Pediatric Dentistry Final Review (ksolman x ryanef123 collab🤩)
1/386
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
387 Terms

Brodsky:
Surgically removed tonsils
0
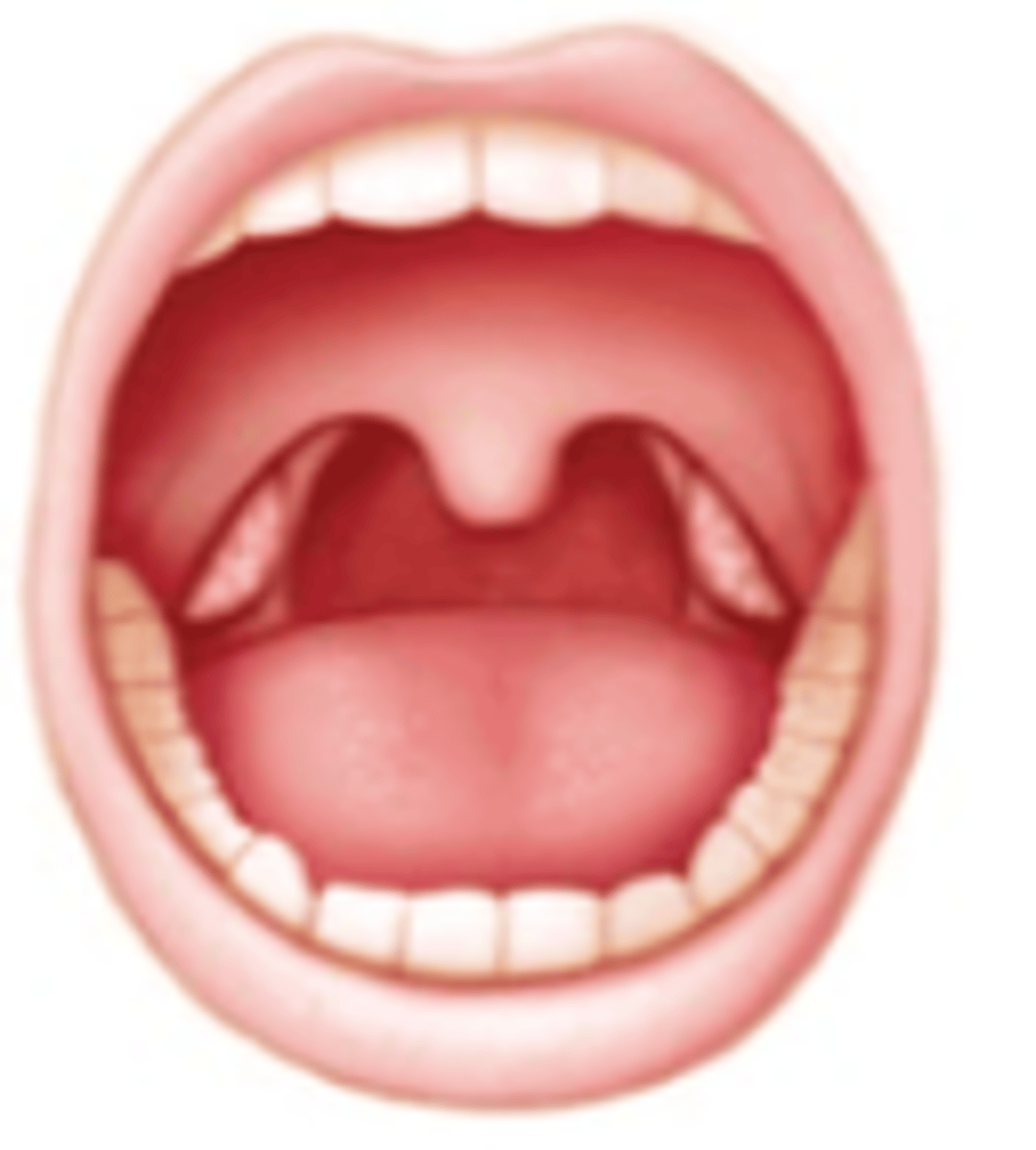
Brodsky:
Tonsils hidden within tonsil pillars
1

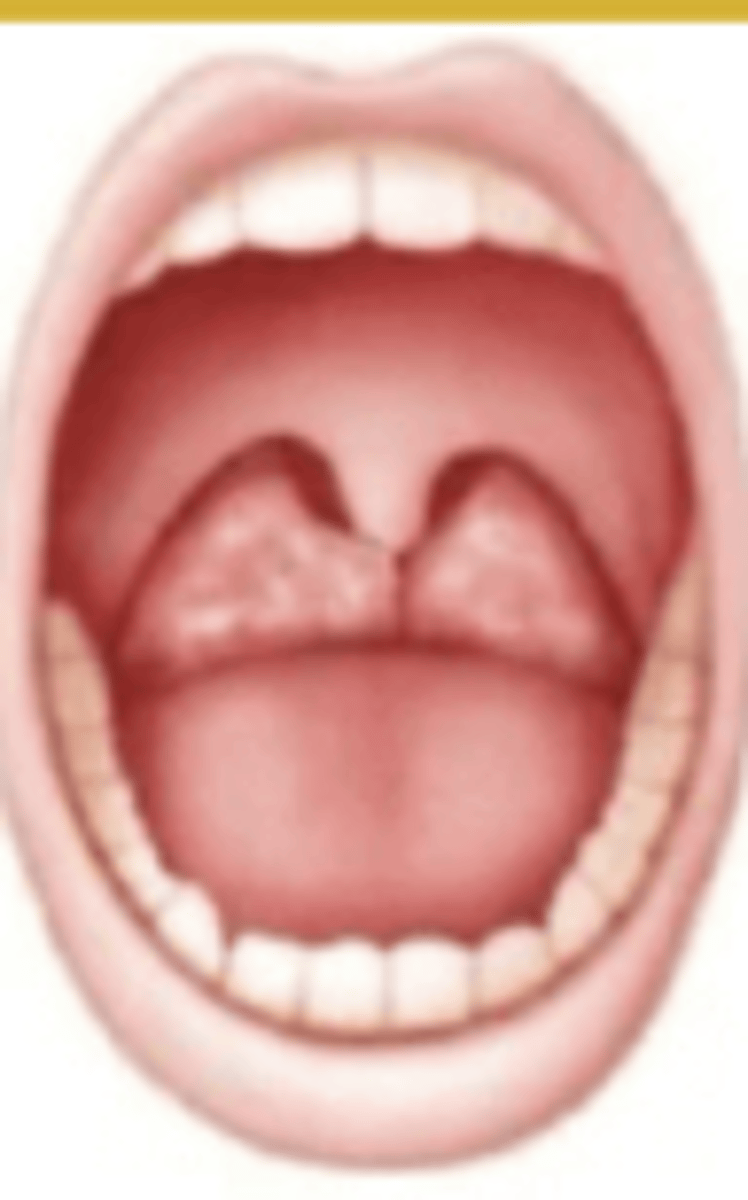
Brodsky:
Tonsils extending to the pillars
2
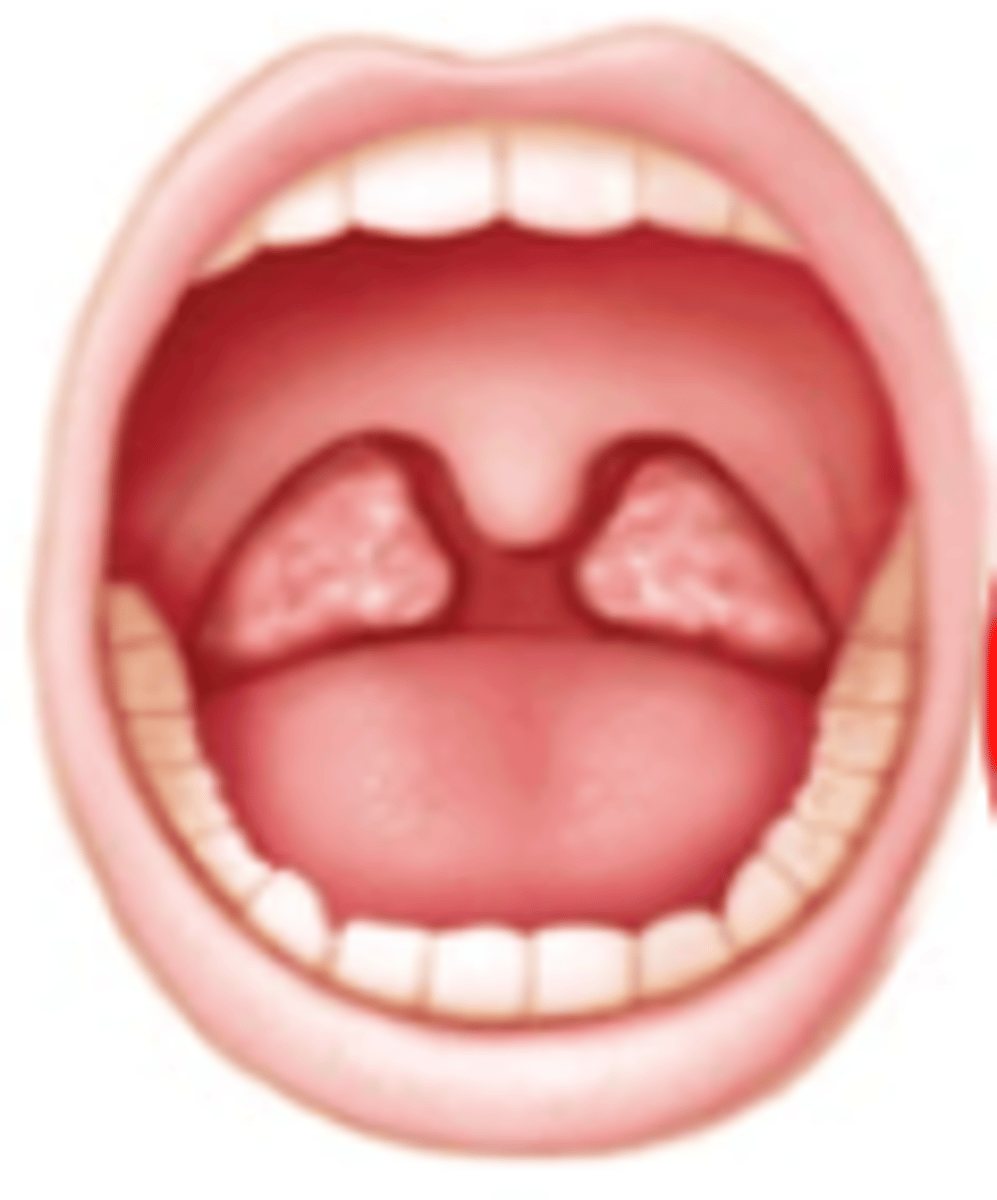
Brodsky:
Tonsils beyond the pillars
3
Brodsky:
Tonsils extend to midline
4
Brodsky grades (_ and _) suggest a narrower airway, which increases the risk of airway obstruction during sedation.
3, 4
Sedation:
A drug-induced state where patients respond to verbal
commands while maintaining stable breathing and heart
function
Minimal sedation
In minimal sedation, children usually only need _________, but if they become moderately sedated, moderate sedation guidelines should be followed.
Monitoring
Sedation:
A drug-induced state where patients can respond to verbal commands or light tactile stimulation.
Moderate sedation
Sedation:
Patients maintain their own airway, and cardiovascular function is typically preserved.
Moderate sedation
Sedation:
Consciousness is usually preserved, but precautions are necessary to prevent deeper
sedation.
Moderate sedation
Sedation:
A drug-induced depression of consciousness where patients are difficult to arouse but respond purposefully after repeated verbal or painful stimulation.
Deep sedation
Sedation:
Patients may have impaired ability to maintain ventilatory function and might need help with airway maintenance, and spontaneous ventilation can be inadequate.
Deep sedation
Sedation:
Cardiovascular function is typically preserved, but there may be a partial or complete loss of airway protective reflexes.
Deep sedation
Patients can transition from deep sedation to...
General anesthesia
A drug-induced loss of consciousness occurs when patients cannot be awakened, even with painful stimulation.
General anesthesia
Sedation:
Their ability to breathe independently is often impaired, requiring assistance to maintain an open airway and possibly the use of positive-pressure ventilation.
General anesthesia
Sedation:
Cardiovascular function may be impaired.
General anesthesia
List the common sedation agents.
Nitrous oxide
Benzodiazepines (diazepam, midazolam)
Opioids (meperidine, morphine)
Antihistamines
Dexmedetomidine
Nitrous oxide is a CNS _________ (minimal CV or respiratory effect).
Depressant
Nitrous oxide has induction time of _ minutes and recovery __ minutes.
5, 10
Anxiolytic, minimal analgesia
Nitrous oxide
Nitrous oxide: __% concentration - open system; nasal hood
20-70
Chronic nitrous oxide exposure/abuse can
occur in dental professionals and may result in ________ ___________.
Peripheral neuropathies
What are these disadvantages of?
Nitrous oxide
Sedative/Hypnotic (Benzodiazepine)
Midazolam (Versed)
Diazepam (Valium)
CNS depression, minimal CV effects occurs with which sedation agent?
Midazolam (Versed)
Diazepam (Valium)
T/F: There is risk of respiratory depression with Midazolam (Versed) and Diazepam (Valium).
True
_________ amnesia occurs with Midazolam (Versed).
Anterograde
Onset vs. working time for Midazolam (Versed)
15 min onset; 20-30 min working time
Oral dose of Midazolam (Versed)
0.5-1 mg/kg to 20 mg max dose
Intranasal dose of Midazolam (Versed)
0.2-0.3 mg/kg to 10 mg max dose
Midazolam (Versed) has _x potency of diazepam.
3-4
What condition:
2% of patients
Agitated and combative
Screaming and flailing
Paradoxical negativism "angry child"
Paradoxical negativism "angry child" is associated with which sedative?
Midazolam (Versed)
Onset vs. working time for Diazepam (Valium)
45-50 min onset; peak 60 min with 45-60 min working time
Dose of Diazepam (Valium)
0.2-0.3 mg/kg orally with max dose 15 mg as single agent or 10 mg in combo with other agents
Contraindication for Diazepam (Valium)
Narrow-angle glaucome
Diazepam (Valium) half life = ?
20-40 hours but can be extended in some patients because of an active metabolite
What pediatric reversal agent do we use?
Flumazenil (benzodiazepine)
Typical pediatric dose of Flumazenil (reversal agent benzodiazepine)
IV: 0.01 mg/kg to 1 mg max
IN: 0.04 mg/kg to 0.2 mg max
Which modality:
Oxygenation (SpO2)
Late indicator of ventilatory
problems
Pulse oximetry
Which modality:
Heart rhythm
Detects arrhythmias
ECG
Which modality:
Ventilation (EtCO2)
Early indicator of hypoventilation/apnea
Capnography
Which modality:
Perfusion trend
Cuff size matters
Noninvasive BP
The younger the age, the ____ accepting of sedation.
Less
Sedation is ____ likely to be successful for child with cognitive impairment.
Less
#1 factor influencing sedation outcome
Child's behavior (temperament)
Socialization: child with few limits or boundaries can be "_______" = not a good candidate for sedation
Difficult
A powerful indicator of a child's response to dental treatment
Temperament
Behavioral style of an individual while interacting with the surroundings
Temperament
Both ___ and ___________ seem to act as predictors of child behavior in the dental setting.
Age, temperament
Frankl:
Definitely positive, good rapport, interest in dental procedures, laughs and enjoys
4, ++
Frankl:
Positive, accepts treatment but may be cautious or reserved, follows directions
3, +-
Frankl:
Negative, reluctant, timid, uncooperative
2, -+
Frankl:
Definitely negative, refusal of treatment, defiant, unable to cooperate
1, --
Most effective for children with
communicative/interactive ability, can be used with any child
Tell-show-do
When is tell-show-do contraindicated?
Hearing impaired
Rewards desired behavior
Best when immediate-concept
Requires consistency and avoid rewarding undesirable behavior
Realization that the desired behavior may be less than totally desired but is still a positive step to be recognized
Positive reinforcement
Attention is directed from dental procedure
Affects pain perception
Dental applications: videogames, headphones, storytelling
Distraction
Controlled alteration of voice to direct behavior
-Volume
-Tone
-Pace
Study of Loud Voice control punishment
Highly effective in reducing disruptive behaviors
Voice control
Greenbaum et al 1990 - Rated voice control as __________ by parents.
Unacceptable
Indicated in any patient who has the potential to be cooperative
Parental absence/presence
Most common technique of parental absence/presence involves...
Previously cooperative child who becomes uncooperative and practitioner asks parents to leave operatory until child becomes compliant
When is parental absence/presence contraindicated?
Parents unwilling/unable to extend effective support
Child unable to understand that parent's presence is contingent on cooperation
ID the basic behavior guidance technique:
- Patient observes another patient exhibiting cooperative behavior during tx
- Can be through live model or video
Direct observation/modeling
What are the three advanced behavior guidance techniques?
1. Protective stabilization
2. Sedation
3. General anesthesia
Informed consent should be presented in a language easy for parents' understanding and should address: (3)
Risks
Benefits
Alternatives of behavior guidance
T/F: Advance Behavior Management requires a separate informed consent.
True
How do we prevent traumatic dental injuries?
Custom pressure-laminated mouthguards have the best protective qualities (multiple layers)
What are the thorough diagnostic steps for managing traumatic dental injuries? (3)
1. Medical history
2. Neurological evaluation (important to evaluate cranial nerves, nausea, loss of consciousness) they require immediate referral
3. Clinical Exam
• Radiographs and Photographs
• Indicators of Cranial Fracture (Battle Sign, Racoon Sign)
What signs are indicators of cranial fracture?
- Battle sign
- Raccoon sign
Uncomplicated or complicated:
Enamel/dentin
Uncomplicated
Uncomplicated or complicated:
Pulp involvement
Complicated
Treatment for uncomplicated trauma
Radiograph, resin restoration
Treatment for complicated trauma
Open apex: preserve pulp vitality CaOH2
Matural apical development: RCT
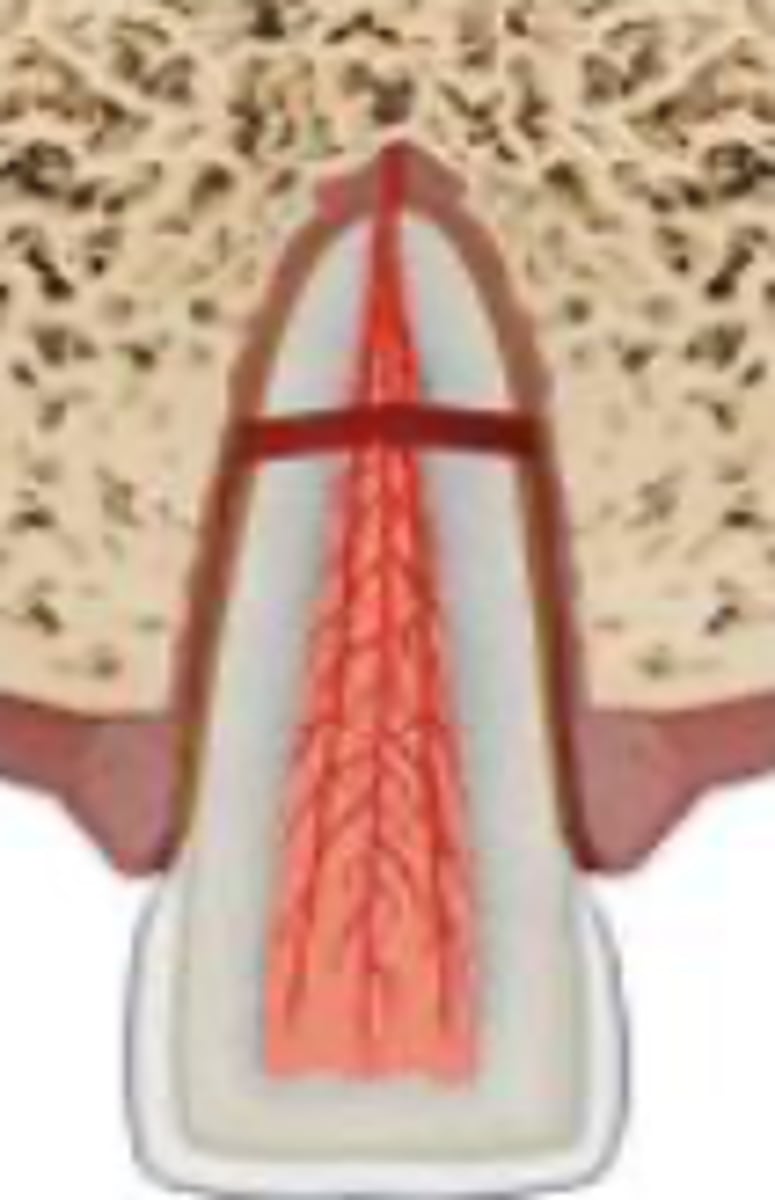
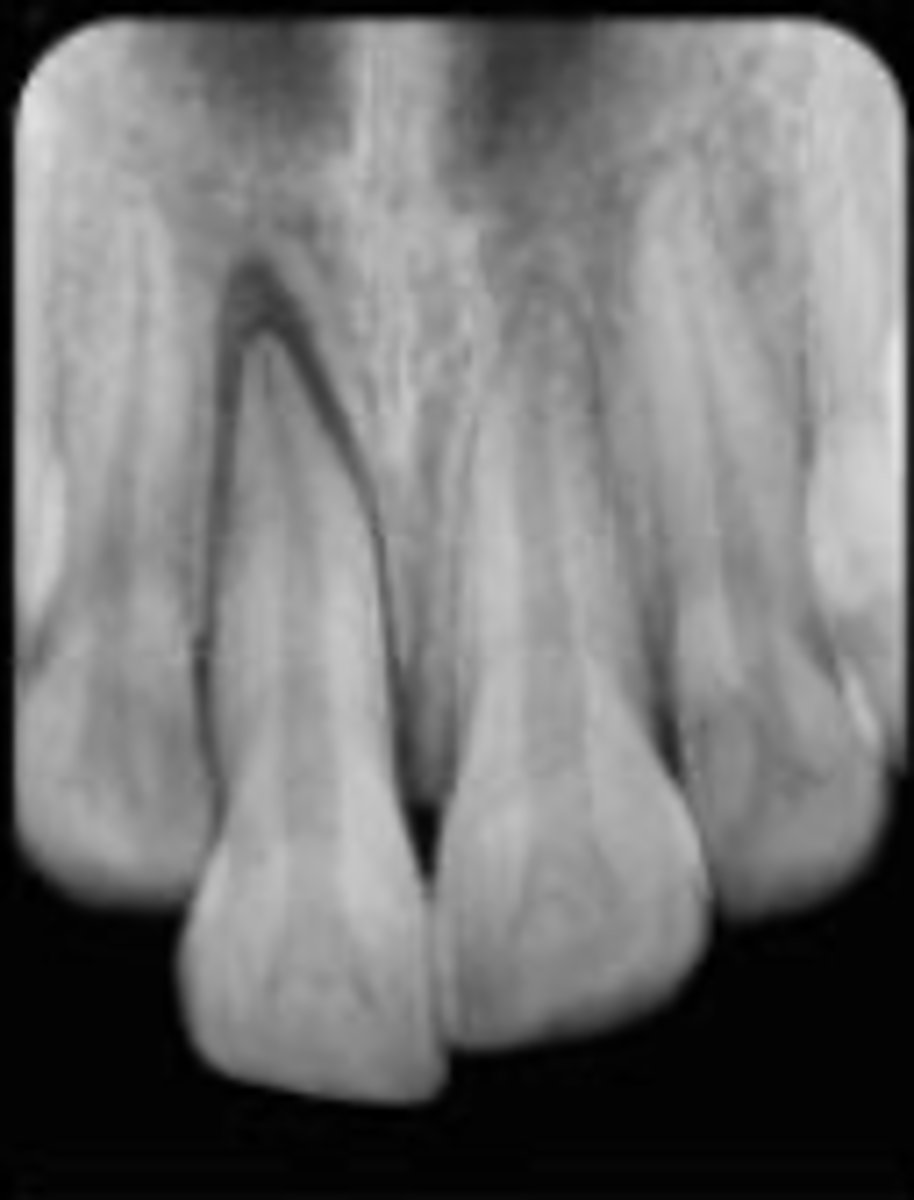
Which trauma:
Coronal segment mobile and displaced
Root fracture
Which trauma:
Tender to percussion
Bleeding from gingival sulcus
False negative initially
Root fracture
Which trauma:
Crown discoloration (red, gray)
Root fracture

Which trauma:
Root fracture
Which trauma:
Root fracture

Which trauma:
Root fracture
For root fracture:
Horizontal plane fracture: ________ third fractures (radiograph PA 90)
Cervical
For root fracture:
Oblique plane fracture: _______ third fractures (radiograph occlusal)
Apical
A patient presents with a root fracture. How do you go about treating them if it's displaced?
Reposition ASAP
Verify position with radiographs
Stabilization flexible splint 4 weeks (apical and middle third)
A patient presents with a root fracture. How do you go about treating them if the root fracture is near the cervical area?
Stabilization with flexible splint (up to 4 months) longer period is beneficial
A patient presents with a root fracture. How do you go about treating them if it's necrosed?
RCT
Monitor healing of root fractures for up to ...
1 year
On mature teeth with root fracture, repositioning of fragment increases frequency of...
Hard tissue healing
On immature teeth with root fracture, there is favorable...
Pulp revascularization, high repair for young cells, healed even sub-optimal repositioning
Which trauma:
Tender to touch or tapping
No displacement or mobility
Sensibility test +
Concussion
Radiographic findings of concussion and subluxation
None
A patient presents with concussion. How do you treat them?
Monitor pulp condition for a year
Which trauma:
Tender to touch or tapping
No displacement
Increased mobility
Bleeding from gingival crevice
Sensibility test -
Subluxation
How do you treat a patient with subluxation?
No treatment normally
Stabilization for patient comfort if excessive mobility
Monitor normal pulpal response
Both concussion and subluxation are tender to touch or tapping. How do you tell the difference?
Subluxation has mobility and negative sensibility testing
Which trauma:
Tooth appears elongated
Excessively mobile
Sensibility test -
Extrusive luxation
Which trauma:
Increased PDL space apically
Extrusive luxation

Which trauma:
Extrusive luxation
Which trauma:
Extrusive luxation