extension "shuck" test (SL Path)
Piano Keys Test (DRUJ - TFCC tear, triq instab)
Lichtman Test (mid-carp instability)
Sitting Hands/Press Test (TFCC, wrist synovitis)*
Supination Lift Test
Wrist tendon and muscle special tests
Finkelstein's Test
Sweater sign
Central Slip Test ( test for extensor hood rupture)
Bunnel-Littler (joint contract v intrinsic v extrinsic)
wrist nerve special tests
Tinel's Sign (Carpal Tunnel Syndrome)
Flick sign/maneuver
Wrist ratio index
Phalen's (Flexion) test
Reverse Phalen's (extension) test
Carpal Compression Test
Froment's Sign (ulnar nerve)
2-pt discrimination
wrist intra-articular special etsts
Grind Tests (joint degeneration)
wrist outcome measures
DASH
**Not hand specific
CT Function Disability Form
Michigan Hand Outcomes
at minimum, what should an upper quarter screen consist of?
-Patient history outside of the wrist/hand
-AROM C-Spine, shoulder, wrist/hand
-neuroscreen C4-T1
Neuropraxia
Focal conduction block
Motor and proprioception defects
Transient problem
Good prognosis with quick recovery
Axonotmesis
Loss of conduction at injury site, and distal due to compression. Prognosis can be good or poor depending on severity.
Neurotmesis
Loss of conduction at site and distally due to severed nerve.
Requires surgical repair
Pathological nerve injury
-acute nerve ischemia
-segmental demyelination
-axonal disrupt/degeneration
Mononeuropathy
disease affecting a single nerve
Mononeuropathy Multiplex
Pathology of 2+ nerve in 1 extremity
Polyneuropathy
Pathological involvement of multiple nerves usually both motor and sensory involvement
Sensory re-education/hierarchy of return from nerve injury
-Pressure
-Heavy moving tough
-Moving 2 point discrimination
-Static 2 point discrimination
-Light touch
-Vibratory sensibility
-Tactile-gnosis.
general rehab guidelines for nerve injuries
-Repair of lacerated nerve requires 3-4 weeks immobilization
-correct and prevent contractures/deformity
-strengthen as muscle function returns
-adaptation
-pain control/desensitization
Guyon's Syndrome
Ulnar nerve entrapment in Guyon's canal (hand-piso-hamate canal)
Gyon's syndrome MOI
Ganglion > trauma, RA, direct compression
Guyons demographics
Bicyclists, racquet sports, wheelchair athletes
Less common than cubital tunnel entrapment
sensory deficit location with Guyon's syndrome
Palmar, NOT dorsal
motor loss with Guyon's
ulnar intrinsic weakness, deformity in advanced conditions.
Positive special tests with Guyon's
Phalen's/reverse Phalen's, Tinel's @ Guyon's, Froment's, Wartenberg's. Possible Allen's test
what to screen for with Guyon's
Cervical, cubital tunnel, double crush
how long to immobilize after repaired lacerated nerve in guyon's?
3-4 weeks.
interventions for Guyon's
-correct/repair contracture
-strengthen as muscle function returns
-adaptation
-pain control/desensitization
-scar management
-neural glides
Superficial radial nerve palsy
less frequent entrapment, can be from compression at the dorsal-radial wrist by tight wristwatch, or impact at that part of the wrist.
Superficial radial nerve palsy aka
Wartenburg's Syndrome/ Cheilalgia paresthetica