Foundations of Occupational Therapy Exam 1 Study Guide
1/86
Earn XP
Description and Tags
A Study Guide for AHU's OTA and MOT students
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
87 Terms
Moral Movement/Treatment
In the 1800s, The philosophy that all people, from the most challenged to sane people, are entitled to consideration and human compassion. Before this, the insane were confined and abused
Arts and Crafts Movement
In reaction to expanding tools and machines, this contingency of proponents developed in the 20th century. This allowed patients to experience pleasure in making practical and beautiful items for everyday use. Proponents believe this approach made the patient connected to their work and therefore healthier
What is NSPOT?
National Society for Promotion of Occupational Therapy
NSPOT changed to which name now?
American Occupational Therapy Association AOTA 1921
In World War I, veterans returned with disabilities that required training. Who helped them return to work?
Reconstruction Aide
World War II created more demand for OTRs. In the 1950s, this medicine changed the practice of occupational therapy called neuroleptic drugs. This ability led to to this treatment to control behaviours through medication. This breakthrough led to this mental-health policy and treatment approach:
What is Deinstitutionalization Plan?
In the 1950s, growing demand for occupational therapy led to the creation of this role:
What is Certified Occupational Therapy Assistant (COTA)
How long was the OTA program for? Explain the changes overtime:
A 3 month course in psychiatry, eventually expanded towards general practice in 1960s. Initially based in hospitals, now in universities and technical schools.
Features Level I and II fieldwork
At the associate or bachelor level
How many names did the first directory of OTAs had in 1961, according to AOTA:
553
In the 1960s, occupational therapy went TOWARD this approach due to advances in technology and connection more with medicine:
Technical/Biomechanical, Medical, and reductionistic approach
The 1970s and 1980s saw a period of innovation in technology. OT practitioners still worked on reductionist approach when working with clients in communities. The 1990s brought a change back to this approach in OT:
Holistic (whole person) / Occupation-based approach

I am responsible for creating in what would become the Moral Treatment Movement. I introduced “Work Treatment” for the “Insane”. Using occupation to divert my patients away from their emotional disturbances, and towards improving their skills. I utilise physical excercise, work, music, and literature in my treatments.
Philippe Pinel
I have seen terrible conditions at an asylum in York. I have established a retreat there (York Retreat) to share my outrage and prevent anyone from being treated poorly ever again. I want the environment there to be like that of a family in which my patients are given kindness and consideration.
William Tuke
Pinel and Tuke are responsible for this idea:
Moral Treatment Movement
I have learned about the Moral Treatment Movement and want to bring this practice over to the United States:
Dr. Benjamin Rush
We lead the Arts and Crafts movement. We disagree with production of items by machine. We want to restore the ties between beautiful work and the worker by emphasising on using your own hands to make and connect with your work, and therefore much healthier. This high-standards is not found in mass produced items.
John Ruskin and William Morris

I am the “mother of occupational therapy”.
I began as a student in social work. Attended courses in 1908 at Chicago School of Civics and Philanthropy, affiliated with Hull House and Jane Adams. I worked in various hospitals in Michigan and New York.
At the Henry Phipps Psychiatric Clinic of Johns Hopkins Hospital, I developed this area of work which I call HABIT TRAINING. I organised the first professional school for OT practitioners at Henry B. Flavill School of Occupations.
I was AOTA’s executive secretary for 14 years.
Eleanor Clarke Slagle

I am the “father of occupational therapy”
I’m a psychiatrist that treats psychiatric patients.
I was hired as an assistant staff physician at Sheppard Asylum (you call it Sheppard and Enoch Pratt Hospital).
I read about Pinel and Tuke’s treatment programs and wanted to apply a similar program at the asylum.
In the 1910s, the hospital introduced a regimen of crafts for the patients, which provided staff with necessary medical procedures and a structured environment. Patients are expected to participate in those rehab in the workshop though.
I have written on the value of occupation for treatment.
I published Occupational Therapy: A Manual for Nurses
I served as NSPOT’s (AOTA) Treasurer and President, and edited the journal for 21 years.
William Rush Dunton Jr.

I am a designer and arts and crafts teacher from Berkeley
I am the Director of Occupations at the New York State Department of Public Charities
I demonstrated how morally uplifting occupation is. It improves mental and physical state of patients and residents at public hospitals, almshouses. These individuals can contribute to their self support
I joined the nursing faculty in Columbia University, teaching OT there.
High Standards, train competent practitioners, not more practitioners.
Susan Cox Johnson

Consider me one of the first occupational therapists
I was a nursing instructor involved in Arts and Crafts Movement and trained nurses in the use of Occupations.
In 1905, I worked at the Adams Nervine Asylum. I supervised the nursing school, developed the occupations program, and conducted postgrad courses for nurses.
I wrote the first known book about OT: Studies in Invalid Occupations
I served as chair of the Committee of Teaching methods.
Susan Tracy
I am a physician that graduated from Harvard Medical School
I worked with debilitated patients, providing medical supervision of crafts for the purpose of improving their health and financial independence.
In 1904, I established a facility in Marblehead. Where patients with neurasthenia (removed from DSM-5, categorised by physical pain, emotional distress, exhaustion in people who lived and worked in cities) worked on arts and crafts as part of treatment.
I developed the “WORK CURE”. Features arts and crafts activities, start with participating on limited basis from bed, and increase gradually with each level of activity until you progress to the workshop, which you can explore looms, ceramics, and other crafts.
This is an alterative to “REST CURE” where you simply rest and most physicians prescribe that, especially as gender roles started to shift, mainly for women as they entered work and education at higher rates.
I got $1,000 to study treating neurasthenia by progressive and graded manual occupation.
Herbert Hall
I am a resourceful architect that studied in London under the tutelage of William Morris (the Arts and Crafts Movement guy in UK)
I incorporated the Boston Society of Arts and Crafts
I have personally experienced several disabling conditions: tuberculosis, foot amputation, paralysis of my left side of the body. This encouraged me to improve the plight of convalescent individuals, and improve their quality of life.
In 1914, I opened the Consolation House in Clifton Springs, New York, USA. Occupation is the method of treatment there using arts and crafts as the form.
I studied rehabilitation courses that were available at the time and networked with people dedicated to reforming conditions at asylums, many of them influenced by Moral Treatment Movement.
I made contact with Eleanor Clarke Slagle, William R. Dunton Jr., Susan Cox Johnson, Susan Tracy
George Edward Barton
I am a good friend of George Barton.
I’m an architect and teacher
I established a presence for OT in vocational rehab and tuberculosis treatment.
I was appointed vocational secretary of the Canadian Military Hospitals Commission.
I developed a system of vocational rehab for disabled Canadian veterans of World War I, constructing institutions for individuals with physical disabilities.
I included workshops for OT there.
I encouraged OTs to capitalise on USA’s Vocational Rehabilitation Act passed in 1920.
I became interested in tuberculosis, after seeing young World War I disabled men having this disease.
I designed hospitals in Canada and USA for treating TB patients.
Thomas Kidner
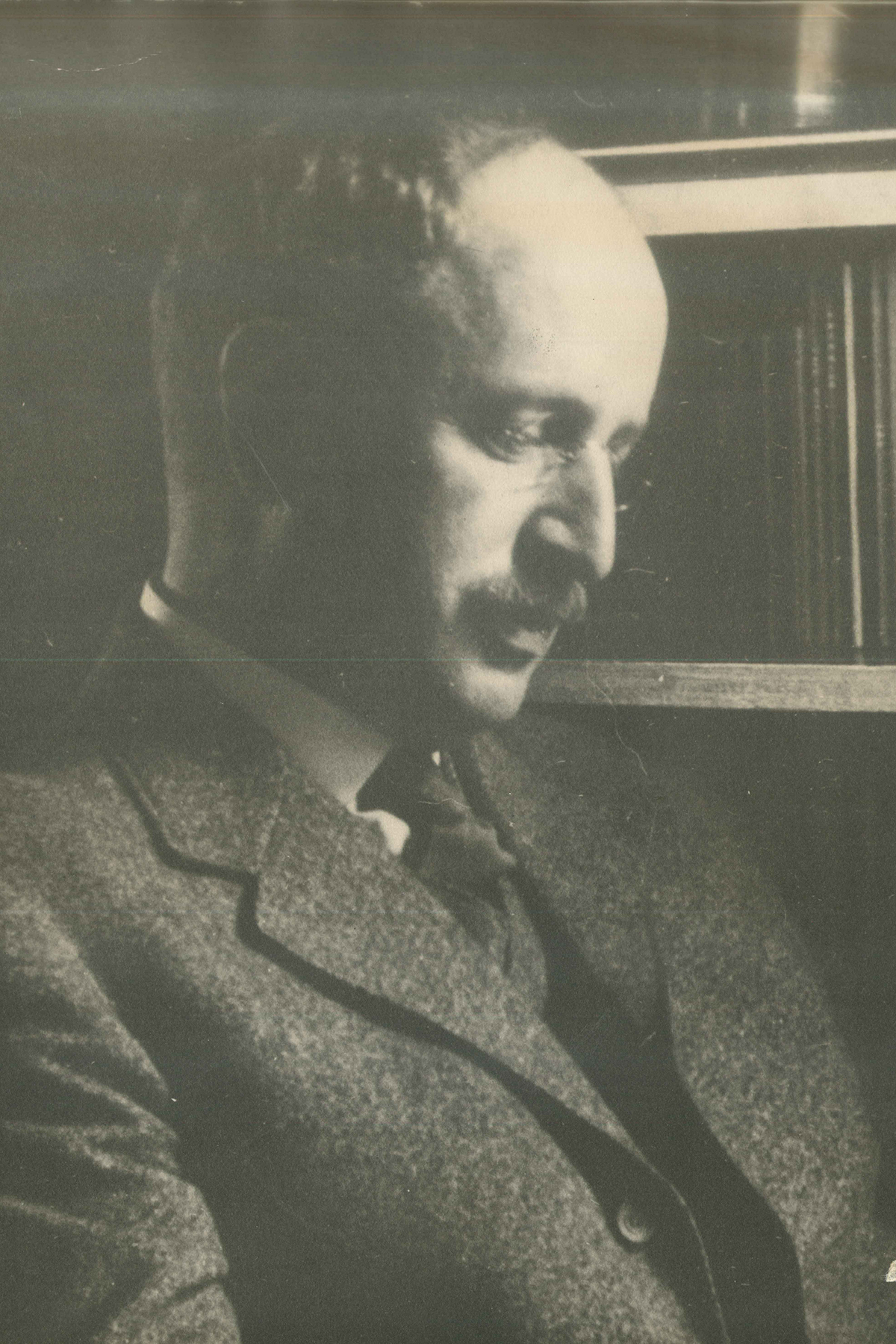
I am a Swiss physician that became a professor of psychiatry at Johns Hopkins University.
I committed myself to a HOLISTIC perspective and developed a psychobiological approach to mental illness.
Each individual should be seen as a complete and unified whole, not a merely a series of parts or problems to be solved (REDUCTIONIST approach)
I believe that providing a person with the opportunity to participate in purposeful activity promoted health.
At the fifth annual meeting of NSPOT in 1921 in Baltimore, I delivered my keynote address.
“Philosophy of Occupational Therapy” published in the organisation’s first journal in 1922. I emphasised developing habits to achieve a balance between work, play, rest, and sleep.
Adolf Meyer
Dunton’s Principles of Occupational Therapy:
Any activity should have a cure as its objective
The activity should be interesting
There should be a useful purpose other than merely gain the patient’s attention and interest
The activity should preferably lead to an increase in knowledge on the patient’s part
Activity should be carried on with others, such as a group.
The occupational therapist should make a careful study of the patient and attempt to meet as many needs as possible through activity
Activity should cease before the onset of fatigue
Genuine encouragement should be given whenever indicated
Work is much to be preferred to idleness, even when the end product of the patient’s labour is of poor quality or is useless.
Which key concepts and trends have persisted in history of Occupational Therapy?
Moral Treatment: everyone is entitled to consideration and human compassion
Arts and Crafts: experience pleasure in making practical and beautiful items for everyday use
Activity: help patients return to their occupations, and reengage in their daily habits to restore health
Holistic manner: Treat the whole person, not a series of parts
Advocate for human rights
This practitioner is the professional stage of occupational therapy. They evaluate, formulate individualised treatments, treat patients, and develop theory and research for it. Requires a Master or doctoral degree since 2007 (in USA). Currently 173 programs in USA
Occupational Therapist Registered (OTR)
History of OTR training
Back then only 8 OT schools in 1921.
AOTA standards was adopted in 1923, and included prerequisites for admission, length of courses, and content
Training was at least 1 year - 8-9 months of medical and craft training, and 3-5 months of clinical work in hospitals
Features Level I and II fieldwork
Now, OTR programs are 2-3 years long and are at a master (MOT or MSc in OT) or doctoral (OTD) as of 2007 (USA only), before 2007 it was a bachelor level in USA
Need to take a board exam by National Board for Certification of Occupational Therapy (NBCOT)
This practitoner is the practical or technical stage of occupational therapy. Under supervision and mentorship, they treat patients and assist in evaluations but cannot make evaluations themselves. Requires an associate or bachelor degree. Currently 222 programs in USA.
Certified Occupational Therapy Assistant (COTA)
World War II and 1940s history of OT
WWII created a new demand for more OT’s, but they wanted them to graduate from an accredited school (18 months).
Emergency courses had to be implemented to quickly train more OT’s. The number of employed practitioners grew quickly.
Black OT’s began to diversify the field beginning in the 1940’s.
In 1945, completion of an exam became a requirement to register as an OT practitioner
Post World War II: 1950s-1960s
Continued shift away from the generalist approach to one of specialization in physical rehabilitation.
US was still struggling with a history of discrimination against disabled people.
The Civil Rights Era was alive and well.
New Drugs and Technology
Neuroleptic drugs (tranquilizers and antipsychotics) in the mid 1950’s changed the course of psychiatric treatment.
Many people were discharged thanks to chemical control, and a national deinstitutionalization plan was implemented.
Community mental health programs were developed, along with innovative technologies such as splinting materials, wheelchairs, and prosthetics/orthotics.
Rehabilitation Movement
1942-1960. VA hospitals increased in size and numbers to handle the casualties of war.
More individuals were living with disabilities as a result of the polio epidemic and new medical procedures and antibiotics that were saving lives.
1970s through 1980s
Prospective Payment System
Social Security Amendments were signed into law by President Reagan in 1983. Up to this point, hospitals were reimbursed based on the actual cost of services provided.
With the implementation of the Medicare Prospective Payment System, a schedule was established showing what the government would pay for each inpatient stay of a Medicare beneficiary.
Advances at AOTA
Lobbying for the interests of OT became a function of AOTA during the 70s and 80s.
In 1986, they were no longer responsible for board certification – instead, one was certified through the National Board for Certification in Occupational Therapy.
State Regulation of Occupational Therapy
State licensing to ensure quality OT services began in 1975.
A Return to the Roots of the Profession: Occupation
Gary Kielhofner: Return to Occupation
Model of Human Occupation (MOHO)
Vision 2025
“Occupational therapy maximizes health, well-being, and quality of life for all people, populations, and communities through effective solutions that facilitate participation in everyday living.”
This USA federal legislation established a program of vocational rehabilitation for soldiers disabled on active duty:
Smith-Sears Veterans Rehabilitation Act / Soldier’s Rehabilitation Act (1918)
This USA federal legislation provided vocational rehabilitation services to civilians with physical disabilities:
Smith-Fess Act / Civilian Vocational Rehabilitation Act (1920)
This amplified the demand for occupational therapy services even further. Persons 65 years or older, or those who are permanently disabled receive assistance in paying for their health care
Medicare (1965)
This USA federal legislation mandated that state agencies provide disabled persons with programs to meet vocational goals.
Examples include: physical restoration, counseling, education preparation, work adjustment, vocational training.
Prohibited discrimination in employment or in admissions criteria to academic programs solely on basis of a disabling condition.
Rehabilitation Act (1973)
This USA federal legislation established the right of all children to a free and appropriate education, regardless of handicapping condition
Education for All Handicapped Children Act (1975)
This USA federal legislation extended the provisions of Education for All Handicapped Children Act to include children from 3-5 years of age and initiated early intervention programs for children from birth to 3 years old.
Handicapped Infants and Toddlers Act (1986)
This USA federal legislation required school districts to educate students with disabilities in the least restrictive environment (LRE), and requires states to ensure that students with disabilities are educated with their nondisabled peers to the maximum extent.
Individuals with Disabilities Education Act (IDEA)
This USA federal legislation addresses the availability of assistive technology devices and services to individuals with disabilities:
Technology Related Assistance for Individuals with Disabilities Act (1988)
This system delineated what the government would pay for each inpatient stay of a beneficiary using descriptive categories according to the individual’s diagnosis, called diagnosis-related groupings (DRGs)
Medicare Prospective Payment System (PPS)
This USA legislation provides civil rights to all individuals with disabilities and guarantees equal access to and opportunity in employment, transportation, public accommodations, state and local government, and telecommunications with individuals with disabilities
Americans with Disabilities Act (1990)
This USA legislation reduced Medicare spending, create incentives for development of managed care plans, encourage enrollment in managed care plans, limit fee-for-service payment and programs. It capped payments at $1,500, and forced OT practitioners to broaden their horizons and look beyond typical areas of practice. This included work in community based programs.
Balanced Budget Act (1997)
This USA legislation was enacted to address the rising cost of health care, shortage of providers, lack of insurance available for many Americans. Intention is to lower government spending on health care by decreasing emergency room visits and increase preventative care.
Affordable Care Act (2010)
Grounded in philosophy that all people, even the most challenged, are entitled to consideration and human compassion
Moral Treatment
Allowed people to experience pleasure in making practical and beautiful items for everyday use.
Arts and Crafts
Define the philosophy of OT that defines the nature of the profession, guide the action of practitioners, determine the profession focus and process.
Importance of occupation to health and well-being
Recognition of occupational problems as the focus of therapy
Importance of a client centered approach.
The summary of the philosophical base of Occupational Therapy
OT philosophy is based on the value of engaging in desired life activities (occupations).
“The use of occupation to promote individual family, community, population health is the core of occupational therapy practice, education, research, advocacy.”
People have the need and right to participate in a constellation of meaningful occupations that provide them with a sense of identity and promote quality of life, health, and wellness
OT practitioners enable people to engage in those desired occupations within their unique circumstances, environments, and abilities
Occupation is both a means (“doing” occupations to enable participation) and an end in therapy (outcome of occupational therapy intervention)
Participation in one’s occupations promotes health and wellness, remediation or restoration, health maintenance, disease and injury prevention and compensation and adaptation.
Assumptions and Beliefs Central to Occupational Therapy
People participate in a variety of occupations that are meaningful to them and provide them with a sense of identity.
Occupations are classified as activities of daily living, instrumental activities of daily living, self-care, education, work, play and leisure, sleep and rest, and participation in social activities
Everyone has an innate need and right to engage in their chosen occupations
Personal and environmental contexts affect the requirements and expectations of occupations
A variety of factors influence occupational performance
The focus of occupational therapy is to enable people to engage in desired occupations
Occupation is both a means and the product of therapy
Occupation promotes health, well-being, and quality of life for all people
Occupational therapy values people and embraces diversity, equity, inclusion, justice
Every person has the potential for change
Client-centred care is essential to understand, create, implement occupational therapy intervention
Values the individual person, their interests and needs
Consider the person first, valuing potential of humans
Support the importance of diversity, inclusion, equity, justice for all
Humanism
Humans are in the process of becoming and have freedom to think, feel, and act
OT’s focus interventions based on client emotions
Emphasis on understanding the clients narrative and life experiences, as people become the things that they do
Existentialism
A practical philosophy that works in a real-world situation
People learn best by applying experiences to problems as they arise
Focuses on actions and accomplishing goals by addressing them realistically
Consider the practical aspects of therapy (finances, resources, timeline)
Pragmatism
How various parts relate to a larger structure
Evolved from the medical model that emphasizes addressing the deficient parts of the system
OT’s using this model believe that addressing the limitation (strength, endurance, ROM, sensation) leads to improvement in one’s daily life
This concept moves away from the value of occupation-based intervention
Structuralism
A person’s values, interests, motivations
Volition
Focus of Occupational Therapy
The focus of OT intervention is enabling people to engage in their desired occupations.
Occupation as a means refers to using a specific occupation to bring about a change in the client’s performance. What are some examples of this?
Occupation as an end refers to the desired outcome of the intervention process
Occupation-based intervention – using engagement in occupation as the therapeutic agent of change. It allows clients to integrate a variety of skills, movements, and sensations within the natural context, which promotes motor learning and generalization.
Core Concepts of Occupational Therapy
Humans are viewed holistically
Humans are viewed as active beings
The focus is on areas of occupation
Human learning involves experience, thinking, feeling, and doing
Occupation is both a means and an end (see box 3.3, page 44)
Every human has the potential to adapt
Based on humanism
The client, the family, and significant others are an active part of the process
Contribution of occupation to health
Occupation supports physical health by keeping people active, mobile, and engaged in routines that promote strength, endurance, and balance (e.g., exercise, cooking healthy meals).
It supports mental health by reducing stress, preventing isolation, and promoting purpose and self-expression.
Participation in occupation can also prevent illness and aid recovery, because structured activity promotes healthy habits and routines.
Contribution of occupation to well-being
Occupation provides a sense of identity and purpose—people often define themselves by what they do.
It helps maintain emotional balance, since engaging in meaningful activities fosters joy, satisfaction, and resilience.
It nurtures social connection, as many occupations involve interaction with family, friends, and community.
Contribution of occupation to quality of life
Occupation enables individuals to live independently and manage daily activities, which improves dignity and autonomy.
It contributes to life satisfaction by allowing people to pursue interests, roles, and goals that matter to them.
Occupations help people adapt to change or disability, ensuring they can still participate in meaningful life roles even with limitations.
Occupation as a means
Using occupation to bring about change
Example: Using LEGO models to increase fine motor strength, bilateral coordination, visual-motor integration (primary goal is hand therapy outcome)
Example 2: Playing violin, French horn, or the piano in music sessions to improve upper-extremity range of motion, motor planning, attention span (violin and piano), breath and trunk control (horn)
Example 3: Going to the art museum to meet people and initiate conversation (improve socialisation skills)
Example 4: Play basketball, football (or soccer), or swimming to improve gross-motor coordination, balance, endurance, and socialisation skills
Occupation as an end
Engaging in the occupation is the goal of the intervention
Example 1: To resume LEGO hobby building as a leisure pursuit, or a architect planning project, designing and displaying completed works with friends and family (focuses on adapting the environment, selecting ergonomic tools, pacing)
Example 2: To perform in an orchestra, recital, or compose music as a leisure, or occupation.(addresses endurance, adapted instrument grips, seating, and modify music scores)
Example 3: Going to the art museum as a leisure activity
Example 4:To compete in recreational leagues, swim laps independently, compete in national or international tournaments, or coach a team
Reductionistic
Reduced to separately functioning body parts
Professionals specialise in specific areas
Isolate, define, treat body functions to focus on a specific problem
Holistic
The core concept of Occupational Therapy
Emphasise the parts working together in harmony, and the whole being
Focus on the interaction of the biological, psychological, sociocultural, spiritual elements
If one area is affected, everything is affected (the whole person)
Altruism
Unselfish concern for the welfare of others, showing care, dedication, responsiveness, understanding
Equality
Treating all people equally, respecting everyone’s beliefs, values, lifestyles
Freedom
Individuals right to exercise choice, independence, initiative, self-direction
Justice
Providing services to those in need of them and maintaining a goal-directed and objective relationship with clients, abiding by all laws
Dignity
Inherent value and worth of humans, showing empathy and respect
Truthfulness
Behaviour that is accountable, honest, and accurate. Maintaining professional competence. Accurate documentation
Prudence
Demonstrating sound judgement, care, discretion, dedication to continued learning, reflection, self-awareness
Supportive
“Promote a comfortable environment while providing stimulation or solace” to those who “cannot benefit from the other two types of activities”
Usually severely cognitively or physically impaired or cannot participate in group
Example: Sensory stimulation (touch, sound, visual) etc.
Maintenance
Provide opportunities to maintain physical, cognitive, social, spiritual, and emotional health
Empowerment
Emphasize the promotion of self-respect by providing opportunities for self-expression, choice, and social and personal responsibility
Focus on opportunities for redevelopment of a sense of purpose in one’s life
Ability to understand the needs and emotions of one’s own culture and the culture of others
Cultural sensitivity
Culture
Customs, beliefs, activity patterns, behavioural standards, expectations accepted by the society in which the client is a member
One’s ability to be sensitive and work with people from other cultures
Cultural competence
Reflecting on knowledge and understanding of different cultures
Cultural awareness
Strategies to develop cultural sensitivity
1. Provide individualized, culturally centred interventions
2. Commit to lifelong cultural competence
3. Collaborate with the patient and their families and communities
4. Expand and broaden cultural knowledge and relate it to occupational therapy
5. Build culturally responsive communication skills
6. Be open minded, practice ongoing self-reflection
Culturally responsive care
Equitable, empathetic, contextualised care that is in sync with shared experiences and meanings of diverse people
Contexts in occupational identity, justice etc.
Environmental or personal factors that influence the person’s choices, opportunities, resources, and subsequent occupational engagement
Environmental: physical, social, virtual
attributes unique to the person that make them who they are
Five constructs of culturally responsive care
1. building cultural awareness
2. generating cultural knowledge
3. applying cultural skills
4. engaging in culturally diverse situations
5. explore multiculturalism
Everyone being able to access their desired occupations throughout life
Occupational Justice
A sense of who you are as a person
Occupational Identity
When persons do not have access to certain occupations
Occupational Depravation
Interprofessional Education (IPE)
Important part of OT education. Involves professionals to collaborate and work closely together for the best interest of the client.
Important part for students, exposes them to global experiences for interprofessional learning on health issues.
They include unique classes, workshops, seminars, interprofessional experiences emphasising global topics. Students learn about the culture.
May allow for international fieldwork placements
This organisation whose mission is to “promote and advance occupational therapy and demonstrate its relevance and contribution to society around the world”
World Federation of Occupational Therapists