6th cranial nerve
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
where is the 6th nerve nucleus located?
Nucleus: pons – beneath floor of 4th ventricle
- Cavernous sinus + subarachnoid space
describe the course of the 6th nerve
under 4th ventricle in caudal pons.
→ Fibers pass thru pons.
→ Pass thru corticospinal tract.
→ Exit midbrain & enter brainstem at pontomedullary junction.
→ Subarachnoid Space:
Runs upward between pons & clivus.
→ Pierces dura mater:
Runs between dura & skull in Dorello’s canal.
→ Enters cavernous sinus:
Adjacent to internal carotid artery.
→ Enters orbit via Superior Orbital Fissure:
Supplies (LR).
nucleus in the pons, traverses brainstem and leaves to enter the subarachnoid space, makes a vertical ascent over the petrous apex bone over the clivus, enters cavernous sinus
why is cavernous sinus an important anatomic feature for the 6th nerve?
it is adjacent to and wraps around the internal carotid artery - any issues affecting the ICA affect the 6th
briefly joined by oculosympathetic fibres responsible for pupil dilation, issues in this area can cause pupil abnormalities where pupil cant dilate
medial to 5th nerve (trigeminal) V1
possible aetiologies that can affect the 6th nerve?
- Aneurysm
- Trauma
- Tumour
- Arnold Chiari malformation – herniated cerebellum
o Brainstem displacement = 6th n impact
- ↑ ICP= 6th N stretch – FLC – tether at Dorello’s canal = tumour, hydrocephalus, pseudo tumour
- False localising sign – press ↓on sharp petrous apex = flc presents as 6th – but aetiology elsewhere
- Gradenigos S: post middle ear infection – inflammation of petrous apex = pressure in 6th
o Symptoms: hearing loss, facial palsy
- Petrous bone F
- Closed head injury- damages 6th
what is an arnold-chiari malformation?
herniated cerebellum pushes down and pulls tissue along the spinal cord
causes displacement of structures in the brainstem
causing direct effect onto 6th nerve
how does increased intracranial pressure cause a 6th?
6th is stretched and tethered
could be due to mass
can cause a non-localising sign/false localising sign
what is a false localising sign
↑ICP - chiari malformation
6th presses down on sharp petrous apex- due to long course form brainstem & passage thru CS, affecting its function
= false localizing sign - presents as 6th but aetiology elsewhere in brain not along the course of 6th
↑ ICP stretch 6th nerve - tethered at Dorello’s canal = 6th NP horizontal diplopia &esotropia
The lesion causing raised ICP may be remote, such as:
Tumors in the posterior fossa.
Hydrocephalus.
Pseudotumor cerebri.
what is pseudo Gradenigo's
presents in a similr way to Gradenigos
nasopharyngeal carcinoma
how can a petrous bone fracture cause a 6th?
closed head injury damages the 6th
list aetiologies within the CAVENOUS SINUS causing a 6th
vascular lesion e.g. ICA aneurysm
thrombosis, tumour e.g. pituitary, meningioma, infection
Inflammation, ischaemia, trauma - skull fracture
Carotid-cavernous fistula (CCF)
would diplopia be worse at N or D
worse at D, may be phoric at near
Dip - Horiztonal
lateral gaze e.g. left LR 6th CNP, looks worse looking right
what is the general health like in someone with a 6th CNP?
vascular problems tend to occur in those 50+
what would the CHP be like in a 6th nerve palsy
face turn to the affected side e.g. right 6th CNP, turn to the right, eyes move to the left
6th
SOL
trauma
vascular
inflammation
secondary to raised IOP = false localising sign
MS
viral infection
congenital
birth trauma
hereditary
infection - maternal
failure of LR development
acuired
children
SOL
infections -
bacterial - gradinegos syndrome - infection of middle ear - spread to 6th nerve at petrous temporal bone
or viral - benign 6th np - follows infection, viral illness, immunization
INV
CH
vascular issues < 50yrs
H dip - worse in D
eso - AHP
CHP: worse in lat gaze - toward affected side e.g. R6th - turn right
VA
reduced if marked dev
ambylopia develop in unilateral strab
CT
eso D>N
c & s AHP
N - phoric/ sm ET
OM
primary u/a LR = limited abduction
o/a of contralteral & ipsilateral MR
secondary u/a - LR
BV
c AHP - bsv
head trauma - fusion may be lost
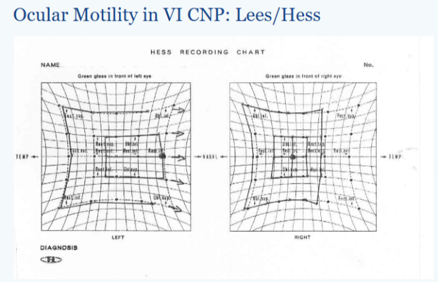
Hess
field of BSV
BSV displaced from affected side
Diplopia
uncrossed - worse in D
mx - congenital/ ac
Management
- Consider false localizing sign
Congenital
- Tx amblyopia
- Occlusion therapy
- Sx – cosmetic
- Teach use AHP
Acquired
- Treat underlying cause
- Wait for spontaneous rec
Botulinum Toxin A:
Inject into MR in recent onset cases.
Prevents contracture, helps restore binocular single vision.
May be combined with surgical transposition.
mx - sugery
Timing:
Performed after ≥6 months of stable deviation.
Non-surgical:
- Prism when dev static
- Occlusion for dip
- BT- to MR prevent contracture
- Bupivacaine
Surgical >6m
- Sm/mod: MR recession only
- LR resection
- Complete palsy
- MR recession + V recuts transposition to LR = Jensen
- ALX – transposition full tendon MR recession
- Residual income – recession of Faden of contralateral MR
Notes:
3 muscle sx = higher ischemia risk.
Botulinum toxin A showed subjective improvement, but no difference in ultimate outcomes in trials.
DD
trauma
raised IOP
decom eso
infntile eso w cross fixaton
mobius syndrome
- Nystagmus block
- Medial wall F